Article Text

Abstract
Background Respiratory failure is associated with significant morbidity and is the predominant cause of death in motor neurone disease/amyotrophic lateral sclerosis (MND/ALS). This study aimed to determine the effect of non-invasive ventilatory (NIV) support on survival and pulmonary function decline across MND/ALS phenotypes.
Methods Cohort recruited via a specialist, multidisciplinary clinic. Patients were categorised into four clinical phenotypes (ALS, flail arm, flail leg and primary lateral sclerosis) according to site of presenting symptom and the pattern of upper versus lower motor neurone involvement. NIV was initiated according to current consensus practice guidelines.
Results Between 1991 and 2011, 1198 patients diagnosed with ALS/MND were registered. 929 patients (77.5%) fulfilled the selection criteria and their data were analysed. Median tracheostomy free survival from symptom onset was 28 months in NIV-treated patients compared to 15 months in untreated (Univariate Cox regression HR=0.61 (0.51 to 0.73), p<0.001). The positive survival effect of NIV persisted when the model was adjusted for age, gender, riluzole and percutaneous endoscopic gastrostomy use (HR=0.72 (0.60 to 0.88, p=0.001). In contrast with the only randomised controlled trial, NIV statistically significantly increased survival by 19 months in those with ALS-bulbar onset (Univariate HR=0.50 (0.36 to 0.70), multivariate HR=0.59 (0.41 to 0.83)). These data confirm that NIV improves survival in MND/ALS. The overall magnitude of benefit is 13 months and was largest in those with ALS-bulbar disease. Future research should explore the optimal timing of NIV initiation within phenotypes in order to optimise respiratory function, quality of life and survival.
- MOTOR NEURON DISEASE
- SLEEP
Statistics from Altmetric.com
Background
Amyotrophic lateral sclerosis/motor neurone disease (ALS/MND) is a progressive neurodegenerative disorder that is associated with disability and death, usually within 3 years of onset.1 Previous research has demonstrated that within ALS/MND, four distinct clinical phenotypes have different rates of functional decline and survival times; ALS, flail arm, flail leg and primary lateral sclerosis (PLS).2 Patients with the ALS phenotype have the most rapid disease progression and within the ALS phenotype, the shortest survival time is observed in those with bulbar symptom onset.2 ,3
Respiratory failure is associated with significant morbidity and is the usual cause of death in people with ALS/MND.1 For this reason, supporting and maintaining respiratory function is regarded as an essential component of care.4 ,5 A significant advance in the respiratory management of ALS/MND was the discovery of the beneficial effects of non-invasive ventilation (NIV), in which the patient uses a mask ventilator system overnight during sleep. A small randomised controlled trial (RCT) found that NIV increased median survival in those without bulbar disease by 7 months and was associated with variable improvements in quality of life measures in all those studied.6 It is not known, however, whether the improvement seen in this controlled research trial would be apparent or as large in routine clinical practice, where a significant number of patients do not receive NIV because of differences in clinicians’ perception and knowledge about its benefits, lack of availability or patient refusal.7 In addition, it is unclear whether patients with different disease phenotypes equally benefit from this intervention.6 ,8
Assessing the effectiveness of interventions outside of traditional RCTs is considered an important priority for health services and outcomes research.9 The present study evaluated the impact of NIV in ALS/MND within routine clinical practice. Importantly it complements the sole RCT, providing realistic estimates of treatment effect sizes and external validity.10 ,11 We analysed data from a prospective clinical cohort to determine (1) the effect of NIV on survival in a clinical cohort, (2) whether there is a differential effect of NIV on survival across clinical phenotypes and (3) the effect of NIV on the rate of decline of respiratory function within and between clinical phenotypes.
Methods
Study design
Retrospective analysis of a prospectively collected cohort of all patients with ALS/MND recruited via a specialist, multidisciplinary clinic at the Bethlehem Hospital in Melbourne, Australia. The local ethics committee approved the study which is reported according to the STROBE statement.12
Setting
The clinic provides care to approximately 60% of people with ALS/MND living in the state of Victoria (approximate population of 5.5 million). Clinical reviews occur three to six monthly. The first use of NIV at the clinic was registered in 1991; however, NIV was not routinely prescribed until 2002, when the Victorian Respiratory Support Service (VRSS—a state-wide specialist NIV programme) joined the clinic. After 1999, criteria for offering NIV initiation followed the recommendations by the American Academy of Neurology ALS Practice Parameter (orthopnea or sniff nasal pressure <40 cm H2O or maximal inspiratory pressure (MIP) <−60 cm H2O or abnormal nocturnal oximetry or vital capacity <50%).13 If the team determines that ventilation is not required at the time of referral, patients are reviewed and offered ventilation when indicated. The VRSS does not routinely distinguish between those with or without bulbar dysfunction when ventilation is offered. NIV is typically implemented with a bi-level pressure ventilator in spontaneous timed mode with a face mask. If a patient cannot be adequately ventilated non-invasively, ventilation via a tracheostomy is discussed although this is used infrequently.4 Treatment with riluzole has been offered to all patients at the clinic since June 2003. Percutaneous endoscopic gastrostomy (PEG) has been offered since the early 1990s.
Data sources
The Bethlehem Hospital ALS/MND database was established in 1991. All patients were diagnosed by neurologists with extensive experience in caring for people with ALS/MND according to the El Escorial criteria (for diagnosis before 2000) or the modified El Escorial criteria (after 2000).14 Information recorded included: demographic details, date of initial symptom onset, region of initial symptom onset (bulbar, cervical or lumbar), presence of lower motor neuron (LMN) and/or upper motor neuron (UMN) signs, results of relevant investigations (ie, brain and spinal cord imaging, nerve conduction studies, electromyography, lumbar puncture and genetic testing), treatments undertaken and dates of initiation. Patients were considered to have received an intervention (ie, NIV, PEG, riluzole) when it was recorded in their files that the intervention was well tolerated and continued at least until the first follow-up appointment after initiation. Information on cognitive function, unsuccessful treatment trials and reasons for intolerance or discontinuation were not routinely available.
Patients were categorised into four clinical phenotypes (ALS, flail arm, flail leg and PLS) according to site of presenting symptom and the pattern of upper versus LMN involvement.2 Patients were designated as being in the ALS phenotype if they have mixed UMN and LMN signs in at least two regions and subgrouped according to their region of symptom onset (ALS-bulbar, ALS-cervical or ALS-lumbar). The Flail phenotype is defined in the presence of LMN signs with absent reflexes, beginning in either the arms (flail arm) or legs (flail leg). PLS is defined when there are only UMN signs in all three regions for at least 3 years.15
Since January 2002, patients routinely underwent spirometry (forced vital capacity (FVC), forced expiratory volume in 1 s (FEV1)) and respiratory muscle testing (MIP and maximal expiratory pressures (MEP) and sniff nasal inspiratory pressure (SNIP)) at each visit. Tests were performed according to ATS/ERS Guidelines.16 Sleep studies are performed when clinically indicated.
Participants
Data from all patients with ALS/MND included in the Bethlehem Hospital ALS/MND database between 1991 and 2011 were included. Patients were excluded from further analysis if data regarding disease phenotype, date of disease onset, date of death or date of last follow-up were not recorded. Patients with PLS were excluded from subsequent analyses as prognosis and response to interventions in this patient group are not comparable to other ALS/MND phenotypes.17
Outcomes
Tracheostomy-free survival (in months) was the primary outcome of interest. Survival was considered from onset of symptoms to either death, date of tracheostomy or censoring date of 31 December 2011. Date of death and date of tracheostomy were ascertained from clinic records. In cases for which we could not verify patient status to the end of the study (potentially ‘lost to follow-up’), we censored tracheostomy-free survival at the date that the patient was last known to be alive (usually last communication or clinic visit). Decline in pulmonary function was assessed with FVC, FEV1, MIP, MEP and SNIP. Only patients with at least two pre and two post NIV initiation pulmonary function tests were included in the analysis.
Statistical analysis
Baseline patient characteristics were compared using one-way analysis of variance or independent sample t tests for continuous variables and Pearson’s χ2 test for categorical variables. The Kaplan-Meier method was used to plot survival distributions in patients who did and did not receive NIV. Univariate Cox regression was used to derive unadjusted HRs for death. Multivariate Cox regression models were used to estimate covariate-adjusted risk of death. The multivariate Cox model included the following clinical and demographic factors that have been previously suggested to affect survival in ALS/MND, irrespective of their statistical effect: age of disease onset, gender, use of riluzole and use of PEG.18 To adjust the model for delayed entry in the study (left truncation), we considered patients to have entered the risk set at the time of index in the database (ie, date of first assessment at the clinic) and not at the origin of survival curves (ie, date of disease onset). To account for the changes in patient treatment in early 2003 (riluzole and VRSS participation), we stratified the analysis by time of index in the database (before and after 2003). A univariate survival model based on a matched cohort design was also developed as a sensitivity analysis to assess the robustness of the findings. Patients who used and who did not use NIV were matched 1:1 according to age at disease onset in deciles, gender and use of riluzole (n=240).
A mixed model analysis was utilised to assess the rate of decline of respiratory function (FVC, FEV1, MIP, MEP and SNIP) before and after NIV initiation. This model provided an analysis involving a ‘before and after’ comparison within patients who used NIV with the main parameter of interest being the interaction between use of NIV and time from NIV initiation. This parameter indicates the difference in pulmonary function slopes before and after NIV initiation in L/year (for FVC and FEV1) or cm H2O/year (for MIP, MEP and SNIP).
We performed statistical analyses for the full study cohort (all phenotypes), followed by a subgroup analysis with patients grouped according to their clinical phenotype. Results were considered statistically significant when p≤0.05 and/or 95% CIs did not include 1. Estimation of the effect size of NIV was exploratory and preplanned; therefore, no adjustments for multiple comparisons were made. More detailed statistical methods and the sensitivity analyses results are provided in the online supplementary material.
Role of the funding source
The research was supported by competitive grants awarded by the Bethlehem Griffith Research Foundation and the Motor Neurone Disease Research Institute of Australia. The funders had no role in study design, conduct, analysis of results or preparation of the manuscript.
Results
Between 1991 and 2011, 1198 patients diagnosed with ALS/MND were registered in the Bethlehem Hospital database. A total of 929 patients (77.5%) fulfilled the selection criteria and were included in the analysis (figure 1). Phenotypic distribution was: ALS-bulbar n=312 (33.5%), ALS-cervical n=240 (25.8%), ALS-lumbar n=295 (31.7%), flail arm n=62 (6.6%), flail leg n=21 (2.2%). As the flail arm and flail leg groups were small and the patterns of disease progression and survival are similar,2 ,19 we combined these into one group named flail limb n=83 (8.9%).

Flow diagram of patient inclusion.
Twenty-three per cent of the patients (n=219) were treated with NIV (table 1). The percentage of males was higher in the group treated with NIV (71.7% vs 52.8%; p<0.001) and the average age at disease onset was lower (58.3±11.5 vs 64.0±11.9; p<0.001). Use of riluzole (79.9% vs 35.2%; p<0.001) and PEG (58.9% vs 25.3%; p<0.001) was more frequent in patients treated with NIV. Use of NIV was non-significantly less frequent in patients with bulbar disease (18.6% (ALS-bulbar) vs 25.4% (ALS-cervical) vs 26.5% (ALS-lumbar) vs 26.5% (flail limb); p=0.08).
Demographic characteristics of patients included in the survival analysis
As shown in table 2, the average age at NIV initiation was higher and PEG insertion was more common in patients with bulbar symptom onset but riluzole prescription and gender were similar across phenotypes. Time from symptom onset to NIV initiation was shortest in the bulbar group but no differences across phenotypes were observed in pulmonary function and sleep test variables (including blood gas analysis) immediately prior to NIV initiation (see online supplementary tables S1 and S2).
Characteristics of patients who received NIV by phenotype
Survival analysis
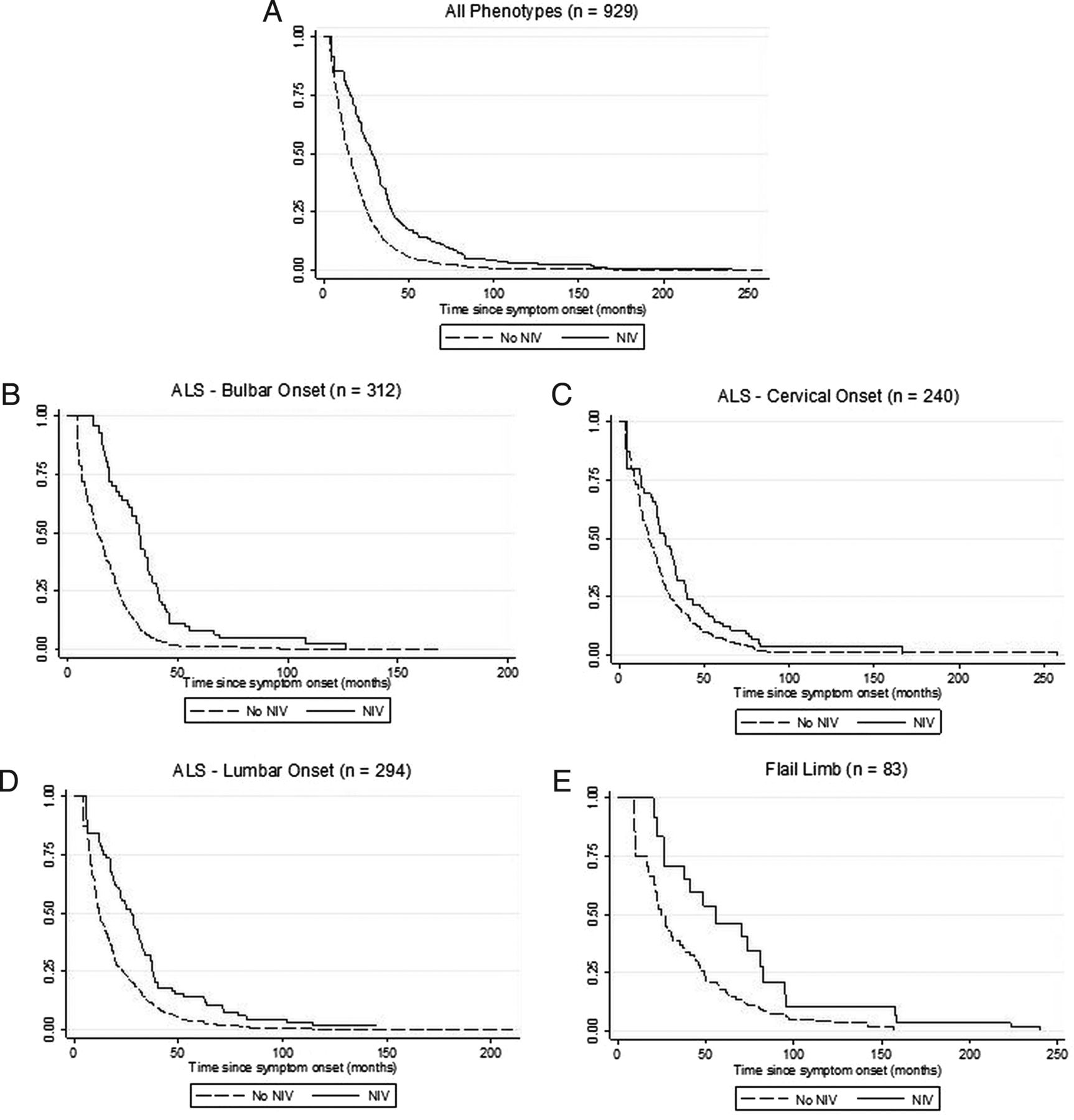
The Univariate Cox regression showed that those using NIV had almost a 40% increase in survival across all ALS phenotypes (HR=0.61, table 3 and see online supplementary table S3A–E). The positive survival effect of NIV persisted when the model was adjusted for age of disease onset, gender, use of riluzole and use of PEG (HR=0.72). Overall median tracheostomy free survival from symptom onset was 28 months in NIV-treated patients compared to 15 months in untreated (figure 2). In patients with ALS-bulbar, NIV significantly increased survival by 19 months (Univariate HR=0.50, multivariate HR=0.59). The observed survival advantage of NIV in patients with bulbar disease onset was confirmed in the sensitivity analyses using the matched cohort model (see online supplementary table S4A–F). In ALS-lumbar patients, NIV significantly increased survival in the univariate analysis (HR=0.62), but not after adjustment for covariates (HR=0.71; p=0.051). In patients with flail limb and ALS-cervical, the association between survival and NIV was not statistically significant (see online supplementary tables S3A–E).
Univariate and multivariate Cox-regression analysis for mortality

{kind=link}
{kind=link}
Kaplan-Meier survival curves according to non-invasive ventilation use in (A) all phenotypes, (B) amyotrophic lateral sclerosis (ALS) bulbar onset, (C) ALS cervical onset, (D) ALS lumbar onset and (E) flail limb.
Pulmonary function analysis
Rates of FVC, FEV1, MEP and MIP decline were significantly reduced overall after NIV initiation (table 4, see online supplementary table S5A–E and see online supplementary figures S1–S5). In the subgroup analyses, NIV initiation tended to have a positive effect on the rate of decline of pulmonary function variables in all phenotypes, but the magnitude and statistical significance varied across variables and phenotypes.
Differences in rate of decline in pulmonary function indices before and after NIV initiation
Discussion
Results from this Australian cohort study confirm the positive effect of NIV on survival of patients with ALS/MND. Our study also observed an overall benefit of NIV on the rate of respiratory decline in patients with ALS/MND, however, there was variation in the magnitude of effect across phenotypes and pulmonary function variables. A major strength of this study was that it involved a large sample of patients with ALS/MND treated in a specialist clinic whose data were accrued prospectively in a standardised format. Although previous studies suggested differences in the effect of NIV across ALS/MND subgroups, to the best of our knowledge, our analysis was the first specifically designed and sufficiently powered for this comparison.
We observed a greater benefit in patients who experienced bulbar onset of their disease, which conflicts with results from the only RCT.6 There are theoretical reasons to explain a lack of benefit of NIV on survival of patients with bulbar disease (eg, reduced tolerance to NIV, increased risk of lower respiratory tract infections from aspiration) and differing treatment approaches could also impact on NIV usage and outcomes, particularly in the bulbar phenotype. The current project regularly used full face masks with secretion management for nocturnal and daytime ventilation while the previous RCT also utilised mouthpieces for daytime ventilation.
It is possible that the difference between the Bourke RCT6 and cohort observations of improved or similar NIV survival in patients with bulbar involvement3 ,20 is due to a type 2 error. In the RCT only 21 patients were included in the bulbar subgroup analysis and the survival curves show a number of very early deaths in the control arm of the non-bulbar subgroup. It is possible that the sample of patients analysed in the only RCT was not large enough to represent the effect of NIV in bulbar disease and that these early deaths over-estimated non-bulbar survival confounding interpretation.
We speculate that the benefits of NIV we observed in bulbar disease may, in part, reflect earlier initiation.21 Our study showed that across the phenotypes, median time to NIV initiation (from disease onset) was shortest in patients with ALS-bulbar. There were no significant differences in pulmonary function before NIV initiation across phenotypes, however, we speculate that clinicians who typically care for patients with ALS know that ALS-bulbar can progress rapidly and thus they may relatively expedite NIV initiation in ‘suitable patients’ within this group. Future research that examines both the effect of timing of NIV initiation within phenotype and explores the clinical ‘drivers’ of NIV initiation is necessary to explore these hypotheses.
The observed benefits of NIV on pulmonary function decline corroborate previous literature.20 ,22 While the benefit was significant overall for FVC, FEV1, MIP and MEP, we found a wide variability in magnitude of effects across pulmonary function tests and phenotypes. This may reflect the difficulty patients have in reliably performing pulmonary function tests as weakness, particularly of the bulbar musculature, progresses or may simply reflect diminished statistical power across comparisons.
Another important strength of this research is the carefully executed survival analysis accounting for left truncation;23 a correction few previous observational survival studies in ALS/MND have made. If left truncation is ignored, survival times are typically overestimated as patients who did not survive until study entry (eg, diagnosis or entry in a database) are not represented in the analysis.24 ,25 In our cohort, median survival from disease onset was 17 months with adjustment for left truncation, compared to 29 months when left truncation was ignored. The later result is comparable to previous survival estimates in ALS/MND populations.2 ,19 ,26 ,27 It is likely that previous reports of unexpected decline in survival from ALS/MND resulted from a lack of adjustment for left truncation.28 Importantly, when not accounting for left truncation, observational studies on NIV in MND maybe be biased towards favourable survival in patients who did not use NIV. Therefore, the real survival benefits of NIV may be larger than the reported in previous cohort studies.3 ,20 ,22
This study has the limitations all observational studies experience in attributing causality; however, since the publication of the RCT by Bourke et al6 it is now arguably unethical to assess the effectiveness of NIV in MND populations using a randomised controlled design.29 Although we controlled our survival analysis for factors that previous literature suggested may influence survival, observational designs cannot allow for unknown prognostic factors that may be differentially distributed across the treatment and non-treatment cohorts (the Rumsfeldian ‘unknown unknowns’). Additionally, the data were clinic based and thus subject to referral bias. However, our data were analysed using an intention to treat approach, with all patients referred for NIV implementation included in the NIV group irrespective of actual use. Hence, the results may be considered a conservative estimate of benefit as it is highly likely actual NIV adherence was less than 100% as detailed adherence data were not available. Lastly, we did not comprehensively capture information on health-related quality of life and therefore, we could not confirm if the prolonged survival observed with NIV use was accompanied by improvements in patient well-being as previously reported.6
These data suggest that NIV has an important role in improving survival in MND/ALS. The magnitude of benefit is large at 13 months overall, compared with the 2–3 months attributable to riluzole.30 Access to NIV services is not universal,31 however, given the substantial clinical benefits observed in ALS/MND determining the cost/benefit of increased access to NIV services should be a priority. The observed benefit was largest in those with ALS-bulbar disease and while this may be partly attributable to earlier NIV initiation, the observed survival increase suggests NIV has a role in bulbar onset disease. We observed an overall reduction in pulmonary function decline, albeit variably distributed across phenotypes. Future research should explore the optimal timing and methods for initiating NIV within different phenotypes in order to optimise respiratory function, quality of life and survival.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online supplement
Footnotes
Contributors DJB, SM and PT initially conceived the study. DJB, JW, AS, FB, SM and PT contributed substantially to data acquisition. DJB, MEH, JFF, SVH, FJOD, JW, FB and PT contributed substantially to data analysis and all authors contributed to data interpretation. DJB took primary responsibility and JFF contributed substantially to the initial drafting of the manuscript. All authors contributed equally to critical revision of the manuscript, had final approval of the version to be published and have agreed to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Funding Bethlehem Griffith Research Foundation and the Motor Neurone Disease Research Institute of Australia.
Competing interests DJB, MEH, JFF, FB, FJOD, JW, SM and PT report a grant from the Bethlehem Griffith Research Foundation and a grant from the Motor Neurone Disease Research Institute of Australia during the conduct of the study. DJB and MEH report a grant from the Resmed Foundation outside the submitted work. PT reports grants from Biogen Idec and the Bethlehem Griffith Research Foundation outside the submitted work. SM reports a grant from Sanofi-Aventis outside the submitted work. AS was funded by Bethlehem Griffith Research Foundation for her contribution during the conduct of the study, by a grant funded by Biogen Idec outside the submitted work and is funded to date by the Bethlehem Griffiths Research Foundation for ongoing work on the Australian Motor Neurone Disease Registry.
Ethics approval Bethlehem Hospital Human Ethics Board, Melbourne.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Additional summary data are available in the online supplementary figure. Further data requests should be directed to the corresponding author.