Article Text

Abstract
Objective The early detection of MRI findings suggestive of immune reconstitution inflammatory syndrome (IRIS) in natalizumab-associated progressive multifocal leukoencephalopathy (PML) is of crucial clinical relevance in terms of treatment decision-making and clinical outcome. The aim of this study was to investigate the earliest imaging characteristics of PML-IRIS manifestation in natalizumab-treated patients with multiple sclerosis and describe an imaging pattern that might aid in the early and specific diagnosis.
Methods This was a retrospective study assessing brain MRI of 26 patients with natalizumab-associated PML presenting with lesions suggestive of PML-IRIS during follow-up. MRI findings were evaluated considering the imaging findings such as mass effect, swelling, contrast enhancement, new perivascular T2 lesions and signs suggestive of meningeal inflammation.
Results Contrast enhancement was the most common imaging sign suggestive of PML-IRIS, seen in 92.3% of the patients (with patchy and/or punctuate pattern in 70.8% and 45.8% respectively), followed by new T2 lesions with a perivascular distribution pattern (34.6%). In those patients with contrast enhancement, the enhancement was present in the lesion periphery in 95.8% of the patients. Contrast-enhancing lesions with a perivascular distribution pattern outside of the PML lesion were observed in 33.3% of the patients. The most common overall pattern was contrast enhancement in the border of the PML lesion with either a patchy or punctuate appearance in 88.5% of all patients.
Conclusions Contrast enhancement is the most common earliest sign of natalizumab-associated PML-IRIS with a frequent imaging pattern of contrast-enhancing lesions with either a patchy or punctuate appearance in the border of the PML lesion.
Statistics from Altmetric.com
Introduction
Progressive multifocal leukoencephalopathy (PML) is a rare opportunistic infection of the central nervous system (CNS) in immunocompromised patients caused by reactivation and replication of JC virus (JCV) leading to a lytic infection of astrocytes, oligodendrocytes and neurons.1–3 Natalizumab (Biogen Inc, Cambridge, Massachusetts, USA), a humanised monoclonal antibody against the α4-integrin adhesion molecule affecting the ability of immune cells to attach and to pass through the blood–brain barrier, is approved for the treatment of relapsing multiple sclerosis (MS).4 ,5 PML is a well-known adverse event in natalizumab-treated patients and as of 3 March 2015, 538 confirmed PML cases in natalizumab-treated patients with MS have been reported.6 ,7
On the basis of the JCV serostatus, treatment duration and immunosuppressant therapies prior to the initiation of natalizumab treatment, patients with MS can be classified according to their risk of developing PML.8 ,9 This has led to the concept of strict pharmacovigilance, in particular for those patients who have a high risk of developing PML.10 MRI of the brain plays a crucial role in natalizumab pharmacovigilance since it has been conclusively shown that MRI can detect PML in very early stages even while the patient does not show any clinical symptoms suggestive of PML (asymptomatic PML).11 ,12 In addition, the detection of natalizumab-associated PML in an asymptomatic stage is associated with a better functional outcome compared with the diagnosis of PML at a symptomatic stage.11–15
Brain MRI plays an important role in the diagnosis of PML, monitoring of the lesions evolution and in the detection of imaging findings suggestive of immune reconstitution inflammatory syndrome (IRIS).16 ,17 IRIS is defined as an inflammatory immune response against causative pathogens or non-infectious antigens during or after partial and full recovery of the immune system in previously immunocompromised patients.18 ,19 In natalizumab-treated patients with MS diagnosed with PML, plasma exchange (PLEX) or immunoadsorption (IA) are frequently used to accelerate the clearance of natalizumab, thus restoring the immune system and leading to lymphocytes trafficking into the brain. This stage is characterised by a simultaneous presence of PML and inflammatory lesions (PML-IRIS) presenting with certain clinical, imaging and histopathology findings.16 ,18–21 Clinically, PML-IRIS is characterised by new clinical symptoms and/or worsening of existing clinical symptoms associated with progressive imaging findings of active inflammation. Recent reports have conclusively demonstrated that frequent imaging characteristics of later PML-IRIS stages are contrast enhancement, rapid progression of existing PML lesions showing mass effect with swelling and oedema.6 ,16 ,17 ,20–25
Although conclusive data is lacking so far, it has been hypothesised that an early and specific diagnosis of PML-IRIS using MRI has crucial clinical relevance since an early treatment intervention (eg, steroid treatment) might be associated with a more favourable outcome. A false-positive PML-IRIS diagnosis resulting in the use of steroids at a premature stage may lead to a PML re-activation and progression with probably negative clinical consequences.26–28 Most of the data on natalizumab-associated PML-IRIS imaging findings are based on symptomatic and later PML-IRIS stages.6 ,16 ,21–24 Therefore, there is an urgent need for advancing knowledge in early PML-IRIS detection on brain MRI. However, the imaging characteristics of early PML-IRIS in natalizumab-treated patients with MS have not been investigated so far.
The aim of our study was to investigate the imaging characteristics of early PML-IRIS in natalizumab-associated PML and to describe an imaging pattern, which might aid the early diagnosis and up-front treatment intervention of PML-IRIS.
Patients and methods
Standard protocol approvals, registrations, and patient consents
Brain MRI is included to the standard patient care for natalizumab-treated patients with MS with respect to treatment efficacy and safety monitoring. Prior to this study, we obtained a waiver from our local institutional review board (IRB) stating that the requirements of the Medical Research Involving Human Subjects Act (WMO) did not apply and that official IRB approval was not mandatory. Written informed consent was obtained from all participants for the use of the clinical and imaging data for research and teaching purposes.
Study design and patient selection
This was a retrospective study using brain MRIs for the diagnosis and follow-up of PML lesions in natalizumab-treated patients with MS. Sixty-one patients with natalizumab-associated PML obtained from two previously described data sets (17 patients form the Dutch natalizumab-associated PML cohort and 44 patients referred by other institutions to our centre for second opinion and research purposes, figure 1)13 were screened for any imaging signs suggestive of PML-IRIS after the discontinuation of natalizumab treatment and the reconstitution of the immune system by natural natalizumab washout or natalizumab removal by PLEX/IA. We defined imaging findings suggestive of PML-IRIS according to PML-IRIS imaging findings with histopathology confirmation as previously described in the literature.20 ,21 This included the first manifestation of any new lesion(s) with inflammatory characteristics (one of the following imaging signs: contrast enhancement, new T2 lesions with a perivascular distribution pattern, oedema, mass effect) occurring after the reconstitution of the immune system either after natalizumab discontinuation and natural washout or after PLEX/IA. In a second step, imaging signs suggestive of PML-IRIS were verified by reviewing follow-up brain MRIs. We defined the following inclusion criteria: (1) symptomatic or asymptomatic natalizumab-associated PML diagnosed according to the American Academy of Neurology (AAN) PML diagnostic criteria as definite, probable or possible PML.29 (2) Availability of brain MRI at the time of diagnosis and during follow-up including the stage of PML-IRIS and post-PML-IRIS stage. (3) A multisequence brain MRI protocol including T2 and/or fluid-attenuated inversion recovery (FLAIR) and postcontrast T1-weighted sequences. (4) Imaging materials collected in the Digital Imaging and Communication in Medicine (DICOM 3) file format. Exclusion criteria were defined as: (1) any sign of inflammation on brain MRI including contrast-enhancing PML lesions suggestive of ‘inflammatory PML’ at the time of (suspected) PML diagnosis because the underlying pathogenesis and evolution of these inflammatory findings suggestive of ‘inflammatory PML’ (eg, overlap and/or interaction with PML-IRIS lesions) are not well understood. (2) Bad image quality not suited for diagnostics purposes (ie, movement artefacts, bad repositioning, etc).

Flowchart presenting the patient selection and the decision-making according to the inclusion and exclusion criteria (IRIS, immune reconstitution inflammatory syndrome; PML, progressive multifocal leukoencephalopathy).
Image analysis and interpretation
All MRIs were analysed on a digital workstation by two raters in consensus (MPW and MTW) with special expertise in the field on inflammatory diseases of the CNS. The first follow-up MRI scan, showing imaging characteristics suggestive of PML-IRIS according to previously published PML-IRIS characteristics20 ,21 were analysed and categorised: (1) occurrence of contrast enhancement in the brain. (2) Occurrence of new and persistent lesions showing new signs of mass effect and/or oedema. (3) Occurrence of new T2 lesions with a perivascular distribution pattern. The characteristics of contrast enhancement was further classified according to the localisation (in the centre of the PML lesions, in the border of the PML lesions, outside of the PML lesions with a perivascular spread, or outside of the PML lesion without a perivascular spread) and the enhancement pattern (punctuate, homogeneous, patchy). Finally, the images were further evaluated to identify the presence of any signs of meningeal inflammation.
MRI protocols
Since the PML cases were collected from different centres, the image acquisition parameters including pulse sequences, head coils and magnetic field strengths (1.5 T and 3 T) and parameters related to spatial resolution were heterogeneous and based on local MRI protocols. In all patients the MRI protocol during follow-up, including the PML-IRIS scan, consisted of T2-weighted/proton density-weighted, FLAIR, and postcontrast T1-weighted MRIs. In 17 patients, precontrast T1-weighted images were also available during follow-up.
Statistical analysis
Descriptive statistics was used to describe the different imaging characteristics of PML-IRIS. Categorical data were summarised as frequencies and percentages, continuous data as median and range.
Results
Patients
Among the screened 61 patients with natalizumab-associated PML, 26 patients met the inclusion criteria and were included in this study (figure 1). The demographic and clinical information of this patient group is given in table 1, and the information on follow-up scanning intervals is presented in table 2.
Demographic and clinical information of the study participants
Characteristics of brain MRI follow-up after PML diagnosis
Early PML-IRIS imaging findings
Imaging findings of the first presentation of PML-IRIS during follow-up after PML diagnosis are presented in table 3. Contrast enhancement was the leading imaging finding present in 24 of the 26 patients (92.3%). With respect to a pattern of early PML-IRIS, we found that contrast enhancement either patchy (n=17) and/or punctuate (n=11) in the border of the PML lesion was the most evident pattern of early PML-IRIS and were present in 23 of the 26 cases (88.5%).
Imaging characteristics of early PML-IRIS
Five patients in this group showed a combination of punctuate and patchy contrast enhancement (figures 2 and 3). In addition, 8 of the 23 cases presented with additional perivascular enhancement (7 with corresponding T2 lesions, 1 without corresponding T2 lesions) (figure 4) and 5 cases had contrast enhancement in the centre of the lesion as well. Among the 24 patients with contrast enhancement, 1 patient presented with perivascular enhancement (with corresponding perivascular T2 lesions) and without any enhancement in the border or centre of the PML lesion. Of the two patients showing no contrast enhancement, one patient had small punctuate T2 lesions with a perivascular distribution pattern in combination with subtle mass effect and signs of oedema. The other patient showed some subtle signs of mass effect only without any contrast enhancement at all. This particular patient was not treated with steroids before the occurrence of PML-IRIS lesions. These imaging findings were considered as highly suggestive of PML-IRIS most likely not due to MS disease activity as previously suggested by expert panel guidelines.17
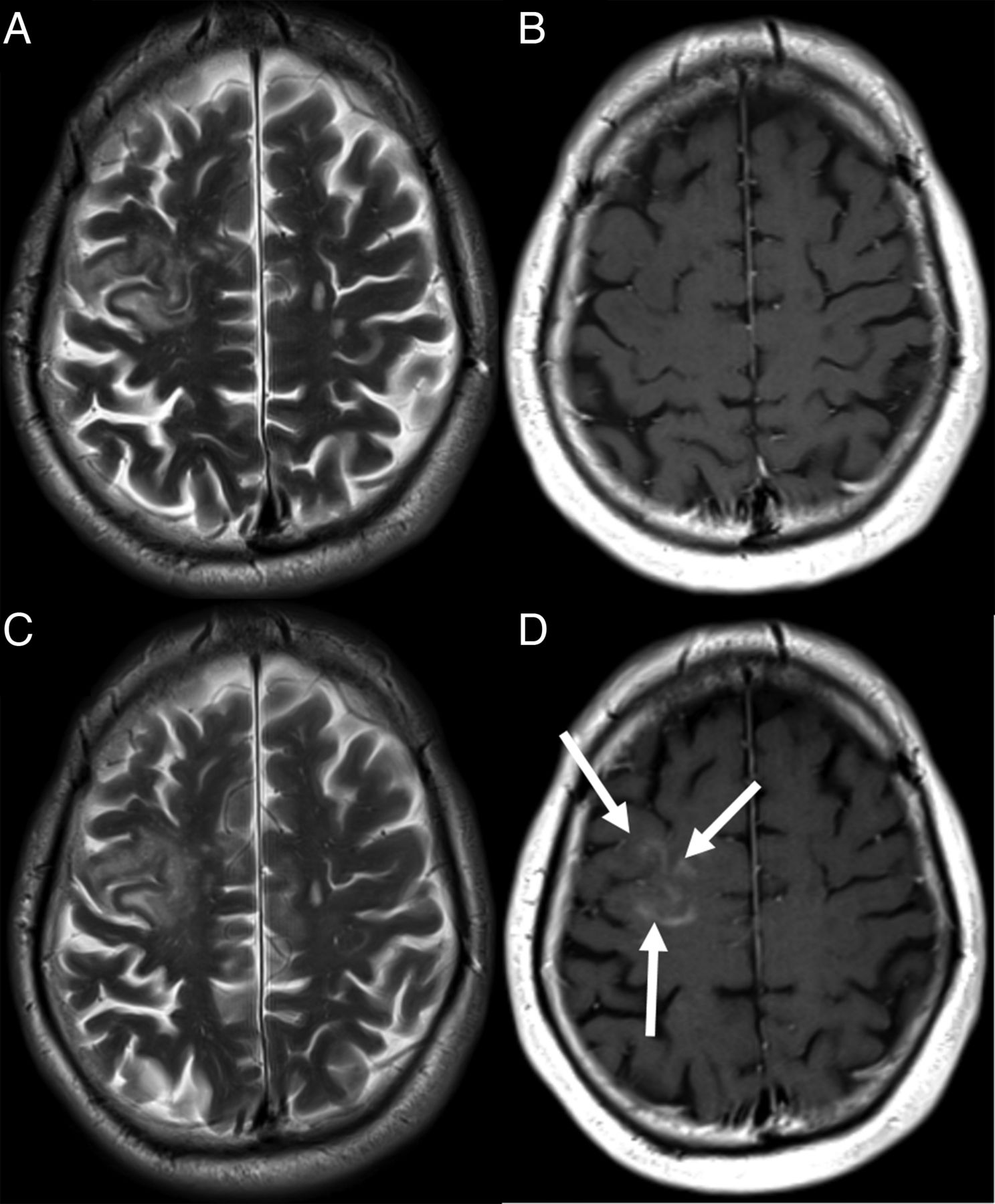
Axial T2-weighted (A and C) and contrast-enhanced T1-weighted images (B and D) of a reference MRI (A and B) and follow-up MRI (C and D) showing the first imaging signs suggestive of progressive multifocal leukoencephalopathy with immune reconstitution inflammatory syndrome (PML-IRIS). This patient showed the most frequent pattern of PML-IRIS with patchy contrast enhancement in the border in the lesion (arrows). In this patient, contrast enhancement was the only imaging sign suggestive of inflammation. This PML-IRIS lesion was not associated with any signs of swelling or oedema.

Axial fluid-attenuated inversion recovery (FLAIR) (A and C) and contrast-enhanced T1-weighted images (B and D) of a reference MRI (A and B) and follow-up MRI (C and D) showing contrast enhancement in the border of the lesion (closed head arrows). In addition, there were signs of perifocal swelling on the FLAIR image (C) with a white sulcus sign (open head arrow). In the vicinity of the progressive multifocal leukoencephalopathy lesion there are small punctuate contrast-enhancing lesions visible (D, open head arrow).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
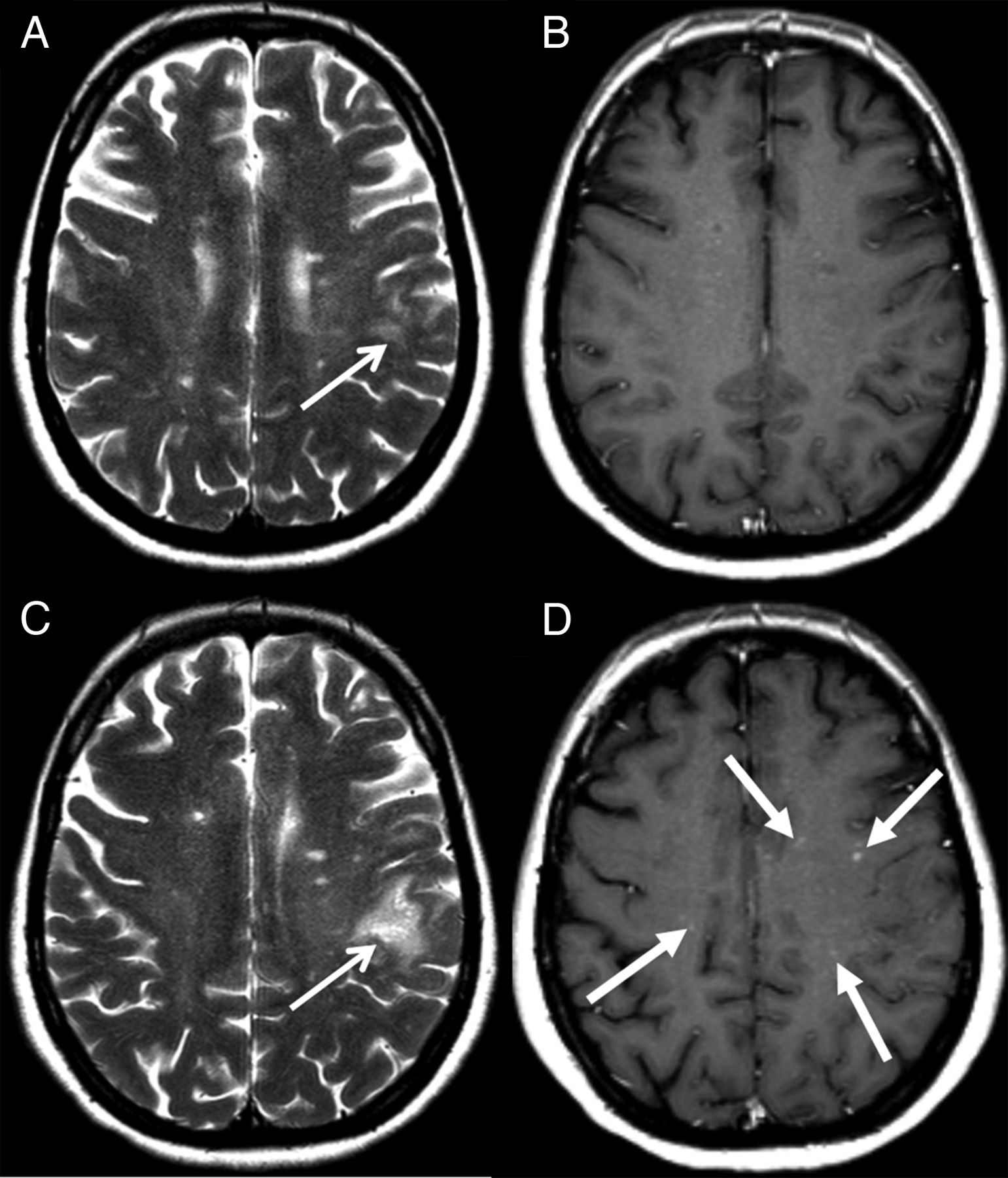
Axial T2-weighted (A and C) and contrast-enhanced T1-weighted images (B and D) of a reference MRI (A and B) and follow-up MRI (C and D) showing a substantial growth of the main progressive multifocal leukoencephalopathy (PML) lesion (A and C, open head arrow). On the follow-up scan, there are multiple small focal enhancing lesions in the deep white matter partially with a perivascular distribution pattern (D, closed head arrows). The main PML lesion itself did not show any contrast enhancement.
Discussion
In patients with natalizumab-associated PML, MRI monitoring of PML lesion evolution and detection of possible signs of inflammation suggestive of PML-IRIS is performed to guide the treating physicians in terms of treatment decision-making and patient management. The knowledge of natalizumab-associated PML-IRIS lesions is based on single case studies in later disease stages. However, the early imaging signs and characteristic MRI patterns of PML-IRIS have never been systematically investigated. In our retrospective study, we analysed brain MRI findings of patients with natalizumab-associated PML during a follow-up period and described the imaging characteristics of the first findings suggestive of inflammation. The scoring scheme we developed was based on imaging and histopathology characteristics of PML-IRIS previously described in the literature in patients with natalizumab-associated PML.6 ,16 ,22 ,23 ,30–32 Our data suggest that contrast enhancement is the most frequent imaging sign of early PML-IRIS found in 24 patients of the 26 included. Contrast enhancement with either patchy or punctuate enhancement in the border of the PML lesion was the most evident imaging pattern being present in 23 of the 26 cases (88.5%). Pathophysiologically, this can be explained by the fact that active lytic JCV infection of white matter cells is mainly present in the periphery of the PML lesion where the myelin is still relatively preserved compared with the centre of the lesion.33 It can be assumed that in these areas of relatively high viral load, the immune reaction after immune reconstitution is more prominent and imaging signs suggestive of inflammation such as contrast enhancement will be obviously present. This PML-IRIS imaging pattern with contrast enhancement in the border of the PML lesions has been confirmed in case series with subsequent histopathology verification showing severe inflammation with CD8-positive T cells and plasma cells in these areas.21 ,34
Another important aspect of inflammation in patients with natalizumab-associated PML-IRIS is the presence of small punctuate contrast-enhancing lesions outside of the main PML lesion with a perivascular distribution, present in 33.3% of the patients with contrast enhancement. These small punctuate contrast-enhancing lesions can even be the leading imaging sign of PML-IRIS. This imaging phenomenon is supported by histopathology data demonstrating an abundance of B cells as well as CD8-positive T lymphocytes outside the main PML lesions particularly in the perivascular spaces of patients with PML-IRIS.20 ,21 We did not observe any enhancement of the leptomeningeal or pachymeningeal structures suggesting that the inflammation during PML-IRIS is rather exclusively present in the brain parenchyma. In addition, it is worth stressing, that other signs of inflammation such as perilesional oedema leading to focal swelling of the brain parenchyma occur almost exclusively in combination with the presence of contrast-enhancing lesions. Subtle perilesional oedema without any contrast-enhancing lesions was only observed in one single patient.
One strength of our study is the fact that all patients had a confirmed diagnosis of PML fulfilling the diagnosis of possible, probable or definite PML according to the AAN diagnostic criteria.29 The diagnosis PML was further strongly supported by clinical and imaging follow-up examinations confirming the PML-IRIS diagnosis according to suggested PML-IRIS imaging characteristics that were based on histopathology confirmation as described in the literature.20 ,21 ,30 This is important since natalizumab discontinuation without having PML can occasionally lead to imaging findings that mimic IRIS.35 ,36 In addition, in order to create a rather homogeneous data set to allow a rather straight-forward MRI assessment of new findings suggestive of inflammation, we excluded all patients from the analysis showing signs of inflammation at the time of PML diagnosis prior to natalizumab discontinuation.14 ,37 ,38
Since there are no strict guidelines on the management and treatment of patients with natalizumab-associated PML, the data sets of PML-IRIS detection using MRI are rather heterogeneous in terms of the frequency of MRI. The lack of standardisation is one considerable limitation of this study. Further limitations include different PML treatment strategies and the administration of steroids prior to the occurrence of PML-IRIS lesions as in four of our patients. However, natalizumab-associated PML is a rare side effect and the collection of non-standardised clinical and imaging data sets from multiple centres is the only possibility to reach a substantial number of patients for research purposes.
Strictly speaking, PML-IRIS is a histopathological diagnosis and our observed imaging findings suggestive of PML-IRIS have not been verified on histopathology. However, this was an in vivo imaging study and in a clinical routine setting, the diagnosis of PML-IRIS has to be made on clinical and/or imaging findings only. Finally, we were formally not able to differentiate our PML-IRIS imaging findings from possible MS rebound disease activity.35 ,36 However, the data in the literature strongly suggest that PML-IRIS occurs first followed by reoccurrence of MS activity in later follow-up stages supporting the assumption that we detected signs of inflammation due to PML-IRIS and not due to MS disease activity.11 ,16 ,17 ,22 ,23 ,25 ,32 ,36
In conclusion, the dominant imaging sign of early natalizumab-associated PML-IRIS is contrast enhancement following a characteristic pattern with either patchy or punctuate enhancement in the border of the main PML lesion. In addition, small punctuate contrast-enhancing lesions outside of the PML lesions, partially with a perivascular distribution pattern, can be observed in a considerable number of patients. This pattern can be explained by the histopathologically confirmed observation of inflammatory cells in the perivascular spaces. We hope that this data will aid the early detection and an accurate diagnosis of natalizumab-associated PML-IRIS, which will lead to an early treatment with a more favourable clinical outcome.
Acknowledgments
The authors wish to thank all participants with PML for agreeing to the use of their MRIs and (para)clinical data for research and education purposes. In addition, they wish to thank Professor Wolfgang Brück and Dr Imke Metz (Department of Neuropathology, University Hospital Göttingen, Germany) for sharing their data and expertise on histopathology findings in natalizumab-associated PML-IRIS.
References
Footnotes
Collaborators Bob W van Oosten and Chris H Polman (VU University Medical Center, Amsterdam, The Netherlands), Dorine A Siepman and Rogier Hintzen (Erasmus MC, University Medical Center Rotterdam, The Netherlands), Jop Mostert (Rijnstate Hospital, Department of Neurology, Arnhem, The Netherlands), Wibe Moll (Maasstad Hospital, Rotterdam, The Netherlands), Alex EL van Golde (ZGT Hospital, Almelo, The Netherlands), Stephan TFM Frequin (St Antonius Hospital, Nieuwegein, The Netherlands), Paul AD Bouma (Tergooi, Blaricum, Hilversum, The Netherlands), Bénédicte Quivron (CH Jolimont, La Louvière, Belgium), Jean Braeckeveldt (Epicura, Baudour, Belgium), Erik van Munster and Jeroen van Eijk (Department of Neurology, Jeroen Bosch Ziekenhuis, ‘s-Hertogenbosch, The Netherlands), Thea Heersema (Department of Neurology, University Medical Center Groningen, Groningen, The Netherlands), Jaap de Graaf (Isala Hospital, Zwolle, The Netherlands).
Contributors MPW and MTW collected the data, analysed the data and wrote the manuscript. AV and MdV collected the data, interpreted the data and edited the manuscript. BIW performed the statistical analysis and edited the manuscript. FB, NDR, BMJU and JK interpreted the data and edited the manuscript. All the authors reviewed and agreed on the final versions of the manuscript.
Funding The MS Centre Amsterdam is funded by a program grant (14-358e) from the Stichting voor MS Research (Voorschoten, The Netherlands).
Competing interests MPW has received consultancy fees from Biogen and Roche. FB serves as a consultant for Bayer-Schering Pharma, Sanofi-Aventis, Biogen, Teva, Novartis, Roche, Synthon BV, Genzyme, and Jansen Research. JK has accepted consulting fees from Merck-Serono, TEVA, Biogen, Genzyme, and Novartis. NDR is an employee of Biogen. BMJU has received consultancy fees from Novartis, Merck Serono, Biogen, and Danone Research. The VUmc has received financial support for research activities from Bayer Schering Pharma, Biogen, GlaxoSmithKline, Merck Serono, Novartis, and Teva. Biogen reviewed and provided feedback on the manuscript to the authors.
Provenance and peer review Not commissioned; externally peer reviewed.