Article Text

Abstract
Background There is little information on the earliest changes in motor unit (MU) physiology in amyotrophic lateral sclerosis (ALS) and the development of the classical neurophysiological features of ALS over time.
Objective We studied the earliest abnormalities in MU physiology in ALS and changes over time.
Design Observational, cross-sectional and longitudinal study.
Population and methods We studied the tibialis anterior (TA) muscle in three groups of subjects; 73 patients with ALS, 10 with benign fasciculation and 37 healthy control subjects. In the ALS group, 61 had normal strength in the TA muscle and 12 had TA muscle strength of 4 on the medical research council scale. In all subjects we evaluated the presence of fasciculation potentials (FPs) and fibrillation/sharp-waves (fibs-sw), and quantified MU potentials (MUPs) and jitter. Twenty-six ALS patients with TA muscle of normal strength were investigated in serial studies.
Results FPs were recorded in TA muscles (medical research council 5) of 21 ALS patients with normal MUPs. Longitudinal studies confirmed that the patients presenting with FPs as the only abnormality progressed to MUP instability before large MUPs associated with fibs-sw were detected. FPs from ALS patients with no other neurophysiological change were simpler than in patients in whom there were also fibs-sw and neurogenic MUPs. The complexity of FPs in patients with weak TA muscle was greater than in the latter group. FPs in patients with benign fasciculations were simpler than FPs in ALS patients with normal TA muscle strength.
Conclusions FPs are a very early marker of ALS and anticipate MUP instability or reinnervation, consistent with a very early phase of increased axonal excitability. Later, widespread neuronal dysfunction causes widespread fibs-sw and loss of MUPs with compensatory reinnervation. Our results confirm the importance of FP morphology analysis in the differential diagnosis of ALS and other disorders, and indicate that benign FPs represent a different phenomenon.
- EMG
- MOTOR NEURON DISEASE
- NEUROMUSCULAR
- NEUROPHYSIOLOGY
- NEUROPHYSIOLOGY, MOTOR
Statistics from Altmetric.com
Introduction
Mills suggested that benign and neurogenic fasciculation potentials (FPs) share identical characteristics, thus implying that fasciculations in amyotrophic lateral sclerosis (ALS) are indistinguishable from FPs in benign fasciculation syndrome.1 This is an important issue since a complex morphology of the FP waveform forms one of the criteria for recognition of neurogenic change in muscles in ALS, for example, as set out in the Awaji consensus.2 Benign FPs have usually been defined as stable, spontaneous potentials of simple, relatively constant morphology with normal jitter between individual components.3 Kimura4 in his textbook stated that ‘no single method [ie, of EMG [electromyography] analysis] reliably distinguishes one type from another [ie, benign vs neurogenic FPs]’. Daube and Rubin5 pointed out that fasciculations occur in many different neurogenic disorders, as well as in normal subjects. Trojaborg and Buchthal drew a distinction between ‘benign’ and ‘malignant’ fasciculations on the basis that FPs in ALS fired more slowly than benign FPs, and tended to be more complex and of longer duration.6 This morphological difference, together with instability of the FP waveform, was also noted by de Carvalho and Swash.7 But it appears that some uncertainty persists.1
We have addressed this issue in a prospective, longitudinal study of the characteristics of FPs and motor unit potentials (MUPs), comparing the findings in ALS with those in a separate group of patients with benign fasciculations. Given the importance of recognising subtle changes in the innervation of muscle in ALS we have sought to define the earliest EMG changes in the disease. We anticipated that relevant information on disease pathogenesis could be derived from observing the earliest EMG changes and their progression. In order to accomplish these aims we studied the tibialis anterior (TA) muscle in a group of patients with ALS from the time of diagnosis by clinical and EMG evaluation. Full diagnostic EMG assessment in other muscles in the four bodily regions was carried out in order to establish the diagnosis of ALS according to accepted criteria. We were therefore able to study disease progression in this muscle, including standard EMG parameters and FPs, from normality to fully developed abnormality, so that we could follow changes over time as the disease progressed to involve the L5 pool of anterior horn cells. We report these observations here.
Patients and control subjects
We studied three groups of subjects; 73 patients with ALS, 10 with benign fasciculations and 37 healthy control subjects. The 73 patients with ALS were recruited consecutively from the EMG diagnostic clinic. The diagnosis of ALS was initially categorised as definite in 10 patients, probable in 47 and possible in 16, according to the El Escorial and Awaji criteria.2 Disease progression was observed in all during follow-up and all patients were then formally recategorised as either probable or definite ALS. In all these patients other neuromuscular disorders (such as polyneuropathy) and diabetes mellitus were ruled out. Patients with marked lower limbs spasticity (>2 on the modified Ashworth scale)8 were excluded since marked spasticity would have precluded full clinical evaluation of lower motor neuron function. In each subject the TA muscle was studied according to a standard protocol (see below).
ALS patients with TA muscle of normal strength
We studied the early changes in ALS in 61 of the 73 patients, aged 42–80 years (mean 64.0), in whom the TA muscle was of normal strength; 37 were men. These 61 patients were studied at their initial diagnostic EMG evaluation. In each subject the selected TA muscle was of normal strength, defined as medical research council (MRC) grade 5/5 force, plus the ability to walk on the heel on that side; in addition, the TA muscle was not atrophied. If both TA muscles were of normal strength, the right side was chosen. Twenty-three of these patients had bulbar-onset ALS, 21 had upper-limb onset, and 13 had lower-limb onset disease on the opposite side as the TA muscle selected for study. An axial-onset disease occurred in four patients. The mean disease duration was 9.3 months (range 2–16 months; SD 4.6); all these ALS patients had a disease duration <18 months. A subgroup of 26 patients (43%) who retained normal strength in the TA muscle were reinvestigated at intervals of 3–6 months.
ALS patients with slightly weak TA muscles (MRC 4)
We also studied a group of 12 patients, eight men, aged 53–78 years (mean 65.1 years), with slightly weak TA muscles (MRC 4), in whom clinically evident fasciculations were observed in the studied muscle. In these patients the disease was bulbar-onset in four, upper-limb onset in five and lower limb-onset in three. The mean disease duration in this subgroup was 11.8 months (6–25 months).
Patients with benign fasciculations
This group consisted of 10 men with benign fasciculations aged 39–64 years (mean 52.2 years). Benign fasciculation syndrome was defined as a disorder presenting with symptomatic cramps and fasciculations without weakness or atrophy, in which nerve conduction studies were normal and there was no systemic disorder. In these men multi-MUP analysis in the TA muscle, as in other muscles studied in these patients, was normal. Clinical follow-up and repeated neurophysiological investigation for more than 2 years (from 2.5 years to 8 years) excluded progression to ALS or to other disorders.
Healthy control subjects
The 37 healthy control subjects (19 men) were aged 30–80 years (mean 64 years). They were recruited as volunteers among hospital staff (16 people) and from relatives of people with ALS who had asked for EMG examination to relieve their personal anxiety (21 people). None of these control subjects developed ALS or any other neuromuscular condition in the subsequent 2 years. The multi-MUP and jitter analysis results were statistically similar between both subgroups (p>0.1).
Ethics
All subjects studied gave their informed consent. The protocol was approved by the local research ethics committee.
EMG methods
We used a KeypointNet EMG machine. The skin temperature was monitored and was always greater than 32°C. We evaluated a number of variables:
MUP analysis
A minimum of 20 different MUPs were recorded from five or more different sites in the TA muscle, during a slight voluntary contraction. The multi-MUP analysis program was implemented on the EMG machine to analyse MUP data. Standard filter setting (5–10 KHz), gain (200 μV/div) and sweep speed (10 ms/div) were used. The mean amplitude, mean duration, mean area, mean number of phases and mean number of turns were analysed. The percentage of polyphasic potentials was noted. These data were calculated automatically according to previously published standards.9 ,10
Motor unit stability studies
We calculated the mean jitter and evaluated blocking in at least 10 different pairs of potentials in TA muscle using a concentric needle EMG electrode (recording area 0.07 mm2), a 1000 Hz low band pass filter and a trigger delay line, with a sweep speed of 1 ms/div.11 ,12 In the initial assessment of ALS patients, when the initial 10 potential pairs showed normal stability, an additional 10 pairs were studied in order to confirm stability. Increased jitter was defined by the presence of one of the three following abnormalities: abnormal mean jitter, >20% abnormal pairs and >10% blocking (table 1).
Control values in the healthy subjects for tibialis anterior (TA) muscle recordings
Spontaneous EMG activity
In TA muscle spontaneous activity was studied in 10 different sites, using five or more needle insertions, with the conventional concentric needle EMG.
Fibrillations/positive sharp waves (fibs-sw) were considered as present if observed as reproducible trains of fibs-sw lasting at least 1 s following needle insertion in at least two different sites in a muscle. Filter settings were 5–10 KHz, gain 100 μV/div and sweep speed 20 ms/div.
FPs were considered as present if observed in a TA muscle completely at rest in at least one site in the muscle. We followed the definition of FPs as set out in the recommendations of the American Academy of Electrodiagnostic Medicine13 and by Daube and Rubin5; spontaneously and randomly discharging action potentials of a group of muscle fibres innervated by the same anterior horn cell. FPs thus resemble the morphology of MUPs.7 We accepted FPs only if their amplitude was greater than 50 μV, since that is the smallest amplitude accepted by Rosenfalck in the Buchthal laboratory analysis as defining a MUP.14 Combined FPs, as defined by complex potentials consisting of two or more components that could occur independently, were not included in this study.15 Patients were always placed at rest in a comfortable prone posture. A minimum of 1 min recording time was required at each of the recording sites before rejecting a site as not revealing FPs.16 The mean amplitude, the mean duration and the mean number of phases of the FPs were assessed, by using the manual MUP analysis software. Any doublet FPs were noted. The variability in the morphology of the observed FPs was assessed qualitatively. The morphology of FPs was compared with that of voluntarily activated MUPs in the same muscle if at least five different FPs were recorded in the test muscle. In patients investigated two or more times FP morphology was compared between the initial and final evaluation when at least five different FPs were recorded in the test muscle.
Results
Controls
No fibs-sw or FPs were recorded in any of the control subjects. The multi-MUP analysis and the jitter results in TA muscles, for voluntarily recruited MUPs, in the group of 10 subjects with benign fasciculations were within the normal range (table 1).3 ,12
FP morphology
Fasciculation potentials from patients with benign fasciculation syndrome
In the 10 subjects with benign fasciculation syndrome 61 FPs were studied in the TA muscle recordings (table 2). These benign FPs were of smaller amplitude (p=0.003) and of fewer phases (p=0.007) compared with FPs in TA muscles of normal strength in ALS patients. Although these benign FPs were of 11% shorter duration than FPs in ALS this difference was not statistically significant (p=0.08; table 2). In subjects with benign fasciculations, only 5% of the FPs were polyphasic and no doublet FPs were seen (figure 1A).
Parameters of fasciculation potentials (FPs) in the three groups of subjects studied, expressed as mean values and SD's

Electromyography: Fasciculation potentials (FPs). (A) Benign FPs, the potentials are of simple morphology, normal size and stable (one FP discharging twice is marked  ). (B) FPs from a patient with amyotrophic lateral sclerosis recorded in tibialis anterior (TA) muscles of normal strength. Most FPs are of normal morphology. Two FPs are discharging repeatedly but their morphology is stable (
). (B) FPs from a patient with amyotrophic lateral sclerosis recorded in tibialis anterior (TA) muscles of normal strength. Most FPs are of normal morphology. Two FPs are discharging repeatedly but their morphology is stable ( and
and  ). (C) FPs from a weak TA muscle (medical research council 4). The FPs are generally complex, one (inside a box) has a very long duration. The FPs discharging more than once are marked (
). (C) FPs from a weak TA muscle (medical research council 4). The FPs are generally complex, one (inside a box) has a very long duration. The FPs discharging more than once are marked ( ,
,  ,
,  and
and  , they are unstable (the unstable components are marked with an arrow).
, they are unstable (the unstable components are marked with an arrow).
Fasciculation potentials from patients with normal strength TA muscles (MRC 5)
In the 61 ALS patients with normal TA muscle strength at study entry, FPs were recorded by EMG in 42 TA muscles (68.9%) at study entry—in total 223 different FPs were analysed (figure 1B and table 2). Doublet FPs were very rarely observed (2.7% of the 223 FPs). The mean amplitude, mean duration, number of phases and percentage of polyphasic potentials were significantly lower in the group of patients with normal TA muscle strength as compared with the 76 FPs recorded from the 12 patients with slightly weak (MRC 4) TA muscles (figure 1C and table 2). Moreover, doublet FPs were more frequently observed in the latter group (11.8% of FPs; p<0.01).
In 21 TA muscles of MRC 5 strength in which the MUP analysis was normal, in which there were no fibs-sw and the jitter was normal or only slightly increased, 77 FPs were recorded (table 3). No doublet fasciculations were observed. In 40 muscles in which the EMG showed abnormal MUP analysis and/or fibs/sw 146 FPs were recorded; the jitter was increased in all but two of these muscles. The FPs recorded in these muscles were of significantly higher amplitude (p=0.005) and increased number of phases (p=0.02) when compared with those deriving from TA muscle with normal MUP analysis. Their duration tended to be longer (8%) but this did not reach statistical significance (p=0.16) (table 3). Six of these 146 FPs showed doublet discharges.
Fasciculation potential (FP) parameters in TA muscles of MRC 5 strength in patients with ALS
Progression of EMG features
In 12 patients with normal TA strength (MRC 5) MUP morphology was normal and no FPs were recorded; but in five of these we found borderline increased jitter (mean 77.6 μs, range 59–104 μs) as the only EMG abnormality. Three of these patients were reinvestigated after 3 months; FPs were recorded in two of these subjects at this second assessment, but mean MUP and jitter duration remained unchanged. In the third patient, in whom the first study showed slightly increased jitter, with no spontaneous activity, the same pattern of abnormality was found at the second study.
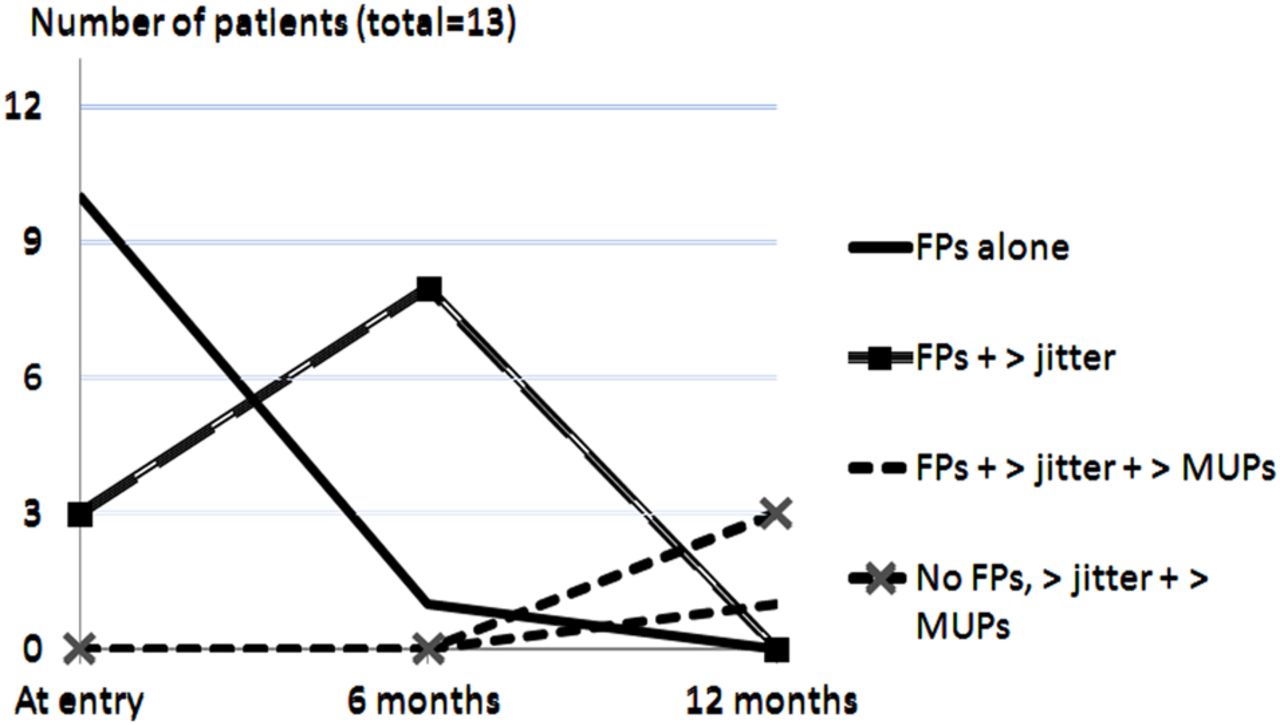
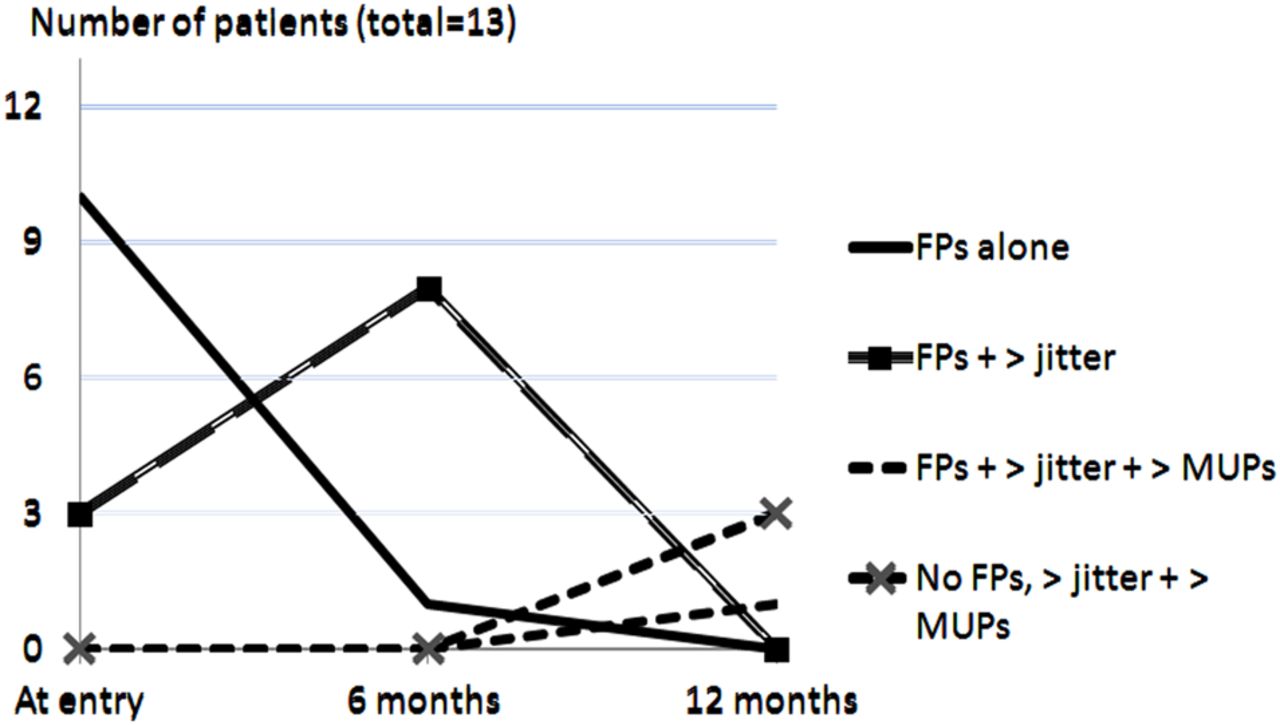
We recorded FPs in 21 patients whose TA muscles were of normal (MRC 5) strength with MUPs of normal morphology. In six of these there was a mildly increased jitter but no other EMG abnormality; there were more than 20% potential pairs with increased jitter or more than 10% blocking (mean jitter 63.8 μs, range 54–90μs; table 1). In the remaining patients, with normal jitter at the first assessment, extension of the investigation to record a further 10 potential pairs in TA muscle did not change the classification of these stable motor units (MUs). In this subset of 21 patients, FP mean amplitude (625.2 μV), mean duration (11.57 ms) and mean number of phases (3.37) was similar to MUP amplitude (650.2 μV, p=0.76), MUP mean number of phases (3.49, p=0.58) and MUP mean duration (9.69 ms, p=0.1). Thirteen of these 21 patients were reinvestigated 3–6 months later (figure 2). MUPs recorded in this later investigation were larger and more unstable, and fibs-sw more frequent, but FPs were scarcer in this later phase of muscle involvement. At the 6 months follow-up examination, the mean jitter had increased (p<0.001) from 49.2 μs (SD 17.7) to 83.8 μs (SD 20.3) and the MUP mean duration (p<0.001) increased from 9.3 ms (SD 1.3) to 11.5 ms (SD 1.4).
{kind=link}
{kind=link}
Progression of 13 amyotrophic lateral sclerosis patients with isolated fasciculation potentials (FPs) (normal motor unit potential (MUP) and no fibrillation/sharp-waves (fibs-sw)). All patients were evaluate 6 months later, but only four had preserved normal tibialis anterior strength 12 months after study entry. The Y-axis represents the number of patients.
There were 21 patients with normal TA muscle strength and neurogenic MUPs (mean duration 12.4 ms, range 9.4–15.3 ms); in 10 of these no fibs-sw were recorded and in 7 FPs were absent. All MUPs were unstable (mean 64 μs, range 55.4–82.0 μs). Four of the 10 patients with FPs but no fibs-sw were reinvestigated 3–6 months later; FPs persisted and fibs-sw were observed in this second investigation; mean jitter increased from a mean of 59 μs to 100 μs and mean duration increased from 12.1 ms to 15.2 ms. Two patients with fibs-sw and FPs were reinvestigated 6 months later; in both fibs-sw persisted but FPs were no longer observed. This was confirmed in one patient at a second follow-up examination 3 months later. MUP duration and instability increased in the 6-month period (mean duration increased from 12.7 ms to 14.4 ms, and mean jitter from 79 μs to 97 μs). In seven patients we found fibs-sw but no FPs, associated with very large neurogenic MUPs (mean duration 13.9 ms, range 11–16.6 ms) and very unstable MUs (mean jitter 110.9 μs, range 87–136 μs). Four patients from this group were reinvestigated after 3 months; in all the same changes were observed, but none showed FPs.
Changes in FP morphology during follow-up
We compared the morphology of FPs in seven patients with normal TA muscle strength, in whom five or more different FPs were recorded at an interval of 3–6 months (mean 4.5 months); in these subjects we recorded 42 FPs at the first observation and 44 at the second. Mean amplitude increased from 651.9 μV (SD 493.7) to 1113.1 μV (SD 723.7) (p=0.02), mean duration increased from 12.46 ms (SD 3.9) to 15.46 ms (SD 6.) (p=0.004), but the mean number of phases did not change significantly (mean value of 3.60 and 3.73, respectively).
Variability of FP morphology and firing frequency
Variability of FP morphology was assessed every time the same FP was recorded three or more times. This was easier to study in slightly weak (MRC 4) than in strong TA muscles, because in strong muscles we found many different MUs fasciculating in the same needle recording area. In general, very complex FPs showed more variability than simpler FPs. No quantitative assessment was made (figure 1B,C).
Individual FP firing rates were not analysed. Although there was a trend towards increased FP firing frequency in muscles of normal strength, the differences were not statistically significant (0.148 Hz for benign FPs, 0.142 Hz for MRC 4 and 0.169 Hz for MRC 5). Although FP frequency was not influenced by upper motor neuron signs in our patients, it should be noted that we excluded patients with marked lower limb spasticity.
Discussion
We evaluated neurophysiological changes in the TA muscle at the first diagnostic investigation in patients with ALS. In 21 of the 61 TA muscles of normal strength (MRC5) the presence of FPs was the only EMG abnormality, although a borderline increased neuromuscular jitter was also noted in six of these 21 TA muscles. In 19 patients no FPs were found in the TA muscle recordings. In 12 the TA muscle was normal at EMG and in the remaining 7 there were fibs-sw and abnormal MUPs without FPs. Increased jitter has been recognised previously as an early feature of ALS,17 ,18 but the occurrence of FPs in otherwise normal muscles in ALS, including normal MUP parameters and normal neuromuscular jitter, was an unexpected finding. This is an important observation, however, since it confirms the relevance of FPs as an early feature of ALS. In the Awaji consensus modification of the El Escorial criteria FPs are defined as one of the features suggesting the onset of neurogenic change in the context of a suspected diagnosis of ALS.2 Our clinical and electrophysiological studies show that isolated FPs anticipate other EMG changes by 3–9 months and muscle weakness by 6–18 months; variability is related to the rate of disease progression in different subjects.
Kleine et al investigated the firing pattern of FPs from ALS patients, using high-density surface EMG. They distinguished two distinct types of FPs.19 Most seemed to originate from membrane instability in motor axons,19 but some may have derived from low-threshold motor neurons, recruited by the hyperexcitable corticospinal system.15 ,19 ,20 Indeed, transcranial magnetic stimulation can drive FPs of simple morphology in ALS.21 Although we did not specifically investigate the origin of FPs, we consider that in ALS simple and stable FPs originating from muscles without other EMG changes probably arise from hyperexcitable lower motor neurons. This interpretation takes into account that the FP morphology at this stage of neurogenic change in ALS resembles that of normal MUPs recorded in the same muscle, and that no doublet discharges were observed.
In muscles with neurogenic MUPs, FPs tend to be of higher amplitude, longer duration, poplyphasic and unstable, particularly in weak muscles. Doublets have been associated with increased supernormality of the axonal membrane.22 Doublets were not observed in patients with benign FPs, or in ALS patients without neurogenic changes in the studied muscle, but they were easily observed in weak muscles. This set of data suggests that FPs from neurogenic muscles in ALS probably derive from distal, slower conducting axonal branches.7 ,23
We have shown that FPs are frequently the first abnormality recorded by EMG during the course of neurogenic change in ALS. Unstable MUPs develop as the next feature of MU involvement in the disease suggesting distal axonal involvement. Distal axonal dysfunction, beginning at the neuromuscular junction, has been recognised in superoxide-dismutase-1 (SOD-1) rodent models of ALS,24 before axonal degeneration or anterior horn cell loss, implying a dying back distal axonopathy.25–27 In mouse models, FPs have not been observed, but prolonged duration of the action potential causing axon instability and repetitive activity has been considered as reminiscent of fasciculations.28 When a significant number of MUs become dysfunctional in ALS, fibs-sw, large and very unstable MUs are seen and more complex and unstable FPs appear in the recording.3 ,18
Our sequential studies of the morphology of FPs over a period 3–6 months in ALS patients, revealed increasing amplitude and duration, although the change in the number of phases did not reach statistical significance. It is likely, therefore, that the site of origin of these FPs remained stable during this period. We have not noted reappearance of FPs once they have ceased to be recorded in a more affected, atrophic muscle. Fibs-sw, however, persist in these muscles as denervation change becomes progressively more evident. Benign fasciculations, and FPs in TA muscles in ALS patients that showed no features of reinnervation, that is, the earliest stage of the disease in that muscle, were similar in size, duration and morphology. However, in benign fasciculation syndrome we never observed complex or unstable FPs, or doublet FPs. Mills studied 11 patients with a final diagnosis of benign fasciculations.1 His patients presented with unexplained neurological symptoms and signs and no follow-up information was given. In contrast, our patients diagnosed with benign fasciculations were followed up for more than 2 years, and none developed any neurological disease. This is important because, very uncommonly, ALS has been reported to develop in patients, at first diagnosed as benign fasciculation syndrome.29 ,30 Mills evaluated up to four different muscles in his study, but did not attempt to consider the changes he reported in relation to separate normative data for these muscles.1 We note that Mills accepted potentials as small as 30 μV, that would usually be discarded as likely to represent discharge of a single muscle fibre.14–31 Indeed, the software used for quantitative MUP analysis in the KeyPoint machine automatically discards potentials smaller than 50 μV in accordance with the work of Stålberg et al9 Most descriptions of the EMG features of ALS relate to diagnostic features characteristic of well-established disease in tested muscles.18 Our results emphasise the importance of FPs as a first manifestation of ALS.
Acknowledgments
This work was supported by ‘Fundação para a Ciência e Tecnologia’—JPND/0002/2011.
References
Footnotes
-
Contributors MdC and MS provided: (1) substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; (2) contribution towards drafting the article or revising it critically for important intellectual content; and (3) final approval of the version to be published.
-
Funding Fundação para a Ciência e Tecnologia-JPND/0002/2011.
-
Competing interests None.
-
Ethics approval Local hospital ethics committee in Lisbon.
-
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- Editorial commentary