Article Text

Abstract
Background Increased titres of serum IgM antibodies to GM1 ganglioside are often associated with multifocal motor neuropathy (MMN). Testing for IgM antibodies to other antigens including GM2, the mixture of GM1 and galactocerebroside (GM1/GalC) and the disulfated heparin disaccharide NS6S were reported to increase the sensitivity of antibody testing in MMN even if it is unclear whether the specificity and positive (PPV) or negative predictive value (NPV) for MMN were also affected.
Methods We measured IgM antibodies to GM1, GM2, galactocerebroside, GM1/GalC and NS6S in 40 consecutive patients with MMN and 142 controls with other neuropathies or related diseases and compared their sensitivity, specificity and PPV for MMN.
Results With the only exception of anti-GM2 and, partially, anti-NS6S antibodies, IgM antibodies to the antigens tested were more frequent in MMN than in controls. Increased titres of anti-GM1 IgM were found in 48% of MMN patients with a specificity of 93% and PPV for MMN of 66%. Anti-GM1/GalC antibodies were present in all anti-GM1 positive MMN patients and in 11 additional patients (28%) with MMN raising the sensitivity of antibody testing to 75%. The specificity (85%) and PPV (59%) for MMN was, however, moderately reduced compared to anti-GM1 IgM, even if they rose with increasing anti-GM1/GalC titres. IgM antibodies to GM2, NS6S and galactocerebroside were found in 8%, 23% and 60% of MMN patients but had a low specificity and PPV for MMN.
Conclusions Testing for anti-GM1/GalC IgM significantly increased the sensitivity of antibody testing in MMN compared to anti-GM1 alone (p=0.021) and may represent a preferred option for GM1 reactivity testing in MMN.
- Neuropathy
- Neuroimmunology
- Ganglioside
Statistics from Altmetric.com
Introduction
Multifocal motor neuropathy (MMN) is a purely motor neuropathy (MN) characterised by asymmetric limb weakness predominant in the upper limbs and multifocal conduction blocks (CB) on motor nerves.1 ,2 Several data suggest that MMN is an immune-mediated neuropathy including the usually good response to treatment with high-dose intravenous immunoglobulin (IVIg).3 After the original report,4 high titres of IgM antibodies to the ganglioside GM1 have been frequently reported in MMN, where they have been detected in 40% to 50% of the patients.5–9 The diagnostic relevance and pathogenic role of these antibodies in MMN remains, however, unclear since these antibodies are not specific for MMN and are sometime encountered in patients with other immune neuropathies or with motor neuron disease (MND).1 ,10 ,11 IgM antibodies to other neural antigens have been reported in MMN including the ganglioside GM2,12–14 the mixture of GM1 with galactocerebroside with15 or without16 cholesterol and the disulfated heparin disaccharide NS6S.17 Testing for these antibodies was reported to increase the sensitivity of antibody testing in MMN even it is unclear how this affected the specificity and positive predictive value (PPV) for MMN. We compared the sensitivity, specificity and PPV and negative predictive value (NPV) for MMN of IgM antibodies to GM1, GM2, galactocerebroside, the mixture of GM1 with galactocerebroside (GM1/GalC) and NS6S.
Methods
Patients
We retrospectively analysed the sera from patients with MMN, other immune or non-immune-mediated neuropathies and related diseases and normal subjects (NS) recruited and tested for anti-nerve antibodies at our Neuropathy Clinics since 2004. All patients had serum collected at the time of other blood tests, and they all consented to its use for research. Sera were kept frozen at −20°C until used. The Ethic Committee of Humanitas Clinical and Research Institute, Rozzano, Milan, Italy, approved this retrospective study. French patients signed an informed consent to have their sera sent to Italy for antibody testing. There was no need according to French law for Ethic Committee approval for retrospective study on stored sera. All the patients were diagnosed in our Centres at the time and on the basis of clinical and electrophysiological assessment. Forty consecutive patients including 20 from France had definite or probable MMN according to the criteria of the European Federation of Neurological Societies and the Peripheral Nerve Society (EFNS/PNS).18 Thirty-eight consecutive Italian patients had definite or probable chronic inflammatory demyelinating polyradiculoneuropathy (CIDP) according to the criteria of the European Federation of Neurological Societies and the Peripheral Nerve Society.19 We also tested 26 patients with neuropathy associated with IgM monoclonal gammopathy with high titres (1:6400 or more) of IgM antibodies to the myelin-associated glycoprotein (MAG),8 30 with definite or probable MND according to the revised El Escorial criteria,20 48 with neuropathy of other or of undetermined causes and 20 NS. All patients with MND had been clinically and electrophysiologically examined to exclude a multineuropathic distribution of weakness and the presence of CB on motor nerves. Similarly, the diagnosis of all patients with increased antibody titres was reconfirmed after revising the clinical and electrophysiological data.
Methods
Patients’ sera were tested by ELISA for IgM reactivity to the gangliosides GM1 and GM2 (0.2 μg/well in ethanol of each ganglioside),8 to galactocerebroside (2 μg/well in ethanol), to a 1:10 mixture of GM1 (0.2 μg) and galactocerebroside (2 μg/well)(GM1/GalC),15 and to the disulfated heparin disaccharide NS6S (α-4-deoxy-1-threohex-4-enopyranosyluronic acid-[1-4]-d-glucosamine-S-6S; IdoA-GlcNS-6S) (0.5 μg/well in 0.05% N-hydroxysuccinimide) (all from Sigma). The remaining procedure was the same used for our current testing for anti-GM1 IgM antibodies.8 Sera where considered positive when the optical density (OD) difference between wells coated with the antigen and bovine serum albumin exceeded 0.050 for GM1, GM2, galactocerebroside and GM1/GalC, and 0.100 for NS6S. Sera were initially tested at serum dilution of 1:640, and positive sera were subsequently tested against reactive antigens by serum twofold dilutions until they became negative. Since in our laboratory testing the sera for anti-GM1 IgM antibodies at 1:640 dilution sometime provided variable data with a few sera with low reactivity ranging between being marginally positive (OD reading around 0.050 to 0.070) or negative (OD around 0.030 to 0.050) and the same was observed at the same dilution for anti-GM1/GalC antibodies, we subsequently examined all the sera starting at the serum dilution of 1:1280. IgM reactivity with the mixture GM1/GalC was defined when it was detected at at least a twofold serum dilution higher than that obtained with galactocerebroside. All the test were done by the same trained biologist with a long-lasting experience in testing for antiglycolipid antibodies and who was not aware of the clinical diagnosis. All the test were repeated twice and repeated a third time if results were discordant (difference in at least twofold serum dilution) and were performed between 2010 and 2012. Following a more recent report,16 sera from 30 patients with MMN including 10 without anti-GM1/GalC IgM were subsequently tested for IgM reactivity to a 1:1 mixture of GM1 (0.2 μg) and galactocerebroside (0.2 μg/well) and the results were compared to those observed in the same experiment with a 1:10 mixture of GM1/GalC.
Statistical analysis
We estimated the diagnostic accuracy by comparing the sensitivity, specificity and PPV and NPV for MMN of each antibody. Sensitivity was determined as the proportion of positive patients among patients with MMN, specificity, as the proportion of negative patients among patients without MMN.21 The PPV corresponds to the proportion of patients with MMN among total patients with a specific IgM antibody.21 The NPV corresponds to the proportion of controls without a specific antibody among total patients with MMN and controls without that antibody.21 In all these calculations, only controls with other neuropathies or related diseases were considered. The statistical analysis on the different frequency of each of these antibodies in MMN compared to controls and of the frequency of each antibody in MMN was calculated by Fisher's exact test using Graph Pad software. Statistical significance was defined as p values less than 0.05. The area under the curve (AUC) was calculated for each antibody to assess their discriminating value in the comparison between MMN and controls. AUC values rely on ROC (receiver operating characteristic) curves which illustrate the performance of a classifier system plotting the true positive rate versus the false positive rate at various threshold settings of each antibody separately. AUC values ranged from 0.5 (no discriminative power) to 1 (perfect discriminative power).
Results
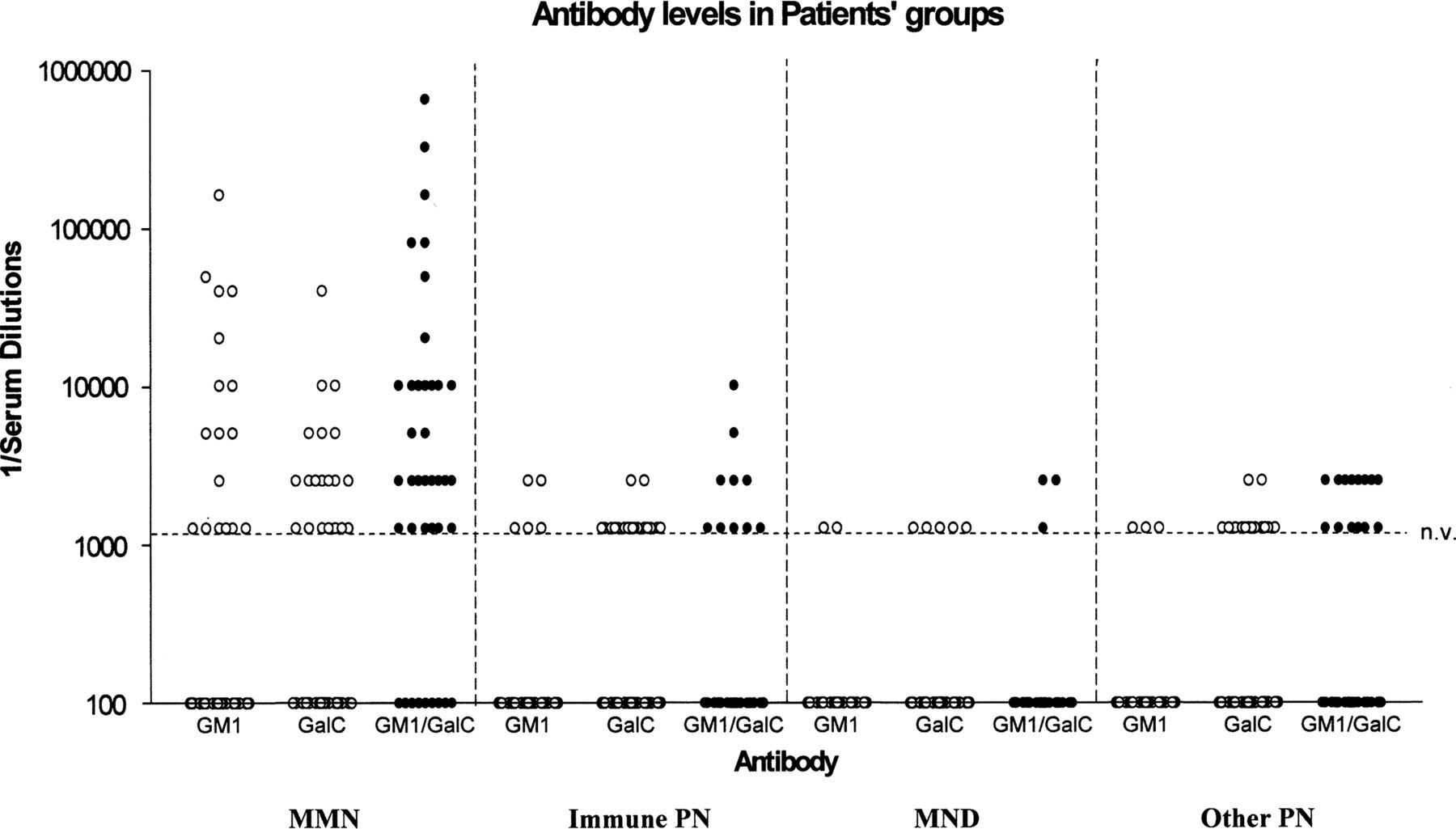
We found increased titres (1:1280 or more) of IgM antibodies to GM1 in 19 out of 40 (48%) patients with MMN, 10 out of 142 (7%) disease controls (p<0.0001) and in no normal subject (figure 1). Among the positive controls, four (11%) had CIDP, two (7%) had MND, one (4%) had PN-IgM and three (6%) had other neuropathies. When compared to individual control groups, MMN patients had more frequently anti-GM1 IgM than patients with MND (p<0.0002), immune-mediated neuropathies (CIDP and PN-IgM) (p<0.0001) and other neuropathies (p<0.0001). All but two controls with CIDP, who had titres of 1:2560, and eight patients with MMN had titres of 1:1280 while the remaining 11 MMN patients had higher titres (figure 1). The sensitivity, specificity and PPV and NPV for MMN of anti-GM1 IgM and of the other antibody tested are summarised in table 1.
Antibody testing in MMN

IgM antibody titres by ELISA to GM1, galactocerebroside (GalC) and the mixture of GM1 and galactocerebroside (GM1/GalC) in the sera of patients with multifocal motor neuropathy (MMN), immune neuropathies, including chronic inflammatory demyelinating polyradiculoneuropathy and neuropathy associated with anti-myelin-associated glycoprotein (MAG) IgM, motor neuron disease (MND) and neuropathy of other causes (Other PN). Sera were tested at the initial serum dilution of 1:1280 and titrated by serum twofold dilutions. The reverse of serum dilution is indicated in the axis. Patient with titres of 1:1280 or more (dotted line; n.v.: normal value) were considered to be positive for the antibody tested. Reactivity to GM1/GalC was considered to be positive when it was detected at at least twofold serum dilution higher than reactivity to galactocerebroside alone.
Increased titres of anti-GM2 IgM antibodies were only found in three out of 40 (8%) patients with MMN (1:1280 in two and 1:2560 in one), and three controls (p=0.12), including two with CIDP (5%) (1:10 240 in one and 1:5120 in the other) and one with other neuropathies (2%)(1:1280). When compared to individual patients’ group, anti-GM2 IgM was not more frequent in MMN than in any other groups (p>0.05 in all comparison). Even if these antibodies were infrequent, their specificity was high (98%) while their PPV for MMN was 50% (table 1).
IgM antibodies to the heparin disaccharide NS6S were more frequent in patients with MMN (9/40; 23%; 1:1280 in all) than in the whole group of disease controls (14/142; 10%; 1:1280 in all but three patients with anti-MAG IgM who had titres of 1:2560), but the difference was not significant (p=0.053). The difference became significant when MMN was compared to MND (p=0.035), other neuropathies (p=0.019) but not other immune neuropathies (p=0.61). The PPV value for MMN of these antibodies was 39% (table 1). Testing for these antibodies in addition to anti-GM1 IgM slightly increased the sensitivity of antibody testing in MMN compared to anti-GM1 testing (from 48% to 55%) but also reduced their specificity (from 95% to 85%) and PPV for MMN (from 66% to 51%).
IgM antibodies to galactocerebroside were found in 22 out of 40 (55%) patients with MMN but also in 39 out of 142 (28%) controls (p=0.002) (figure 1) and in one normal subject (titre 1:1280) (5%). These antibodies were more frequent in MMN patients compared to MND (13%; p=0.0004), other immune (30%; p=0.014) or non-immune neuropathies (p=0.049). The frequency of this antibody in MMN patients was not significantly higher than that of anti-GM1 IgM (p=0.65). The relative high frequency of these antibodies in controls resulted in a low PPV of a positive test for MMN (36%) (table 1).
IgM antibodies to GM1/GalC were found in 30 out of 40 (75%) patients with MMN and in 21 out of 142 (15%) disease controls (p<0.00001) (figure 1) and in no normal subject. Of the 30 MMN patients with anti-GM1/GalC antibodies, 19 also had high anti-GM1 IgM including four with the same titre while 15 had twofold (seven patients), fourfold (four patients) or eightfold or more (four patients) higher titre of anti-GM1/GalC than anti-GM1 IgM (figure 2). None of the MMN patients with anti-GM1 IgM did not have a concomitant reactivity to GM1/GalC or had a lower reactivity to it. Anti-GM1/GalC antibodies were more frequent in MMN than in each patient's groups (p<0.00001 in all). In patients with MMN, they were significantly more frequent than anti-GM1 IgM (p=0.021). This difference did not remain significant when the four patients with the same titre of anti-GM1 IgM were excluded from the anti-GM1/GalC group (p=0.18). In MMN patients, anti-GM1/GalC IgM titres ranged from 1:1280 to 1:640 000 (figure 1) and were higher than 1:1280 in 24 patients (60%; p<0.00001 compared to 8% of controls) and higher than 1:2560 in 16 patients (40%; p<0.00001 compared to 1% of controls). The PPV of anti-GM1/GalC IgM for MMN was 59% and rose to 67% with titres above 1:1280 and to 89% above 1:2560 (table 1). When we verified whether testing for antibodies to GM1/GalC in 1:1 or in 1:10 proportion provided different results in 30 MMN, none of the ten patients without anti-GM1/GalC (1:10) IgM had antibodies to GM1/GalC (1:1). Of the remaining 20 patients with anti-GM1/GalC (1:10) IgM, 12 patients had the same titre anti-GM1/GalC (1:1) and anti-GM1/GalC (1:10) IgM, seven had twofold higher titre of anti-GM1/GalC (1:10) and only one of anti GM1/GalC (1:1) IgM.

Comparison of IgM reactivity to GM1, galactocerebroside (GalC) and the mixture of GM1 and galactocerebroside (GM1/GalC) in two representative patients with multifocal motor neuropathy (MMN). Sera were tested staring at 1:1280 or 1:2560 serum dilutions and subsequently titrated at fourfold serum dilutions. In both patients, IgM reactivity to GM1/GalC was consistently higher at each serum dilution than reactivity to GM1 and galactocerebroside alone and persisted when it had disappeared for GM1 and galactocerebroside. Optical density absorbance indicated in the axis.
In figure 3 are represented the ROC curves and reported AUC values for MMN versus disease controls for each antibody separately. The saturate model reported a high value of AUC (0.89), mostly driven by anti-GM1/GalC AUC value (0.83). Anti-GM2 and anti-NS6S reported irrelevant AUC values (0.54 and 0.58, respectively), while anti-galactocerebroside had slight (AUC=0.67) and anti-GM1 moderate (AUC=0.71) discriminative powers.

{kind=link}
{kind=link}
{kind=link}
Receiver operating characteristic (ROC) curves and reported area under the curve (AUC) values for multifocal motor neuropathy (MMN) versus disease controls for each antibody separately. The saturate model (Model: all antibodies together) reported a high value of AUC (0.89), almost totally driven by the anti-GM1/GalC AUC value (0.83). Anti-GM2 and anti-NS6S reported irrelevant values (AUC=0.54 and 0.58, respectively). Anti-galactocerebroside (GalC) had a slight (AUC=0.67) and anti-GM1, a moderate (AUC=0.71) discriminative power.
Discussion
In this study, we examined the frequency, specificity and PPV and NPV for MMN of a few antibodies that have been associated with MMN. With the exception of anti-GM2 IgM and, when compared to some controls’ groups, of anti-NS6S IgM, these antibodies were more frequent in patients with MMN than in patients with other immune or non-immune neuropathies, MND and NS confirming their previously reported association with MMN. When we analysed the possible contribution to the diagnosis of MMN of these antibodies in comparison with anti-GM1 IgM, only testing for anti-GM1/GalC significantly improved the sensitivity of antibody testing. The increased sensitivity was, however, associated with a reduced specificity and PPV for this diagnosis that was partially compensated by the close association of high anti-GM1/GalC titres with MMN. When we considered antibody values rather than only their presence/absence using ROC analysis, we could confirm a high level of validity of anti-GM1/GalC IgM. Testing for anti-GM2, anti-NS6S and anti-galactocerebroside IgM revealed these antibodies in 8% to 55% of patients with MMN. No more than 50% of the patients with a positive test had, however, MMN so that the diagnostic usefulness of these antibodies in MMN resulted to be quite limited.
In his original report, Pestronk et al17 reported that testing for IgM antibodies to the NS6S heparin disaccharide increased the sensitivity of antibody testing from 43% to 64% compared to anti-GM1 IgM in patients with MN including patients with MMN. They also found an increased positivity from 0% to 21% in patients with sensory neuropathy. The PPV for MN of anti-NS6S antibody was 73% compared to the PPV of 100% for anti-GM1 IgM. In that study, patients with CIDP and MND were negative for both reactivities. Studies from several other centres reported, however, that 5% to 10% of patients with MND and a minor proportion of those with CIDP also have anti-GM1 IgM.5 9 11 We confirmed the significant association of anti-NS6S antibodies with MMN and also found that testing for these antibodies in addition to anti-GM1 IgM slightly increased the sensitivity of antibody testing in MMN. The specificity and PPV for MMN of these antibodies and of their combination with GM1 was, however, consistently reduced compared to anti-GM1 IgM. Pestronk et al15 also showed that testing for IgM antibodies to GM1 in addition to cholesterol and galactocerebroside in patients with MMN increased the sensitivity of IgM testing to GM1 alone from 43% to 62% (19% increase). The authors tested the reactivity to GM1/GalC using the same proportion of antigen of 1:10 that we used in our study. They did not find any reactivity to this mixture in a series of 525 patients with other neuropathies or motor system disorders. Similar results were recently reported by Galban-Horcajo et al16 who found that testing by ELISA for IgM reactivity to GM1 and galactocerebroside in a 1:1 proportion increased the sensitivity of antibody testing in MMN from 67% to 88% (21% increase). In addition when they used a new combinatorial glycoarray system, all patients with MMN had antibodies to GM1/GalC. None of their controls had this reactivity but they only examined 30 neurological controls including only six patients with other neuropathies and three with MND. Despite the different methodology used in our ELISA system, we observed a similarly increased frequency of IgM reactivity to GM1/GalC compared to GM1 alone (48% to 75%; 27% increase). This high prevalence was significantly higher than observed in 142 patients with different forms of immune-mediated or non-immune-mediated neuropathies and MND (15%) even if it was associated with a moderate reduction of their PPV for MMN (59%) compared to anti-GM1 (66%). Testing for antibodies to GM1/GalC in 1:1 or in 1:10 proportion did not provide additional positive data among our MMN patients.
As was previously postulated for anti-ganglioside complex antibodies,22 ,23 it is possible that the mixture of GM1 with galactocerebroside leads to the formation of a new antigen recognised by patients’ IgM. All our patients with MMN with anti-GM1 IgM also had anti-GM1/GalC IgM that in most patients were found in higher concentration (figure 2). In addition, the remaining patients with anti-GM1/GalC had anti-GM1 IgM titres (1:320) lower than the initial serum dilution used in our assay (data not shown). We therefore think that more than the formation of a new antigen, the combination of these glycolipids leads to a better binding or exposure of GM1 in ELISA plates facilitating antibody detection. It is possible that IgM binding to GM1 in an ELISA system only partially reflect the binding capacities of these antibodies and that this might be improved using a system theoretically more consistent with the expression of GM1 on neural membranes.
The increased frequency of the examined antibodies in MMN compared to controls further supports the hypothesis of an immunological involvement in MMN.1 ,2 In addition, this study confirms the close, though not invariable, association of MMN with IgM reactivity with GM1 either when tested alone or in combination with galactocerebroside. The possible pathogenic relevance of this association is beyond the aims of this study and was addressed in other studies.1 ,2 The increased detection of this reactivity by testing for anti-GM1/GalC antibodies may help, however, in the diagnosis of patients with an unclear presentation and should be considered as preferred option for testing for GM1 reactivity in MMN patients.
Acknowledgments
We wish to thank Dr Francesca Gallia and Dr Fabrizia Terenghi (2° Neurology, Humanitas Clinical and Research Centre, Rozzano, Milan, Italy) and Dr Raquel Guimaraes Costa (National Reference Centre for Neuromuscular Disease, the University Hospital Pitié-Salpêtrière, Paris, France) for helping in collecting and reviewing the clinical data.
References
Footnotes
-
Collaborators Francesca Gallia, Raquel Guimaraes Costa.
-
Contributors EN-O designed and supervised the study, interpreted the results and drafted the manuscript; CG analysed and interpreted the data; LM and J-ML participated in the design of the study and J-ML also in drafting the manuscript; PM performed statistical analysis and participated in the analysis and interpretation of the data.
-
Funding The work was made possible by the financial support of Humanitas Clinical and Research Centre, Rozzano, Milan, Italy and by a Grant (Ricerca Finalizzata 2007) from the Italian Ministry of Health.
-
Competing interests There were no competing interests in the preparation of this study. E Nobile-Orazio acted as ad-hoc consultant for Baxter, CSL Behring, Kedrion and Novartis. He received personal compensation for lecturing from Baxter, CSL Behring, Kedrion and Grifols, and travel grants to attend Scientific Meetings from Baxter, Grifols, Kedrion and Novartis. C Giannotta, L Musset and P Messina have no conflict of interest. J-M Léger received departmental research grants or honoraria from Biogen-Idec, Baxter, CSL Behring, LFB, Novartis and Octapharma.
-
Patient consent Obtained.
-
Ethics approval Institutional Review Board, Humanitas Clinical Institute.
-
Provenance and peer review Not commissioned; externally peer reviewed.