Article Text

Abstract
Background Depression is a common neuropsychiatric symptom in Parkinson's disease (PD). In previous research, PD-related depression was associated with striatal dopaminergic deficits, presumably due to degeneration of brainstem dopaminergic projections. Segregated areas of the striatum are crucially involved in various parallelly arranged cortical-striatal-thalamocortical circuits and serve functions in, among others, motor control or emotion. This suggests regional specificity of dopaminergic deficits in the striatum in motor and depressive symptoms in PD.
Methods In this cross-sectional retrospective study, we correlated severity scores of depressive and motor symptoms in 100 non-demented PD patients (median Hoehn & Yahr stage: 2) with dopamine loss in specific regions of the striatum as measured by [123I]FP-CIT SPECT tracer binding to the dopamine transporter (DaT).
Results Depressive symptoms were related to lower DaT binding in the right caudate nucleus, while motor symptoms were associated with decreased DaT binding in the right putamen. This double dissociation was most pronounced in early-stage PD patients.
Conclusions These results suggest that depressive symptoms in PD are associated with dopamine loss in the caudate nucleus, possibly related to degeneration of dopaminergic projections from the ventral tegmental area, while motor symptoms are associated with low dopamine signalling to the putamen and loss of nigrostriatal projections. This is consistent with the neuroanatomy of partially segregated cortical-striatal-thalamocortical circuits and supports the role of dysfunctional associative and motivational circuits in PD-related depression.
- Parkinson's Disease
- Depression
- Spect
Statistics from Altmetric.com
Introduction
Depression is a common non-motor symptom of Parkinson’s disease (PD), with a prevalence of around 35%1 and an increasing incidence with progression of the disease.2 PD is characterised by a gradual loss of nigrostriatal dopaminergic projections, with a relative sparing of projections to the caudate nucleus.3 ,4 SPECT and PET tracers that bind to the dopamine transporter (DaT) in the presynaptic terminal of dopaminergic projections are routinely used to measure the integrity of these neurons. The majority of previous studies have shown a negative correlation between dopaminergic signalling in the striatum and depressive symptoms,5–8 although conflicting results have also been reported.9 ,10 These results fit the conceptualisation of PD-related depression as a hypodopaminergic state of the striatum,7 although the noradrenergic7 ,11 and serotonergic systems12 are also involved. The striatum is a crucial way station in each of the parallel cortico-striatal-thalamocortical circuits in which dopamine is a major neuromodulator.13 ,14 The putamen is involved in sensorimotor functions through its connections with the primary motor cortex, somatosensory cortex and premotor area.14 The caudate nucleus, on the other hand, is involved in associative functions, motivation and reward, and receives input from multiple prefrontal regions, the hippocampus and amygdala.15 ,16 This suggests region-specific effects of dopamine loss in the striatum on either motor or depressive symptoms, although no study has yet investigated this. Here we examined [123I]FP-CIT ([123I]N-ω-fluoropropyl-2β-carbomethoxy-3β-(4-iodophenyl)nortropane) SPECT scans from relatively early-stage PD patients and hypothesised that depressive symptoms would be associated with lower DaT binding in the caudate nucleus due to its role in motivation and reward.
Methods
Subjects
We retrospectively obtained clinical and imaging data through the outpatient clinic for movement disorders of the VU University Medical Center (VUmc) in Amsterdam. Data were acquired between May 2008 and December 2011. All included patients were non-demented (Mini Mental State Examination (MMSE) score >24), had an abnormal [123I]FP-CIT SPECT scan and were diagnosed clinically with idiopathic PD by movement disorder specialists (HWB, EMJF), according to the diagnostic criteria of the UK PD Society Brain Bank.17 All patients on antidepressants were excluded from analyses, (1) because of their influence on [123I]FP-CIT SPECT tracer binding (eg, escitalopram, paroxetine, clomipramine and venlafaxine)18 and (2) so as not to bias the results with (partially) treated depression. A flow chart of patients is presented in figure 1. This study was approved by the medical ethical committee of the VUmc and all patients provided written informed consent to use their medical data for scientific purposes.

Flow chart of patients included in this study.
Measurements
We assessed disease severity in the ON-state with the Unified Parkinson's Disease Rating Scale part III (UPDRS-III) and disease stage with the modified Hoehn & Yahr scale (H&Y). The MMSE was used to evaluate the presence of dementia. We assessed the severity of depressive symptoms with Beck's Depression Inventory (BDI). All clinical evaluations were performed on the day of acquisition of SPECT scans. The levodopa equivalent daily dose (LEDD) was calculated by the method described previously.19
SPECT imaging
We used [123I]FP-CIT to measure presynaptic striatal DaT density. All patients received potassium perchlorate orally to block thyroid uptake of free radioactive iodide. Three hours before image acquisition [123I]FP-CIT was injected intravenously at an approximate dose of 185 MBq (specific activity >185 MBq/nmol; radiochemical purity >99%). Subjects were imaged using a dual-head gamma camera (model E.Cam; Siemens, Munich, Germany) with a fan-beam collimator. We acquired 60×30 s views per head over a 180° orbit on a 128×128-pixel matrix resulting in a total imaging time of 30 min. Image reconstruction was performed using a filtered back projection with a Butterworth filter (order 8, cut-off 0.6 cycles/cm). Scans were reoriented manually to ensure that the left and right striatum were aligned.
Data analyses
Individual SPECT images were analysed using a standard template with five fixed-size regions of interest (ROIs) for the left and right head of caudate nucleus, left and right putamen and occipital cortex. Mean counts per ROI for three adjacent axial SPECT slices were used to calculate average counts for all five ROIs. Binding ratios (BRs) of specific to non-specific DaT binding were calculated for the left and right putamen and head of the bilateral caudate nuclei, using the occipital cortex as a reference area. Image analysis was performed with the region ratio software of the E.Cam (Esoft, version Syngo VE2B, Siemens, Erlangen, Germany) and statistical analyses with SPSS V.20.0 (Statistical Package for Social Sciences, IBM, Armonk, New York, USA). Not all outcome measures met the assumptions required for parametric testing. When appropriate, non-parametric tests are therefore reported. The relation between BDI score and striatal BRs was analysed using Pearson's r and partial Pearson's r with correction for age and UPDRS-III score. The correlations with LEDD score and disease duration were analysed with Spearman's r (rs). We also performed multiple regression analysis. Since DaT availability declines with natural ageing,20 age was entered in the first block and UPDRS-III and BDI scores simultaneously in the second block to examine the association with DaT BR beyond the association of age with DaT BR alone. Because our sample consisted of both medicated and unmedicated PD patients, we checked whether medication status influenced our findings. We therefore added the use of dopamine replacement therapy as a dichotomous predictor to the second block of the multiple regression analysis. Furthermore, to account for other possible confounding factors we also entered gender and motor predominance into the second block of a separate multiple regression analysis. These same analyses were also performed in a subsample of early-stage PD patients (H&Y ≤2; N=65) to reduce the influence of motor disability on depression scores. All assumptions of multiple regression analyses were met, including normality of the residuals and homoscedasticity. Statistical significance was set at p<0.05. We also conducted a post hoc voxel-based analysis using Statistical Parametric Mapping 8 (SPM8) software (Wellcome Trust Center for Neuroimaging, London, UK). This method is described in the online supplementary content (eMethods).
Results
Of the 128 available patients, 28 were excluded: 11 due to technical problems during the [123I]FP-CIT SPECT scan and 17 patients had incomplete or invalid clinical data, leaving 100 scans for analyses. Demographics are shown in table 1. Age correlated negatively with BRs in the right putamen (r=−0.27, p=0.007), right caudate nucleus (r=−0.30, p=0.003) and left caudate nucleus (r=−0.30, p=0.003). The correlation between age and BR in the left putamen did not reach statistical significance (r=−0.20, p=0.05). Age correlated positively with the UPDRS-III score (r=0.31, p=0.002) but not with the BDI score (r=−0.02, p=0.82). BDI scores correlated positively with motor severity (UPDRS-III scores; r=0.26, p=0.008) but not subjective disease duration. In patients on dopaminergic medication (N=40), LEDD correlated positively with disease duration (rs=0.67, p<0.001), but not UPDRS-III or BDI score.
Sample characteristics
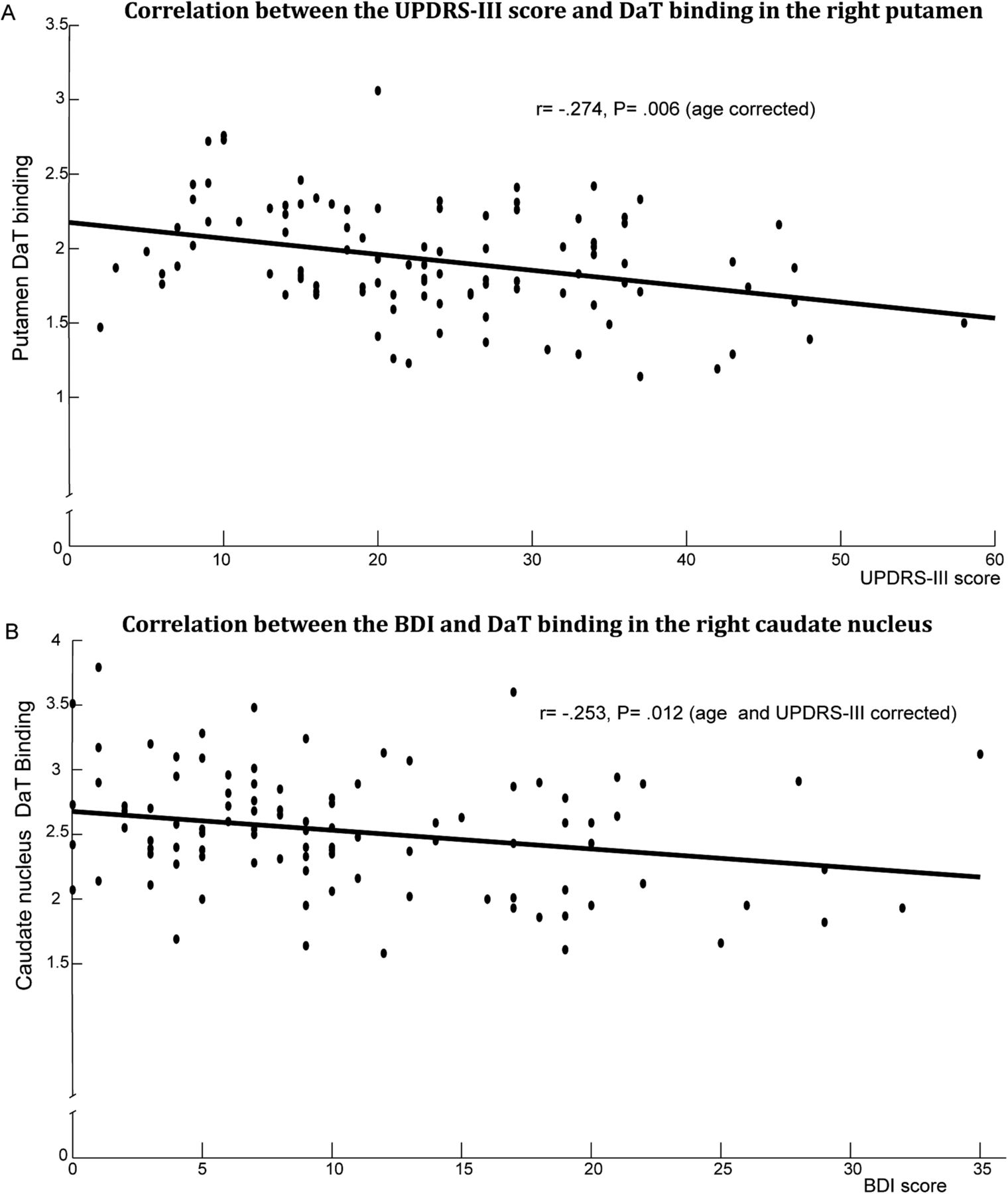
UPDRS-III scores correlated negatively with DaT BR in all four ROIs (right putamen: r=−0.34, p=0.001, left putamen: r=−0.22, p=0.03, right caudate nucleus: r=−0.25, p=0.01, left caudate nucleus: r=−0.20, p=0.04). After controlling for age, only the association with the right putamen remained significant (r=−0.27, p=0.006; see figure 2A).

{kind=link}
{kind=link}
Scatter plots showing associations between clinical scales and dopamine transporter binding. (A) Scatter plot and trend line of the motor severity as measured by the Unified Parkinson's Disease Rating Scale part III and dopamine transporter (DaT) binding ratio in the right putamen. (B) Scatter plot and trend line of the severity of depressive symptoms as measured using Beck's Depression Inventory and dopamine transporter (DaT) binding ratio in the right caudate nucleus.
Severity of depressive symptoms correlated negatively with DaT BR in the right caudate nucleus (r=−0.27, p=0.007), but not in any of the other three ROIs. This association persisted after controlling for age and UPDRS-III score (r=−0.25, p=0.01; see figure 2B).
The multiple regression analysis showed that the BDI score was significantly associated with DaT BR in the right caudate nucleus (β=−0.25, p=0.01) even after accounting for the effect of age on DaT BR. The BDI score showed no association with DaT BR in the right putamen (β=−0.13, p=0.19). Conversely, the UPDRS-III score was significantly associated with DaT BR in the right putamen (β=−0.26, p=0.03) but not in the right caudate nucleus (β=−0.09, p=0.38). The multiple R2 of the full model was 0.17 for the right caudate nucleus (ΔR2=0.08 with step 1 ‘age’ model, F(2,96)=4.54, p=0.01) and 0.15 for the right putamen (ΔR2=0.08, F(2,96)=4.41, p=0.02). BDI and UPDRS-III were not associated with DaT BR in the left caudate nucleus and left putamen beyond the effect of age alone on DaT BR (see table 2). Adding the side of motor symptoms or gender as possible confounding factors to the second step of the multiple regression analysis did not affect the results, neither did the use of dopamine replacement therapy. Furthermore, the analyses in early-stage PD patients, to reduce the influence of motor disability on depression, indeed showed that the correlation between UPDRS-III and BDI was no longer significant, nor was the correlation between age and UPDRS-III. All other reported correlations remained significant (see etable 1). The double dissociation between motor and depressive symptoms on DaT BR in respectively the right putamen and the right caudate nucleus remained (see table 2).
Multiple regression analyses
Lastly, we conducted a voxel-based analysis using SPM software. The results of this analysis showed a similar segregation between depressive and motor symptoms within the striatum. Further details are provided in eResults and efigure 1 in the online supplementary content.
Discussion
Our findings confirm the hypothesis that lower dopamine signalling in the caudate nucleus, as measured by a decline in [123I]FP-CIT binding, is associated with depressive symptoms in PD. Conversely, lower dopamine signalling in the putamen relates to increased motor symptoms. These findings were corroborated by our analyses using SPM.
Our results are in accordance with previous studies on depressive symptoms and striatal DaT binding.5–8 Nonetheless, none of these studies examined region-specific effects of dopamine loss in the striatum on the motor and depressive symptoms in PD. A lack of motor scores,8 a small sample size or a long time interval between acquisition of the scan and clinical evaluation6 may have precluded this examination in some of these studies. Another important methodological difference between previous studies and the present is the exclusion of patients on medication that can influence the binding of the SPECT tracer to DaT. Selective serotonin reuptake inhibitors (SSRIs) or serotonin-norepinephrine reuptake inhibitors (SNRIs) are known to increase the [123I]FP-CIT BR by approximately 10%.18 This may not hinder the interpretation of qualitative assessments for clinical purposes, but does significantly influence the quantification of DaT binding,18 precluding unambiguous comparisons.
The association between depressive symptoms and decreased [123I]FP-CIT BR was lateralised and involved only the right caudate nucleus. In contrast, previous DaT SPECT studies in PD primarily reported left-sided associations.6 ,8 Unfortunately, none of these studies reported whether there was an association between the predominance of motor symptoms and depressive symptoms. In our study, neither patients with a left-sided motor predominance nor those with a right-sided motor predominance were more likely to have depressive symptoms (data not shown). In addition, incorporating motor predominance into the multiple regression analyses did not significantly alter the results. This suggests that the left or right predominance of motor symptoms does not influence the association between depressive symptoms and [123I]FP-CIT binding. This is consistent with previous research that showed that motor predominance does not affect depression or other non-motor symptoms.21 Mixed results on the lateralisation of depressive symptoms are also evident in non-PD samples, with some studies showing right-lateralised dysfunction,22 while others showed left-lateralised dysfunction.23 More research is therefore warranted on the lateralisation of depressive symptoms in both PD and non-PD samples.
The association between motor symptoms and putaminal [123I]FP-CIT BR was also right lateralised even though the majority of our sample showed a right motor predominance and the lowest BR in the contralateral left putamen. Previous studies have shown robust correlations between DaT binding in the ipsilateral putamen and motor impairments but weaker or absent correlations for the contralateral and more affected putamen.24–26 This apparent paradox in these studies and the present results is most likely explained by a restricted range in both the BR in the most affected putamen and motor scores in the contralateral body side, weakening the correlation.24 ,26 Our sample indeed showed a smaller range of BR in the left putamen (1.55) compared with the right putamen (1.92). In this study, another source of variability may stem from the fact that some patients were on dopamine replacement therapy during the UPDRS-III assessment, which probably led to an underestimation of their motor impairments. Dopaminergic medication, however, does not influence [123I]FP-CIT binding.18
Dopamine has a modulatory role in the communication within cortico-striatal-thalamocortical circuits. Our results on reduced DaT availability in the caudate nucleus suggest involvement of dysfunctional associative and limbic cortico-striatal-thalamocortical circuits in the pathophysiology of depression in PD. Imaging studies have consistently shown dysfunction of these circuits in non-PD-related depression,27–29 whereas studies focusing on cortico-striatal-thalamocortical functioning related to depression in PD are limited. One study showed decreased regional glucose metabolism in the caudate nucleus and inferior frontal cortex in depressed PD patients compared with non-depressed PD patients.30 Both are involved in the limbic cortico-striatal-thalamocortical circuit. Further support for dysfunction of this circuit in PD-related depression comes from studies that showed a correlation between the severity of depressive symptoms in PD and reduced orbitofrontal cortex volume31 and loss of white matter tracts in the right inferior orbitofrontal region.32
Although our design is correlational, which limits our ability to draw conclusions on cause and effect, the results suggest that loss of dopaminergic input to the caudate nucleus may be a contributing factor in the development of depressive symptoms in PD. The ventral tegmental area (VTA) innervates the ventral striatum, which includes a large part of the caudate nucleus.33 The putamen is innervated by dopaminergic projections from the substantia nigra, which, in comparison with the projections from the VTA, are generally more severely affected by the PD pathology.4 Because depressive symptoms correlated negatively with DaT binding in the caudate nucleus, we speculate that depression in PD might be specifically associated with degeneration of dopamine neurons in the VTA. This claim is supported by studies in animal models that showed a link between decreased or abnormal activity of VTA dopamine neurons and depression.34 ,35 Moreover, successful treatment with antidepressants led to normalised neural activity of the VTA.35 ,36 Since it is impossible to differentiate between dopaminergic projections from the substantia nigra and VTA using [123I]FP-CIT SPECT, this claim needs to be substantiated by further studies. Such studies should also investigate the interaction of dopamine with the noradrenergic and serotonergic system, which are also affected in PD-related depression.7 ,11 ,12
A possible limitation of this study is that the assessment of depressive symptoms was based on a self-report questionnaire (BDI). We therefore had no validated clinical diagnosis by an experienced psychiatrist. Nonetheless, the BDI has excellent psychometric properties and has been validated for use in PD patients.37
In summary, our results support a differential role of anatomically segregated cortical-striatal-thalamocortical circuits in motor and depressive symptoms in PD. The current results suggest that depressive symptoms in PD relate to degeneration of dopaminergic projections and possibly those specifically from the VTA. This finding is in accordance with the clinical experience that depression in untreated PD often disappears after the start of dopamine replacement therapy38 ,39 and suggests that optimising dopamine replacement therapy in PD deserves consideration as a first step in the treatment of depression.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online supplement
Footnotes
-
Contributors CV: analysis and interpretation of the data, writing and literature search. PR: data collection, analysis and interpretation of the data and revising manuscript. DJV: data analysis and interpretation, revising manuscript and intellectual contributions. KDvD: data collection and management, and revising manuscript. YDvdW: study design and revising manuscript. EMJF: patient recruitment, study design and revising manuscript. JHS: revising manuscript and intellectual contributions. HWB: patient recruitment, study design, revising manuscript and supervision. OAvdH: study design, analysis and interpretation of the data, study supervision, writing and guarantor.
-
Competing interests None.
-
Ethics approval VU University Medical Center Medical Ethics Committee.
-
Provenance and peer review Not commissioned; externally peer reviewed.