Article Text

Abstract
Background The prognosis of functional (or psychogenic) motor symptoms (weakness and movement disorder) has not been systematically reviewed.
Methods We systematically reviewed PubMed for all studies of eight or more patients with functional motor symptoms reporting follow-up data longer than 6 months (excluding studies reporting specific treatments). We recorded symptom duration, physical and psychiatric comorbidity, disability, occupational functioning at follow-up and prognostic factors.
Results 24 studies were included. There was heterogeneity regarding study size (number of patients (n)=10 491), follow-up duration clinical setting and data availability. Most studies (n=15) were retrospective. Reported symptom outcome was highly variable. Mean weighted follow-up duration was 7.4 years (in 13 studies where data was extractable). The mean percentage of patients same or worse at follow-up for all studies was 39%, range 10% to 90%, n=1134. Levels of physical disability and psychological comorbidity at follow-up were high. Short duration of symptoms, early diagnosis and high satisfaction with care predicted positive outcome in two studies. Gender had no effect. Delayed diagnosis and personality disorder were negatively correlated with outcome. Prognostic factors that varied between studies included age, comorbid anxiety and depression, IQ, educational status, marital status and pending litigation.
Conclusions Existing follow-up studies of functional motor symptoms give us some insights regarding outcome and prognostic factors but are limited by their largely retrospective and selective nature. Overall, prognosis appears unfavourable. The severity and chronicity of functional motor symptoms argues for larger prospective studies including multiple prognostic factors at baseline in order to better understand their natural history.
- NEUROPSYCHIATRY
- SYSTEMATIC REVIEWS
- MOVEMENT DISORDERS
- HYSTERIA
- SOMATISATION DISORDER
Statistics from Altmetric.com
Introduction
Functional (or psychogenic) motor symptoms refer to weakness or movement disorders that are genuine but do not relate to an underlying neurological disease.1 ,2 Alternative names for this group of symptoms include motor conversion disorder/symptoms (diagnostic and statistical manual of mental disorders, fourth version (DSM IV)) and dissociative motor disorder (ICD-10). Functional motor symptoms, as we will call them in this review, are the second commonest ‘non-organic’ symptom seen in neurological practice after non-epileptic attacks,3 ,4 with paralysis or weakness being the commonest manifestation.3
The perception of the prognosis of functional motor symptoms in the medical literature is variable. Historically, patients with acute functional motor symptoms have often been thought to have a good outcome. However, neurologists working in specialist clinics frequently encounter patients with disabling and chronic functional motor symptoms that appear resistant to treatment.
We aimed to systematically review all follow-up studies of functional motor symptoms. We focused on global clinical outcome as well as physical and occupational functioning. We also collated data regarding negative and positive prognostic factors including comorbidity and socio-economic status.
The issue of diagnostic revision and misdiagnosis at follow-up was not included in this review since we have systematically reviewed this topic previously.5
Methods
A broad search strategy was used, using PubMed, the reference lists of articles we found in this search and reference lists of important overview articles, as well as articles known by JS, MJE and AC.
We searched for all studies reporting on functional motor symptoms, using these terms: “conversion disorder, conversion symptoms, hysteri*, somatisation, psychogenic, psychosomatic, non-organic, unexplained, dissoc*” and first “weakness, paralysis, movement disorder, gait disorder, motor symptoms, dystonia, myoclon*, tremor, twitching, wheelchair, *plegia, *paresis, disability, *” and second “prognosis”, “follow-up”, “natural history” and “natural course”. Relevant studies were identified and their reference lists were hand searched.
Inclusion and exclusion criteria are listed in table 1. We attempted to find all the literatures from 1 January 1940 up to and including 1 January 2013.
Criteria for study inclusion and exclusion
We extracted information on: number, age and gender of participants; follow-up duration and proportion followed up; study design; symptom duration and type; prognostic factors: physical and psychiatric comorbidity, disability and occupational functioning at follow-up. We planned an analysis with a general composite of outcome and of outcome per symptom. We planned graphical analyses of prognosis by duration of follow-up, duration of symptoms at initial presentation, type of motor symptom, age and proportion of patients followed up in each study. Prognostic factors were divided into: ‘positive’, ‘negative’ and ‘no influence’ for the purpose of description and analysis.
Results
The initial search strategy yielded 5874 articles. After deduplication and review of titles and references, 102 studies were selected for the review as potentially eligible, 78 studies were excluded. Finally, 24 articles were included. Table 2 summarises all included articles and the outcome reported. Six of the excluded articles had useful information about prognosis and are also described separately below but were not included in the main analysis.6–11
Study characteristics and outcome
Included studies (24 studies, n=2069)
There was considerable heterogeneity between studies with studies ranging in size (n=8–517), duration of follow-up (0.5–19 years), completeness of follow-up (14–100%), type of motor symptom, symptom outcome (ranging from 10 to 90% better or completely recovered at follow-up) and data availability of the studies. Most studies (n=15) were retrospective. There were two pairs of studies of dystonia12 ,13 and tremor14 ,15 in which the population studied overlapped. The study of Carter16 was considered as two separate prognostic studies of paralysis and tremor. There was one case–control study, which was prospective,13 but there were no prognostic studies in which control data were used to determine prognostic factors.
Outcome
Typically, the outcome for patients with functional motor symptoms was unfavourable. In four out of 22 studies (not including two overlapping studies),12 ,14 66% to 100% of patients had the same or worse symptoms at follow-up (n=135).13 ,17–19 In further 14 studies, 33% to 66% of patients’ symptoms were the same or worse at follow-up (n=533),15 ,16 ,20–31 and in only five studies, 33% or less of patients had symptoms same or worse at follow-up (n=464).16 ,32–35 Table 3 shows the percentages of symptoms that were same or worse, or improved or remitted at follow-up, weighted according to the numbers of patients in follow-up, in the above-mentioned categories.
Percentages of symptoms that were same/worse or improved/remitted at follow-up, weighted according to the number of patients in follow-up and categorised by symptoms same/worse per study
The mean weighted duration of follow-up in years was 7.4 years (in 13 studies where mean years of follow-up data were extractable). Carrying out an analysis of the total 23 studies weighted according to the numbers of patients at follow-up but not heterogeneity and duration of follow-up, the mean percentage with the same or worse outcome overall was 40% (n=1134) with outcome for each symptom being dystonia 69% (n=77), tremor 66% (n=67), Mixed Movement Disorders 44% (n=291), Weakness 41% (n=129), Mixed Motor 29% (n=556). The total percentage of patients whose symptoms completely remitted was 21.5%, excluding five studies that did not mention numbers of total remission.19 ,22 ,28 ,29 ,35
Physical and occupational functioning
Generally, high levels of dependency, disability and work absence were found at follow-up. A range of 17% to 65% of patients were at work at follow-up (n=734).15 ,18–20 ,23 ,27 ,32 ,34 ,35
Comorbidity
High frequencies of comorbid functional (psychogenic) symptoms were seen at baseline and follow-up. None of the studies reported data comparing these comorbidities at follow-up and baseline. In four studies (n=188),13 ,17 ,19 ,22 30% to 60% of patients and in another three studies (n=216) 60% to 90% of patients had one or more other functional neurological symptom.14 ,20 ,28 Often more than one symptom at a time was reported, especially pain in multiple sites (eg, back, head, limbs), sensory symptoms, as well as many others such as bladder or bowel symptoms, fatigue, nausea, diarrhoea, sleep problems, dizziness, non-epileptic seizures, memory problems, visual disturbance, speech problems, black outs, dysphonia and hearing problems. A supplementary study36 to the included study by Crimlisk et al20 highlighted frequent re-referrals to neurology and other medical specialties during the follow-up period.
Psychiatric comorbidity was also seen frequently. Mostly anxiety and depression were reported, anxiety in 17% to 42% of patients in five studies (n=266),2 ,13 ,25 ,27 ,32 depression (or affective disorder) 19% to 71% in six studies (n=349).13–15 ,19 ,27 ,32 Dissociative symptoms and personality disorder were also commented on.13 ,25 ,32
Additional neurological disease comorbidity at presentation was reported in Feinstein et al27 in 12% (not further specified), in Kim et al17 17%, of which mainly organic tremor, and furthermore dystonia, dyskinesia and Parkinson's disease, each in one patient and in Crimlisk et al.20
Analysis of improvement by study duration, % follow-up and symptom
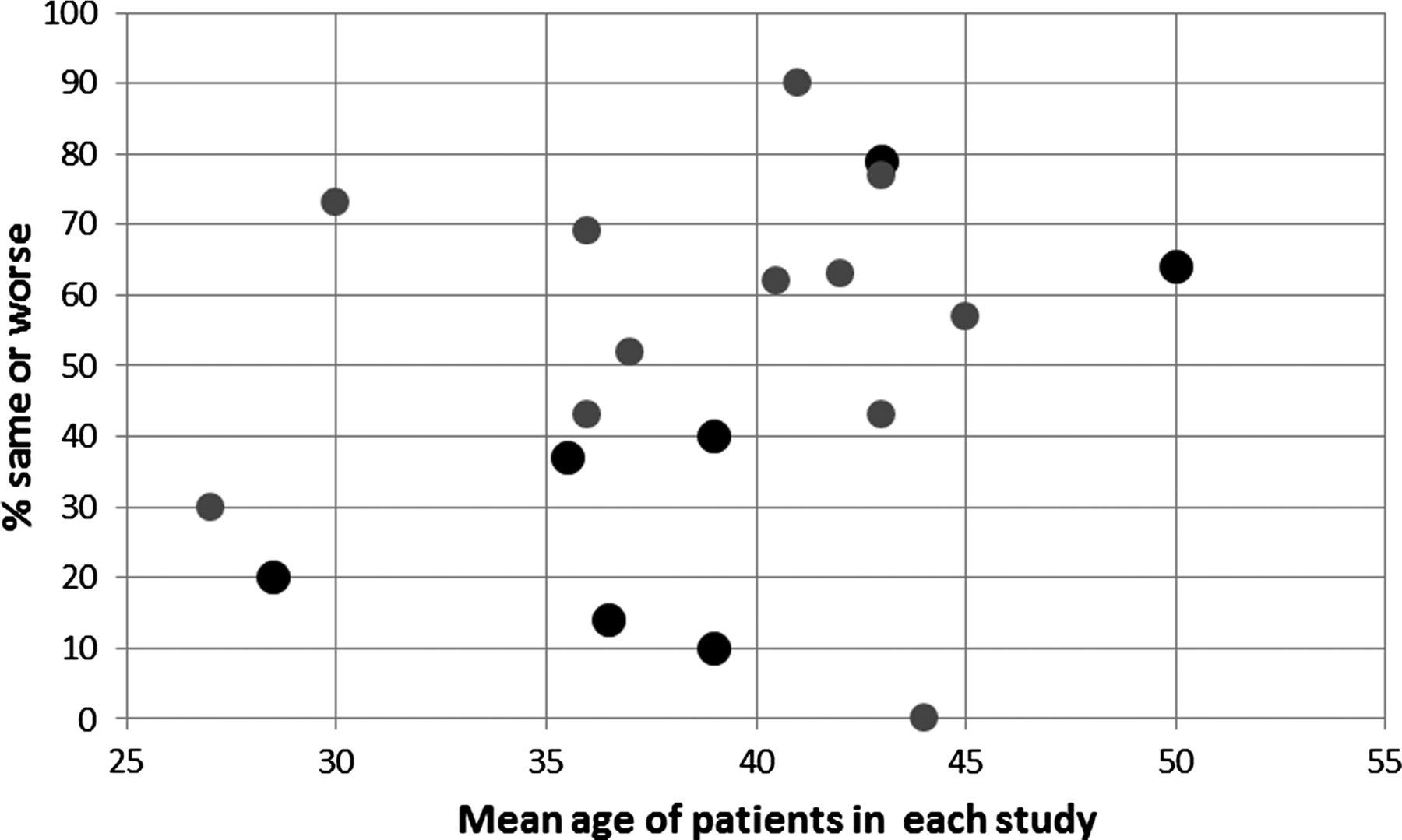
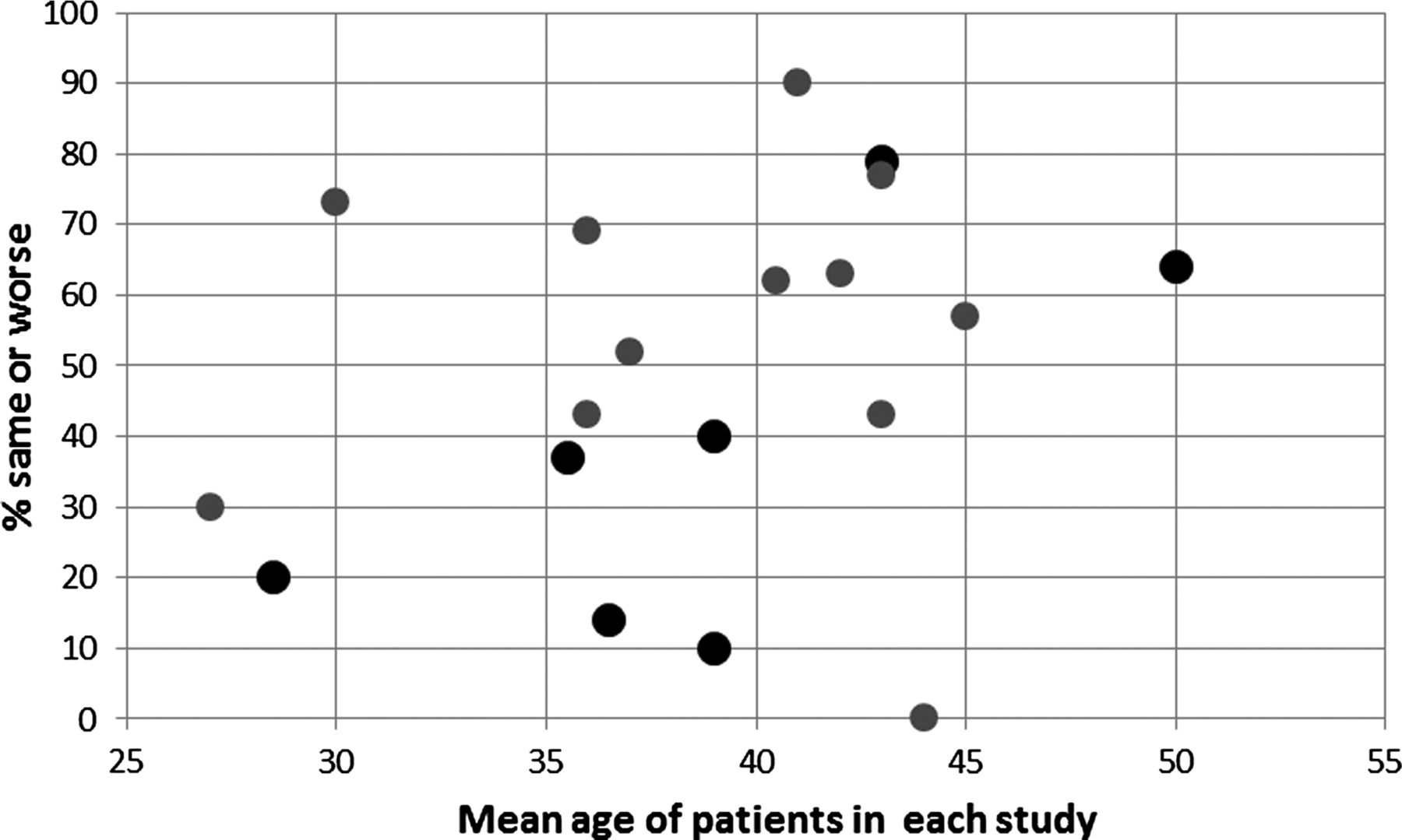
Figure 1 shows symptom outcome plotted against duration of follow-up. There was no obvious relation between follow-up duration and outcome, nor, perhaps surprisingly between symptom type and symptom outcome. Figure 2 shows symptom outcome plotted against the follow-up rate of individual studies. There was possibly a slight trend indicating that a higher follow-up rate might be correlated with a better mean outcome, but a wide spread, different study size and other confounding factors prevent any firm conclusions. Figure 3 shows symptom outcome plotted against mean age of patients in the study with no clear trend seen. We also carried out an analysis of outcome relative to symptom duration prior to recruitment to the study. There were only 11 studies with extractable data. No clear trend emerged from this analysis (see online supplementary file 1).

Proportion ‘same or worse symptoms’ at follow-up relative to mean follow-up duration in years in all included studies, also showing symptom. Tremor, Dystonia (functional dystonia and fixed dystonia), Mixed movement disorders (more than one type of movement disorder), Weakness (paralysis), Mixed weakness and movement disorders (mixture of movement disorder and weakness/paralysis). Two studies did not record follow-up duration.18 ,24

Proportion ‘same or worse symptoms’ at follow-up relative to follow-up rate in 23 included studies. One study did not record percentage follow-up.29
{kind=link}
{kind=link}
{kind=link}
Proportion ‘same or worse symptoms’ at follow-up relative to mean age in 19 included studies. Studies that reported age at onset of symptoms are depicted with a slightly bigger black circle; studies that reported age at baseline of the study are depicted with a grey circle. Studies that did not record mean age,29or whether age was recorded at baseline or follow-up,16 ,21 ,28 are not shown.
Outcome by type of motor symptom
Prognosis varied between different functional motor symptoms. Studies of functional tremor showed relatively high proportions of patients same or worse at follow-up (44–90%) (n=191).14 ,16 ,17 ,22 ,23 Functional/psychogenic dystonia had an even worse prognosis. In the overlapping studies of Schrag et al13 and Ibrahim et al12 (n=103) with a mean of 4.9 years and 7.6 years of follow-up 73% to 78% of patients had the same or worse symptoms. The outcome of weakness/paralysis was more variable, ranging from 4% to 69% of patients with same or worse symptoms at follow-up (n=25–60).16 ,19 ,28 ,33 ,34 The most optimistic study in this group was a 1949 study in which patients were treated actively with hypnosis, thiopental suggestion and psychotherapy.16 The 1957 study of Ljungberg (n=381) still represents one of the best prospective studies and contained a comparison of outcome between symptoms.35 In this study, patients with gait disorder fared better at 5 years (10% symptomatic) compared to patients with weakness (32% symptomatic) and tremor (51%). Two studies looked at influence of symptom type on outcome within their sample and found no correlation.27 ,32
Prognostic factors
Factors correlated with outcome and therefore thought to influence prognosis were investigated in many studies. Table 4 shows these factors.
Prognostic factors (positive, negative or no effect) in studies of functional motor symptoms
Age
Four studies (n=211) found that younger age predicted a better outcome,15 ,19 ,23 ,29 but seven studies (n=248) found age was not a significant prognostic factor.12 ,20 ,27 ,30 ,32 ,34 ,35
Gender
None of the studies that looked at the influence of gender on outcome found an effect (n=676).12 ,15 ,19 ,20 ,32 ,34 ,35
Duration of symptoms prior to diagnosis
A shorter duration of symptoms prior to diagnosis was shown to predict a better outcome in nine studies (n=451).15 ,20––22 ,25 ,27––30 There were no studies which did not find a relationship between duration of symptoms prior to diagnosis and outcome, suggesting this as one of the most consistent findings of this review.
Psychiatric comorbidity
The presence of psychiatric comorbidities was correlated with outcome in eight studies.12 ,14 ,15 ,20 ,27 ,29 ,34 ,35 Six found a negative effect on outcome (n=633).12 ,14 ,27 ,29 ,34 ,35 Ibrahim et al12 found a high Hospital Anxiety and Depression Scale (HADS) score was correlated with bad outcome, Mace and Trimble29 found anxiety had a worse effect than depression, Feinstein et al27 found the severity of psychiatric comorbidity influenced outcome. Jankovic et al14 reported that any psychological, psychogenic or somatic comorbidity predicted negative outcome. Binzer et al,34 however, did not find any correlation between an axis I diagnosis and outcome. Personality disorder was negatively correlated with outcome in three studies (n=442).29 ,34 ,35 Two studies reported a positive effect of the presence of an affective or anxiety disorder on outcome.15 ,20 The authors of these studies suggested that functional symptoms improved synergistically with these emotional disorders.
Education, IQ, social class, marital status and litigation
Several studies found educational status (n=93),27 ,32 ,34 IQ (n=381)35 and social class (n=64)20 and had no prognostic effect. The effect of marital status was investigated in two studies (n=106), one showing no effect,27 while the other found that change in marital status (either marriage or separation) was positively correlated with outcome.20 Two overlapping studies reported on the effect of perception of the patient's social life, one found it beneficial (n=122,15 the other found no effect (n=127).14 Pending litigation correlated with negative outcome in one study (n=64), 20 while three (partially overlapping) studies (n=164) did not find a correlation.14 ,15 ,27 No other studies reported on litigation.
Treatments given as part of the study
In many of the studies included in this review, some treatment was given in part of the population.13––18 ,21 ,25 ,32 Treatment interventions were very heterogeneous, ranging from antidepressants and levodopa to hypnosis, suggestion and psychological treatment. Results were usually only partially helpful in some of the patients or gave temporary relief. Crude analysis of the weighted percentage of same or worse symptoms at follow-up according to the number of patients at follow-up in these studies was 49%. All other (non-treatment) studies had a weighted percentage of same or worse symptoms at follow-up according to the number of patients at follow-up of 39%. We did not find a relation between better outcome and treatment interventions.
Additional excluded studies
Six studies described some form of follow-up on cohorts of patients with functional motor symptoms but did not meet inclusion criteria for our main review, primarily because the follow-up duration was too short or not stated (see online supplementary table S1).6––11 In three studies (total n=74), inpatients in spinal rehabilitation units with functional paralysis were reported with data at discharge.7 ,9 ,11 The outcome was 100% recovery in two of these studies9 ,11 and 55% in another.7 In some follow-up studies of functional movement disorder, that outcome was more variable although duration was unknown.6 ,8 ,10
Discussion
Outcome
Overall, the prognosis of functional motor symptoms appears unfavourable. In a large majority of studies (20 out of 24 studies), more than one-third of patients had the same or worse symptoms at follow-up. In cases where symptoms improved, they tended not to resolve completely.
The outcome of motor symptoms appears comparable to a recent review of the prognosis non-epileptic attacks, which found in a majority of studies that 60% or more patients were still having attacks at follow-up,37 and to a study of a more general group of 761 patients with symptoms unexplained by disease attending neurology clinics (Scottish Neurological Symptom Study, SNSS) where poor outcome was reported by 67%.38
High rates of physical and psychological comorbidity at baseline in these studies highlight the importance of not simply considering functional motor symptoms in isolation. They are typically only one of multiple somatic and psychological symptoms.2 In most studies, levels of physical disability were high, and working status and quality of life impaired. Studies examining comparator groups of disease controls have found comparable levels of disability and quality of life between patients with functional movement disorders and Parkinson's disease,39 and between functional paralysis and multiple sclerosis.19 SNSS found that patients with symptoms unexplained by disease had comparable rates of physical disability and higher rates of psychological disability to patients with defined neurological disease.40
Movement disorders, like fixed dystonia and tremor, seem to have a worse outcome than weakness and paralysis. Because of the low number of studies and the multiple confounding factors varying between studies, it is difficult even to draw this conclusion. In particular, studies of patients with movement disorders are often drawn from specialist movement disorder clinics where severity may be worse, in comparison with studies of patients with weakness which have more commonly been drawn from a general neurology setting.
Prognostic factors
We found heterogeneity in many prognostic factors reported. Probably the strongest factor to emerge was a short duration of symptoms as a good prognostic factor. Even here, clinical experience indicates that a long duration of symptoms does not always preclude a good recovery and similarly patients with short duration of symptoms do not always recover.
The influence of age was surprisingly ambiguous, and there was no clear effect from gender or even comorbid emotional disorder. We did not include paediatric studies which generally do report better outcomes.37 ,41––44
Socio-economic factors, such as a change in marital status may be a good prognostic factor, but there was surprisingly no effect with litigation, although only four studies looked at this. In contrast, the receipt of health-related financial benefits was a strong independent predictor of poor outcome in the SNSS.38
A limited amount of data support the idea that a good explanation of the diagnosis and patient confidence in the physician correlates with a good outcome for functional motor symptoms. Studies in functional motor symptoms are limited by the retrospective nature of the way in which this question was asked.14 ,15 SNSS found that beliefs about illness were of key importance in predicting outcome, more so than disability, symptom count and emotional distress which all disappeared from a multifactorial model.38 A review of prognostic factors in non-epileptic attacks did not find that understanding of the disorder makes a difference in outcome, but suggested that acceptance does: patients who showed relief that their diagnosis was not epilepsy had improved seizure frequency, whereas those who reacted with anger or confusion had a poorer outcome.37
Limitations
The studies that matched our criteria were mostly retrospective, small and largely did not fulfil basic aspects of a proper follow-up study, with baseline measurement of prognostic factors or outcome of specific symptoms and proper follow-up rates. The data should therefore be interpreted with care. There is likely to be considerable heterogeneity between, for example, patients with short duration of symptoms attending a local service 34 and patients with fixed dystonia attending a tertiary centre.12 The minimum follow-up duration of 6 months is relatively arbitrary. Patients who present acutely and remit in a few days will be missed. However, it is important to know whether these patients relapse in the ensuing months, and therefore, a minimum follow-up duration seems necessary.
In addition follow-up rates were variable, patients with better outcomes may be more likely to be lost to follow-up. There were no treatment intervention studies in the review (those studies were excluded), but during the follow-up period, some of the studies described treatments. We found that the outcome of these studies was comparable to studies where treatment was not mentioned (crude weighted mean 49% vs 39% same or worse). It seems likely that even where treatment was not mentioned that many would have received some form of it so it remains hard to know what the ‘untreated’ natural history of functional motor symptoms might be. Our review was also limited in its scope to adult studies. There was a risk that by including paediatric studies, the data would not have been generalisable, since most neurologists are either adult or paediatric neurologists. The review was also limited by selecting only English Language Studies.
Conclusion
Follow-up studies of functional motor symptoms give us some insights regarding outcome and prognostic factors but are limited by their largely retrospective and selective nature. Overall, the prognosis appears unfavourable. Based on the limited data available, there is a suggestion that a short duration, early diagnosis and an acceptable explanation would be valuable in clinical practice.
The severity and chronicity of functional motor symptoms argues for the importance of larger prospective studies including multiple prognostic factors and comorbidity at baseline in order to better understand their natural history.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online figure
- Data supplement 2 - Online table
Footnotes
-
Contributors JG: substantial contributions to conception and design, acquisition of data, analysis and interpretation, wrote the first and last draft of the article. JS: substantial contributions to conception and design, acquisition of data, analysis and interpretation, critically revising, finally approved the version to be published. ME: substantial contribution to design, to interpretation of data, critically revised the manuscript, finally approved the version to be published. AC: substantial contribution to the concept and design, to interpretation of data, critically revised the manuscript, finally approved the version to be published.
-
Competing interests None.
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
Data sharing statement All data, abstracted from the included studies in this systematic review, are available to anyone being interested in receiving them.