Article Text

Abstract
Background Grey matter (GM) pathology in multiple sclerosis (MS) is associated with progressive long-term disability. Detection of GM abnormalities in early MS may therefore be valuable in understanding and predicting the long-term course. However, structural MRI measures such as volume loss have shown only modest abnormalities in early relapsing-remitting MS (RRMS). We therefore investigated for evidence of abnormality in GM perfusion, consistent with metabolic dysfunction, in early RRMS.
Methods 25 RRMS patients with ≤5 years disease duration and 25 age-matched healthy controls underwent 3 Tesla MRI with a pseudo-continuous arterial spin labelling sequence to quantify GM perfusion and a volumetric T1-weighted sequence to measure GM volume. Neurological status was assessed in patients and neuropsychological evaluation undertaken in all subjects. Voxel-based analysis was used to compare regional GM perfusion and volume measures in patients and controls.
Results There was reduced global GM perfusion in patients versus controls (50.6±5.8 mL/100 g/min vs 54.4±7.6 mL/100 g/min, p=0.04). Voxel-based analysis revealed extensive regions of decreased cortical and deep GM perfusion in MS subjects. Reduced perfusion was associated with impaired memory scores. There was no reduction in global or regional analysis of GM volume in patients versus controls.
Conclusions The decrease in GM perfusion in the absence of volume loss is consistent with neuronal metabolic dysfunction in early RRMS. Future studies in larger cohorts and longitudinal follow-up are needed to investigate the functional and prognostic significance of the early GM perfusion deficits observed.
- CEREBRAL BLOOD FLOW
- MULTIPLE SCLEROSIS
- COGNITION
- CLINICAL NEUROLOGY
Statistics from Altmetric.com
Introduction
Multiple sclerosis (MS) is a chronic demyelinating disorder of the central nervous system in which white matter (WM) lesions are readily visualised on T2-weighted MRI in almost all patients in the early clinical phase of the disease.1 However, modest correlation of T2 lesion load with both concurrent and future clinical impairment has stimulated efforts to identify other quantitative imaging measures to more fully elucidate pathological events in the early disease course and to identify imaging measures that more robustly predict the future course of MS. This includes measures of the volume and intrinsic structural integrity of both grey matter (GM) and WM.
Recent histopathological and structural MRI studies in MS have found evidence of GM abnormalities that are especially marked in progressive MS. GM tissue volume loss measured on MRI is often substantial in progressive MS2 ,3 and its presence implies neuronal loss. Cortical demyelinating lesions are often abundant in progressive MS.4 ,5 The presence and extent of cortical lesions seen on MRI has been correlated with physical disability and cognitive impairment in MS6 and may contribute to GM atrophy.4 Furthermore, GM atrophy has been identified in several studies to be strongly associated with permanent or progressive physical disability2 and with cognitive impairments in MS.7
In respect of the relationship of irreversible GM damage with progressive MS and long-term disability, it would be advantageous to have imaging measures that detect early and potentially reversible pathophysiological GM abnormalities in vivo, before irreversible damage has occurred. Such imaging measures could help elucidate the mechanisms leading to, and predict the future risk of, neuronal tissue loss; these markers might also be used to monitor the efficacy of experimental neuroprotective treatments at an early stage of disease, when there is the greatest potential to prevent irreversible GM damage.
Several previous studies have used perfusion MRI techniques to measure cerebral blood flow (perfusion) in relapsing-remitting MS (RRMS) patients. These studies have identified both decreases8–11 and increases12 of perfusion in WM. A decrease in WM perfusion might be secondary to a reduction in tissue metabolic function, or it could reflect a primary vascular mechanism causing reduction in blood flow. Inflammation with increased tissue metabolic demand has been proposed as a mechanism of increased WM perfusion. Other studies have shown decreased perfusion in deep GM11 ,13 ,14 and decreased perfusion in cortical lesions when compared with normal appearing cortical GM.15 It is likely that a decrease in GM perfusion reflects either neuronal metabolic dysfunction or neuronal loss. The question arises as to whether perfusion MRI in early RRMS might detect a reduction in GM perfusion in the absence of GM atrophy, which could potentially indicate a reversible state of neuronal dysfunction prior to irreversible neuronal loss.
Arterial spin labelling (ASL), a safe and non-invasive perfusion imaging modality, uses the inflowing cerebral blood as an endogenous tracer to quantitatively measure cerebral blood flow (mL/100 g/min).16 Pseudo-continuous ASL (p-CASL) combines the advantages of both pulsed and CASL (higher signal-to-noise ratio, higher tagging efficiency and improved transit time).17 In addition, p-CASL, used with background suppression, has proved to be a robust clinical method to measure in vivo perfusion changes with the least data dispersion and best reproducibility measures in both single-centre and multicentre data.18 This technique has been used to detect perfusion abnormalities in patients with neurodegenerative disorders19 but has not to our knowledge been previously investigated in patients with MS.
In this study, we investigated the integrity of GM tissue volume and perfusion in a group of early RRMS patients (≤5 years from symptom onset) and age-matched healthy controls. In addition to p-CASL, the study acquired structural MR images and comprehensive cognitive and neurological assessments. We hypothesised that reduced GM perfusion would be detected early in the disease, in the absence of detectable GM atrophy, and that the GM perfusion abnormalities would correlate with measures of clinical and/or cognitive dysfunction.
Methods
Study design
Twenty-five patients with early (≤5 years from symptom onset) RRMS (McDonald criteria1) were recruited by an experienced MS neurologist. All patients were aged between 18 and 56 years and had been relapse-free and clinically stable for at least 3 months before study entry. Exclusion criteria included a history of other central nervous system disorders (eg, head injury, cerebrovascular disease, brain surgery or tumour), severe depression, as measured by Beck Depression Inventory (BDI-II), English as a second language, dyslexia and steroid treatment within the preceding 3 months. Five RRMS patients were receiving interferon β treatment. Twenty-five age-matched healthy controls, with no previous history of neurological disorders, were also investigated. Assessments which included neurological, neuropsychological and MRI were scheduled over 1 month. This study was approved by the Lower South regional ethics committee of New Zealand and informed consent was obtained from all participants.
Neurological and neuropsychological assessments
All patients underwent clinical assessments, including relapse history, disability assessment using the Expanded Disability Status score (EDSS), MS Functional Composite (MSFC) and MS severity score (MSSS) (derived from the EDSS and disease duration). Subjects’ premorbid IQ was estimated with the Wechsler Test of Adult Reading (WTAR). All participants performed the Montreal Cognitive Assessment (MoCA) and 11 standard neuropsychological tests covering four cognitive domains: executive function (letter fluency, category fluency, Stroop interference), memory (both visual (Brief Visual Memory Test) and verbal (Californian Verbal Learning Test) tests), attention and working memory (Stroop colours, word reading, Symbol Digit Modality Test (SDMT), Paced Auditory Serial Addition Test (PASAT)) and visuospatial function (Judgment of Line Orientation, Rey Complex Figure copy). Raw test scores were converted to z-scores on the basis of age-adjusted and gender-adjusted normative data for each test and then averaged for each domain. Group differences were assessed using analysis of covariance (ANCOVA) model (R software V.2.15.2, R core team, 2012) controlling for sex, age and premorbid IQ.
MRI data acquisition
All scans were acquired in a single session on a 3 T General Electric HDx scanner with an eight-channel head coil.
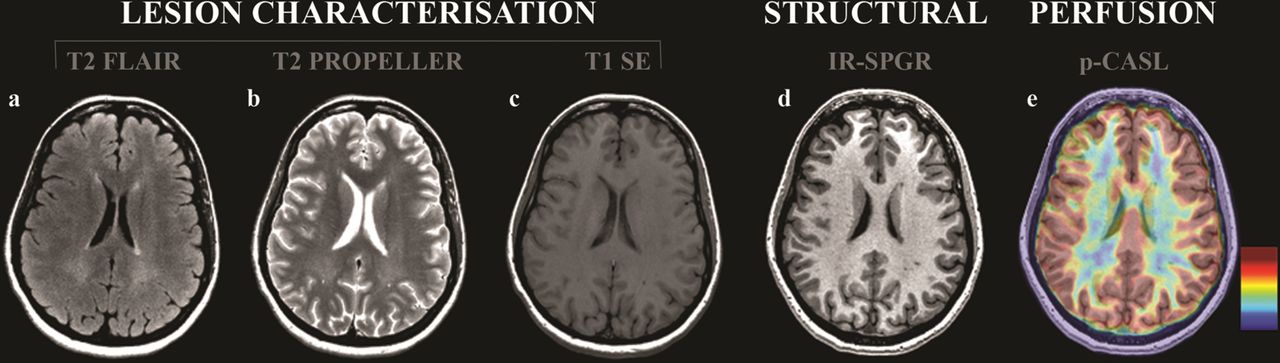
Conventional MRI sequences were acquired for lesion characterisation: T2 FLAIR (SE, TE/TR=11/500 ms, TI=2250 ms, acquisition matrix=512×512×50, field of view (FOV)=220 mm, voxel size=0.43×0.43×3.0 mm3), T2 PROPELLER (SE, TE/TR=98/3700 ms, acquisition matrix=512×512×50, FOV=220 mm) and T1 SPIN ECHO (SE, TE/TR=12/500 ms, acquisition matrix=512×512×50, FOV=220 mm, voxel size=0.43×0.43×3.0 mm3).
Additional imaging included a volumetric, T1-weighted inversion-prepared spoiled gradient recalled-echo acquisition (IR-SPGR, TE/TR=2.8/6.6 ms, TI=400 ms, flip angle=15°, acquisition matrix=256×256×170, field of view (FOV)=250 mm, voxel size=0.98×0.98×1.0 mm3) to measure tissue volumes and a p-CASL sequence19 ,20 (a stack-of-spiral fast spin echo acquired images, eight interleaved spiral arms with 512 samples at 62.5 kHz bandwidth and 30 phase-encoded 5 mm slices, postlabelling delay=1525 ms, labelling duration=1525 ms, FOV=240 mm, voxel size=3.75×3.75×5 mm3, Number of excitations=5) (figure 1) used to quantitatively measure perfusion in mL/100 g/min. Subjects were asked to remain still throughout the scan, and for the perfusion imaging sequence, subjects’ eyes were closed.

MRI images obtained for all participants in the study. MR images for lesion characterisation included (A) T2 FLAIR, (B) T2 PROPELLER and (C) T1 SPIN ECHO sequences. (D) displays the T1-weighted inversion-prepared spoiled gradient recalled-echo (IR-SPGR) image used for structural analysis, and (E) shows a perfusion image using pseudo-continuous arterial spin labelling (p-CASL).
MR data analysis
Lesion segmentation
Lesion load: MS lesions were manually outlined on T2 FLAIR images by a single trained observer using Jim software (Jim V.4.0 Xinapse System Leicester, UK) to quantify T2 lesion load for each patient. The presence of T2 lesions was confirmed by reference to T2 PROPELLER (hyperintense lesions) and of T1 hypointense lesions by reference to the T1 SE images.
Lesion filling: Additionally, lesions were manually outlined on the IR-SPGR images. The presence of IR-SPGR-identified lesions was confirmed by reference to the T2 FLAIR images. Lesions were then automatically filled with a lesion-filling program (LEAP) so that they had the same signal intensity as surrounding normal appearing tissue.21 This was done to avoid classification biases during the subsequent GM and WM tissue segmentation procedures. Each structural image was visually inspected after lesion filling to confirm that they had been effectively filled.
Voxel-based morphometry (VBM) analysis
Data preprocessing and analysis were performed using VBM8 (http://dbm.neuro.uni-jena.de/vbm/), a toolbox of SPM8 (Statistical Parametric Mapping, Wellcome Department of Imaging Neuroscience Group, London, UK; http://www.fil.ion.ucl.ac.uk/spm) in Matlab V.7.10.0 (R2010a, Mathworks, Massachusetts, USA). After lesion filling, structural images were intensity bias corrected, tissue classified and registered using linear and non-linear transformations (DARTEL) within a unified model.22 GM segments for each subject were modulated using non-linear components of the normalisation only, thereby preserving actual tissue values locally in order to account for individual brain size globally.23 Modulated, normalised GM segments were smoothed with a 10 mm full width at half maximum (FWHM) Gaussian kernel to improve signal to noise, to meet the assumptions underlying Gaussian random fields theory and to account for any spatial normalisation imperfections.24 A smoothing kernel of 10 mm has been reported to be appropriate for DARTEL-VBM analysis to detect GM atrophy for group sizes of 25.25 A visual inspection of the data was performed to detect and correct any tissue misclassification.
Perfusion images were coregistered to the IR-SPGR images using SPM8 and normalised using the deformation fields generated from the structural registration and warping process. Normalised perfusion images were also smoothed with a 10 mm FWHM Gaussian kernel. Intracranial volume was –defined as the sum of GM, WM and cerebrospinal fluid segments—global GM and WM volumes and global GM and WM perfusion measurements were extracted for each subject. Although our study was focused on GM, global WM volume and perfusion measurements were included in order to provide information on WM abnormalities at this stage.
Statistical analysis
Voxel-based analysis
Voxel-based analyses were performed to investigate regional differences between MS and control subjects on the smoothed, modulated, normalised GM volume and smoothed, normalised GM perfusion images. Group differences (control vs early RRMS) in GM volume and GM perfusion were assessed using ANCOVA models, with age, gender and premorbid IQ as covariates.
Individual multiple linear regressions were used to assess the relationship of perfusion measurements with clinical (disease duration, EDSS, MSSS, MSFC) and cognitive impairments (MoCA, PASAT, SDMT, executive function z-score, visual and verbal memory z-score, attention and working memory z-score and visuospatial function z-score), T2 and T1 lesion loads, with age, gender and premorbid IQ as covariates in all subjects. An average GM mask was created from normalised GM segments of the 25 healthy controls, thresholded at a value of 0.20 (voxels with >20% GM fraction values) and used to restrict statistical comparisons with the GM. The results were corrected for multiple comparisons using the false discovery rate (FDR) (p<0.05).
Statistical analysis on global WM and GM metrics
All statistical tests were performed using R software (V.2.15.2, R core team, 2012). Global GM and WM volume and perfusion measurements were assessed between early RRMS and healthy controls using an ANCOVA model, adjusting for age, gender and premorbid IQ. Multiple linear regressions were used to assess the association of (1) WM volume and WM perfusion, (2) GM perfusion and WM volume and (3) GM perfusion and WM perfusion. Age, gender and premorbid IQ were added in the model as covariates as they can affect volume and perfusion measurements.
Results
Clinical and cognitive scores
Demographic, neurological and neuropsychological data are presented in table 1. Sixty-eight per cent of the patients had a disease duration of less than 2 years and 24 out of 25 patients had an EDSS of 2.5 or less, reflecting minimal neurological impairment. When corrected for sex, age and premorbid IQ, the early RRMS group revealed a significantly lower z-score (p=0.05) only in memory (mean: 0.7; SD: 0.6) relative to healthy controls (mean: 1.2; SD: 0.5). No differences were seen in SDMT (p=0.5), PASAT (p=0.8), MSFC (p=0.4), MoCA (p=0.8), executive function (p=0.3), attention and working memory (p=1.0) and visuospatial function (p=0.71) (table 1).
Table description of demographical, neurological, neuropsychological and global imaging details of each group (healthy controls vs early RRMS)
Voxel-based analysis
Visual inspection of GM segments for each subject showed that there was no obvious tissue misclassification.
Between-group comparison
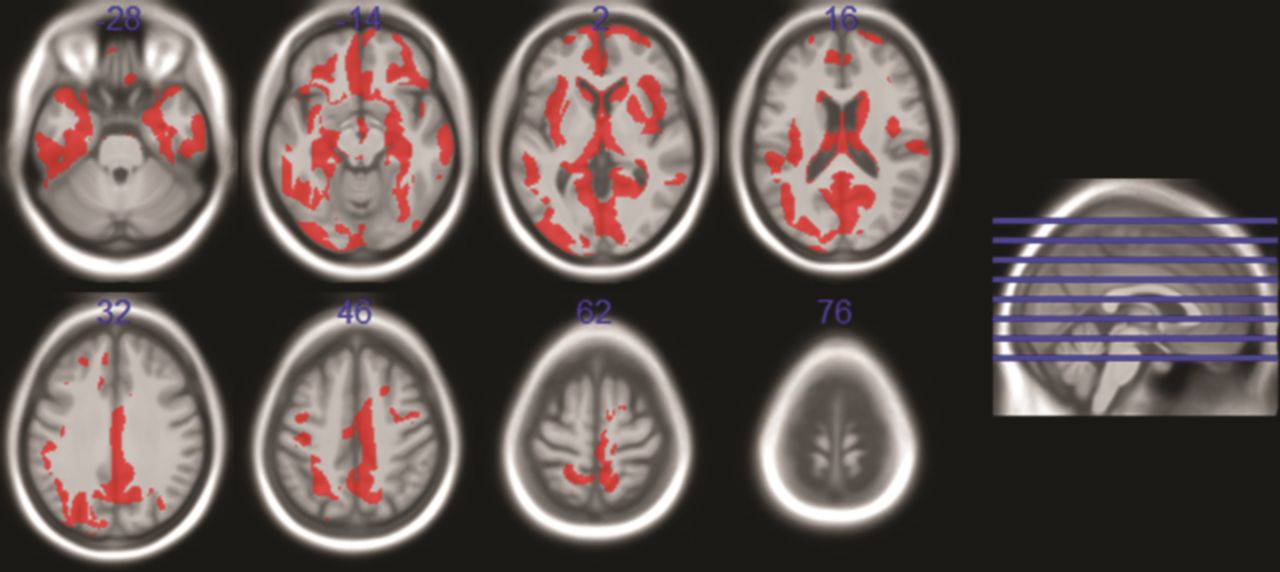
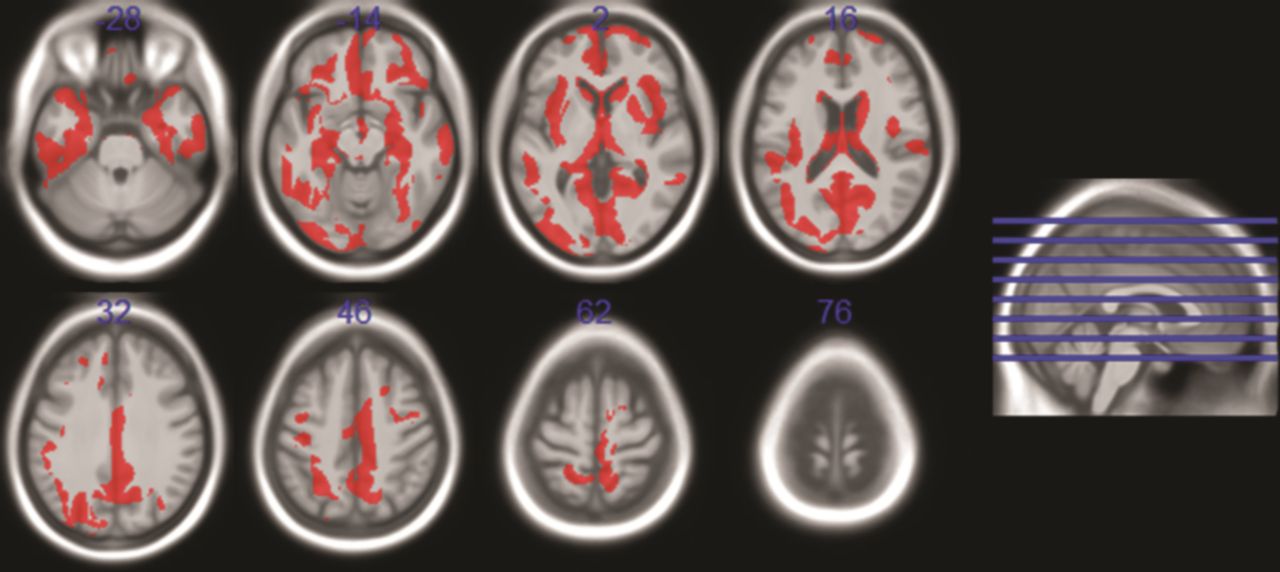
Reduced GM perfusion in the early RRMS group versus controls was seen in the lingual gyrus, intracalcarine, insular and operculum cortex, temporal (temporal gyrus, temporal fusiform cortex), parietal (precuneus cortex, superior parietal lobule), frontal (frontal gyrus, postcentral gyrus, frontal orbital cortex) and occipital areas and deep GM (bilateral thalamus, left hippocampus, right caudate and right putamen). Areas of significantly reduced GM perfusion (FDR-corrected p<0.05), overlaid on the Montreal Neurological Institute template, are displayed in figure 2 and summarised in table 2.
Areas of significantly (p<0.05 and corrected for multiple comparisons in each voxel) reduced GM perfusion measurements in early RRMS patients relative to controls
{kind=link}
{kind=link}
Regions displaying areas of significantly (false discovery rate, p<0.05, corrected t>2.59) reduced perfusion in patients with early relapsing-remitting multiple sclerosis compared with healthy controls, covarying for age, gender and premorbid IQ. The map of significant clusters is overlaid onto a T1-weighted template in Montreal Neurological Institute Space (MNI 152 template).
No significant decrease in regional GM volume was found in early RRMS relative to controls using voxel-based analysis.
Correlation with neurological and neuropsychological scores
The voxel-based analysis revealed positive associations between GM perfusion values and memory z-scores in the precentral and postcentral, cingulate, lingual and frontal gyri, intracalacarine and supracalcarine cortex, parietal (supramarginal and angular gyri, precuneus cortex) and occipital areas, bilateral accumbens, putamen, caudate and right thalamus. No significant association was found between GM perfusion values and disease duration, EDSS, MSSS, MSFC, SDMT, PASAT, MSFC, MoCA, executive function, attention and working memory, visuospatial function or T2 and T1 lesion loads.
Global GM and WM volume and perfusion measurements
There was a significant decrease in global GM perfusion in the RRMS group versus controls (50.6±5.8 mL/100 g/min vs 54.4±7.6 mL/100 g/min, p=0.04), but no significant difference in global GM volumes (46.1±3.3% vs 45.7±2.0%, p=0.38) (table 1).
Statistical analysis of WM metrics revealed a significant decrease in WM volume in RRMS patients compared with controls (37.3±1.5% vs 38.8±1.5%, p=0.01). Global WM perfusion was also significantly reduced in the RRMS group compared with controls (28.9±3.0 mL/100 g/min vs 31.2±4.9 mL/100 g/min, p=0.01) (table 1).
Relationship between WM volume and WM perfusion, GM perfusion and WM volume and GM perfusion and WM perfusion
Visual inspection of the quantile plots of the residuals confirmed the normality of the residuals. Non-constant variance test was not rejected, validating homoskedasticity, and the predictors were not correlated with each other (variation inflation factor was found to be less than 3.3). In all subjects, there was no association between WM perfusion and WM volume (β=0.13, p=0.56) and GM perfusion and WM volume (β=0.17, p=0.69). Decreased WM perfusion was significantly associated with decreased GM perfusion (β=0.59, p<0.01).
Discussion
This, the first study to assess perfusion abnormalities using p-CASL in MS, focused on GM integrity in early RRMS. The major finding of the study was the presence of a widespread decrease in GM perfusion in the absence of GM atrophy.
GM abnormalities in early RRMS
Reduced GM perfusion in deep GM has previously been demonstrated in RRMS using region-of-interest analysis.11 ,13 ,14 Using voxel-based analysis, we found decreased perfusion in deep GM and also in multiple cortical areas, including lingual gyrus, intracalcarine, insular and operculum cortex, as well as some temporal, parietal, frontal and occipital cortical regions. Only one previous study has used voxel-based analysis to investigate regional GM perfusion changes in MS. The study used a CASL technique at 1.5 T, and identified decreased GM perfusion in primary and secondary progressive MS patients but not in RRMS patients.12 The RRMS patients in that study had a longer disease duration (median 10 years vs 2.4 years in our study) but low disability scores (median EDSS of 2.5), indicating that they were experiencing a generally favourable longer term disease course. About half were receiving β-interferon treatment, whereas only 20% of our cohort was receiving treatment. It is conceivable that the normal GM perfusion of the previously reported RRMS cohort reflects its favourable natural history and an effect of disease modifying treatment, although a controlled investigation of the effects of immunomodulatory treatments on perfusion has not been undertaken to date. In addition, the lower field strength may also have reduced sensitivity to detect abnormalities.
Although other studies have reported GM atrophy in early RRMS compared with age-matched healthy controls,7 ,26 ,27 the amounts of tissue loss have been small. The absence of atrophy in our cohort may reflect several factors, including the relatively small sample size, differences in image analysis algorithms used to measure GM volumes (although we also did not find atrophy using a second method with FSL software called SIENAX—data not presented), the short disease duration of the cohort (they have early RRMS) and their largely preserved neurological and cognitive functions (see table 1).
Mechanisms of reduced GM perfusion
There are several potential mechanisms for the decrease in GM perfusion. First, GM neuronal loss per se should be considered, since perfusion will be linked to total metabolic neuronal activity, which will be decreased when there is neuronal loss. However, neuronal loss would be expected to cause GM tissue volume loss, which was not observed. While it is possible that GM atrophy from neuronal loss has been partially masked by inflammation in GM lesions, as has been reported in early MS,28 the total cortical lesion load is likely to be small in relation to total GM volume in early RRMS,29 and thus unlikely to affect the latter substantially.
Second, there could be a primary, GM-based, disturbance of neuronal metabolic function, for example, due to inflammation with mitochondrial dysfunction triggered by macrophage-derived reactive oxygen and nitrogen species, as has been reported in experimental allergic encephalomyelitis in the absence of demyelination and in acute MS inflammatory WM lesions.30 Incidental cortical inflammatory lesions have been reported as a frequent finding in a large case series in which biopsies were performed to investigate tumefactive WM lesions in what proved to be early MS.28 Although neuroaxonal damage was generally mild in these cortical lesions,28 it seems plausible that neuronal metabolic function could be impaired.
Third, reduced GM perfusion may reflect neuronal metabolic dysfunction secondary to anterograde or retrograde degeneration of axons consequent on their transection in inflammatory WM lesions.31 However, there was no correlation between T2 or T1 (WM) lesion loads and GM perfusion suggesting that the latter may have occurred by a mechanism that is independent of WM lesions. Similarly, the absence of correlation between GM perfusion and WM volume does not support the role of more generalised WM axonal loss in causing reduced GM neuronal activity and consequent GM hypoperfusion.
Finally, a primary abnormality of cerebral vascular mechanism could contribute to the GM hypoperfusion.32 An increase in calcium is seen within neuronal and glial cells in MS lesions.33 The increase in calcium within astrocytes has been reported to cause constriction of blood vessels.34 An increase in the blood concentration of the endothelin-1 (ET-1), a vasoconstrictor compound, is also reported in MS.32 Additionally, reduced astrocyte energy metabolism has been reported to lead to a reduction in the arterial supply.32
Although the mechanisms for GM hypoperfusion remain uncertain, and may be multiple, the significant association between WM and GM hypoperfusion is noteworthy as it could reflect a common causal mechanism to account for at least a part of the hypoperfusion seen in both tissues. For example, inflammation-mediated mitochondrial dysfunction might reduce metabolic activity in both GM and WM. On the other hand, based on findings of a cross-sectional study of clinically isolated syndrome and RRMS patients, Varga et al11 have suggested that tissue hypoperfusion occurs earliest in WM and spreads to the GM as the disease progresses. Further studies, including serial observations, should help better understand the relationship between WM and GM perfusion abnormalities.
Correlation of GM perfusion with neurological and cognitive findings
Similar to the findings of Inglese et al14 in RRMS, GM perfusion did not correlate with disability measures (EDSS, MSSS). This probably reflects the early disease stage at which GM perfusion abnormalities are occurring. Significant voxelwise correlations with GM perfusion measures were observed only with memory z-score, which was the only cognitive function found to be reduced in our MS cohort. The functional interaction of neuronal networks makes it biologically plausible to detect associations in a large number of cortical and subcortical regions, as were observed. In a previous study, Inglese et al14 reported that deep GM perfusion abnormality in RRMS was significantly associated with visuospatial skills. Another study in RRMS reported a significant association between deep GM perfusion and fatigue.13 Considering the associations observed in these previous studies and our study together, it seems plausible that GM perfusion abnormalities reflect pathophysiological changes that contribute to cognitive deficits and/or fatigue in RRMS. However, further studies of larger cohorts who exhibit more marked cognitive impairments will be needed to definitively investigate the relationship of GM perfusion changes with cognitive impairment in MS.
Significance of reduced GM perfusion in early RRMS
With long-term follow-up, approximately two-thirds of early RRMS patients will eventually develop secondary progressive MS, marked by high disability and loss of GM tissue; others will remain a more benign group, with low levels of disability and relatively preserved GM tissue volume.35 T2 WM lesion load changes in the early years provide only a modest prediction of the long-term course of relapse–onset MS36 and it is uncertain whether or to what extent existing disease modifying treatments for RRMS alter the long-term disease course. It is therefore clear that a better understanding of early pathophysiological mechanisms and improved prediction of the long-term disease course are both much needed, as they may lead to new and effective long-term treatment strategies and identify patients for whom treatment is most needed. Detection of reduced GM perfusion in early RRMS, as we have found, suggests a potential for quantitative perfusion MRI to be a biomarker of clinically relevant early pathophysiology and to identify patients at risk of long-term disability through subsequent GM neuronal loss. However, further work is needed to confirm or refute such a potential role for perfusion MRI; larger cohort studies are needed to more definitively investigate the relationship of perfusion with concurrent neurological and cognitive deficits and longitudinal studies will be required to evaluate whether reduced perfusion predicts future GM atrophy and disability.
Some studies have reported hyperperfusion in WM12 and it has been suggested that this may reflect inflammation and an early metabolically active stage of lesion development. MS GM lesions are difficult to visualise on MRI and are also less inflammatory than WM lesions, although it is conceivable that focal areas of hyperperfusion might exist, especially in an early and more inflammatory stage of lesion evolution. Investigation of this possibility would require imaging sequences more sensitive to GM lesions, such as double inversion recovery29 and phase-sensitive inversion recovery37 and serial scanning to detect new lesions.
WM abnormalities in early RRMS
As reported at this stage of MS,26 our early RRMS cohort exhibited a decreased WM volume. In addition, they showed a decrease in WM perfusion. Previous studies using dynamic contrast-enhanced MRI have reported decreased WM perfusion in MS.8–11 The decrease observed in our cohort would be consistent with reduced metabolism due to neural tissue loss, as implied by the detection of WM loss. While our study has focused on early GM changes, these findings confirm that WM damage is an early feature of MS and emphasise the importance of therapy that also aims to prevent this aspect of MS pathology.
Other considerations
Reduced cortical perfusion using ASL has been reported with increasing age in men38 and in patients showing strong signs of drowsiness.39 MS more often affects women (the female to male ratio is 3:1 for RRMS), and a smaller number of men were included in our study. Local and global GM perfusion differences were assessed between early RRMS patients and healthy controls by adjusting for age and gender effects in the statistical analysis. We did not quantify drowsiness, and it could be an important additional parameter to monitor in future perfusion studies, for example, with an eye-tracking camera.39
Because the number of patients receiving a disease modifying treatment in our study was small, we did not adjust for this factor. However, the same analysis restricted to patients not receiving β-interferon therapy gave the same results; that is, GM hypoperfusion but no GM atrophy in RRMS patients when compared with healthy controls. It would be prudent to adjust for disease modifying treatments in future studies that include larger numbers on treatment, as the effects of such treatments on WM and GM perfusion abnormalities are unclear to date.
Furthermore, perfusion measurements will vary when different methods and scanners are employed, and it is important to establish reproducibility. The within-session retest reliability of the p-CASL sequence in our centre demonstrates excellent reliability and is similar to that reported in the literature40 (across eight healthy subjects not included in this study: mean difference in peripheral GM cerebral blood flow (CBF) between sessions: 0.5 (SD 2.3) mL/100 g/min; within-subject coefficient of variation (95% CI): 3.7% (2.0% to 5.5%); intraclass correlation coefficient (95% CI): 0.975 (0.893 to 0.995)). The differences between the MS and control groups (global GM/WM: 3.8/2.6 mL/100 g/min, ∼7%) were substantially greater than the retest variability (∼1%), suggesting that observed differences were due to disease and not a consequence of variability in the p-CASL sequence. Additionally, it will be pertinent to develop a standard methodology for perfusion imaging in future multicentre studies in MS. Lastly, currently available structural imaging techniques have a limited sensitivity in detecting cortical lesions; insofar as perfusion decreases in GM are a consequence of altered neuronal metabolism due to cortical lesions, perfusion imaging may provide insight into the extent of such lesions in vivo.
Conclusion
This study has shed light on early pathophysiological processes in the GM in RRMS by coupling structural and perfusion imaging modalities. Early RRMS patients with relatively preserved clinical and cognitive functions showed multiple regions with reduced GM perfusion, but no GM volume loss. Larger cross-sectional studies with neurological and cognitive correlations and longitudinal follow-up studies are required to ascertain the functional and prognostic significance of early GM perfusion abnormalities in RRMS.
References
Footnotes
-
Contributors All authors have made substantial contributions to all of the following: (1) the conception and design of the study, or acquisition of data, or analysis and interpretation of data, (2) drafting the article or revising it critically for important intellectual content and (3) final approval of the version to be submitted. Moreover, each of the authors has read and concurs with the content of the present manuscript.
-
Funding This work was supported by the New Zealand Brain Research Institute.
-
Competing interests DHM is also supported by the UCL-UCLH Biomedical Research Centre.
-
Patient consent Obtained.
-
Ethics approval Lower South regional ethics committee of New Zealand.
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
Data sharing statement To our knowledge, this is the first study to assess perfusion abnormalities using p-CASL in early RRMS patients and to combine structural and perfusion imaging modalities to elucidate pathophysiological processes in the GM in RRMS. As corresponding author, I (Laetitia Debernard) take full responsibility for the data, the analyses and interpretation and the conduct of the research; that I have full access to all of the data and that I have the right to publish any and all data separate and apart from any sponsor. This manuscript is not under review at any other publication.