Article Text

Abstract
Objective There are inconsistent data on mortality in people with multiple sclerosis (MS). We performed a meta-analysis of all-cause, cause-specific and gender-specific crude mortality rates (CMRs), and standardised mortality ratios (SMRs) in MS, and estimated the rate of change of CMR and SMR over the past 50 years.
Methods Medline, Embase and the Cochrane Library were searched. Keywords: ‘Multiple Sclerosis’ and (‘standardised mortality’ or ‘standardized mortality’). Inclusion criteria: availability of data on the number of deaths; mean or median patient follow-up or reports of SMRs; being a longitudinal study. 12 studies were included covering the period 1949–2012 (27 423 patients; 6628 deaths; 437 832 person-years follow-up). CMR was calculated. SMRs were extracted. CMRs and natural logarithm of SMRs were pooled by the method of the inverse of the variance. Meta-regression models were used to investigate the secular trends.
Results Pooled CMR was 9.78/1000 person-years (95% CI 6.81 to 14.02). Pooled all-cause SMR was 2.80 (95% CI 2.74 to 2.87). All-cause SMR was 2.56 (95% CI 2.47 to 2.66) in males and 3.06 (95% CI 2.97 to 3.17) in females. SMR due to cancer was 0.89 (95% CI 0.83 to 0.97). SMRs due to cardiovascular diseases, suicide, infection and respiratory diseases were 1.29 (95% CI 1.20 to 1.38), 2.13 (95% CI 1.80 to 2.51) and 2.91 (95% CI 2.60 to 3.26). There was no trend in CMRs, all-cause, and gender-specific SMRs.
Conclusions The excess mortality in MS relative to the general population has not changed over the past 50 years. Female patients with MS have higher survival disadvantage compared to that of males. Death due to cardiovascular diseases, suicide and infection is higher in patients with MS compared to the general population.
- MULTIPLE SCLEROSIS
- EPIDEMIOLOGY
Statistics from Altmetric.com
Introduction
Patients with multiple sclerosis (MS) have an increased risk of premature death compared with the general population.1 The epidemiological features of MS have changed over the last decades2 and the lifespan of the general population has increased. Little is known about changes in MS mortality over time, and how these changes compare to trends in mortality in the general population.
Several observational studies on mortality in MS have been published, providing inconsistent results. For example, a study of the trend of standardised mortality ratios (SMRs; the ratio of observed deaths in a study group to expected deaths in the general population) in a large group of Danish patients with MS showed that SMR has halved from the period 1949–1958 to the period 1979–1988.3 In contrast, no evidence of improved relative mortality was noted in the British Columbia MS cohort over the period 1980–2007.4 Differences in study methodology and duration, and the increase in the lifespan of the general population, make comparing data on MS mortality challenging. In a recent review, Scalfari et al1 outlined the importance of death as clinical outcome in MS and highlighted the gaps in the current understanding of MS mortality. They emphasised the conflicting evidence in several aspects, such as: whether the relative survival has improved in patients with MS; causes of death in MS; and the relationship between gender and mortality. As disease-modifying treatments (DMTs) may significantly increase survival in MS,5 a better characterisation of MS mortality is needed to better understand the impact of DMTs on death as an outcome in MS.
The current gaps in knowledge and the lack of systematic studies evaluating cause-specific mortality ratios prompted us to perform a meta-analysis of crude mortality rates (CMR) and SMR to investigate the all-cause, cause-specific and gender-specific SMRs, and their trend over the time period covered by the available mortality studies in MS. CMR indicates the number of deaths occurring in a given period of time (usually 1000 person-years of follow-up time) in a cohort, and SMR indicates the mortality in a cohort relative to the mortality in a reference population. SMR use eliminates the effect of differing sex and age distributions in the two compared populations, and thus provides a better picture of changes in survival. Causes of death in patients with MS have been considered extensively in large population-based studies, but cause-specific SMRs have not yet been systematically studied. We used reported cause-specific SMRs in the studies included in our meta-analysis to investigate death due to cancer, cardiovascular diseases, respiratory diseases, infections and suicide in patients with MS.
Methods
In performing this study, we followed the PRISMA (Preferred Reporting Items for Systematic reviews and Meta-Analyses) protocol.6
Data source and search
Medline, Embase and the Cochrane Library up to November 2014 were searched using the keywords ‘multiple sclerosis’ and (‘standardised mortality’ or ‘standardized mortality’) with no time restriction. Two investigators working independently extracted data in a blinded approach from the literature databases and references of the identified papers.
Inclusion criteria
Inclusion criteria were the availability of data on the number of deaths and mean or median patient follow-up, reports of reports of overall all-cause SMR or an overall all-caused age-matched HR and being a longitudinal study. Only papers published in English were included. For multiple studies using the same cohort, the study with the longest duration of follow-up that met the study inclusion criteria was used. Where no cause specific SMRs were reported, either authors were contacted or relevant publications/reports were considered if they were based on the same cohort and material.
Data extraction
Total number of patients, number of deaths, mean or median duration of follow-up, person-year, type of study, study onset and publication date were extracted from the papers. CMR with 95% CIs were calculated. SMR with 95% CI were extracted for: total population, each sex, cancer, cardiovascular diseases, respiratory disease, infections and suicide. If the cause-specific SMR was not reported in the original paper, where available, it was obtained from the relevant publications from the same cohort.
Data analysis
For each study, CMR was calculated as follows: number of deaths during the study follow-up period divided by total person-year follow-up time. If the total person-year follow-up time was not reported, CMR was calculated by dividing the number of deaths by the mean (or median if mean was not available) study follow-up time multiplied by the total number of patients. The 95% CI for CMR was obtained by: and the 95% CI for SMR was obtained by:
and the 95% CI for SMR was obtained by: if it was not reported.7 The CMRs and SMRs were then pooled by the method of the inverse of the variance. Natural logarithms of the SMRs were used in our analyses as log-SMR has more normal sampling distribution and it is preferred when the reference population is different between studies.8 The pooled log-SMRs were then back-transformed for interpretation. The SE of log-SMR was estimated by
if it was not reported.7 The CMRs and SMRs were then pooled by the method of the inverse of the variance. Natural logarithms of the SMRs were used in our analyses as log-SMR has more normal sampling distribution and it is preferred when the reference population is different between studies.8 The pooled log-SMRs were then back-transformed for interpretation. The SE of log-SMR was estimated by  8 or ln(SMR Upper CI/SMR Lower CI)/3.92.9 SE was used as study weights in the meta-regression models when assessing the influence of time on SMRs.
8 or ln(SMR Upper CI/SMR Lower CI)/3.92.9 SE was used as study weights in the meta-regression models when assessing the influence of time on SMRs.
To examine how SMR and CMR change over time, a meta-regression model was used (with CMR or Log-SMR being the dependent variable and the middle year of the follow-up period being the independent variable).
We used random effects models for analysis of CMR and fixed effect models for the analysis of SMR. Heterogeneity was measured by the I2.10 In case of high heterogeneity, subset analysis was repeated multiple times, with removal of one or more studies each time to investigate the source of high heterogeneity. Cause specific SMRs were pooled for mortality due to cancer, cardiovascular disease and suicide. A funnel plot was used as a visual tool for assessment of publication bias and Egger's regression test was used for the investigation of small study bias.
All statistical analyses were performed with Stata V.12 (StataCorp, 2009, Stata Statistical Software: Release 12, College Station, Texas, USA: StataCorp LP).
Results
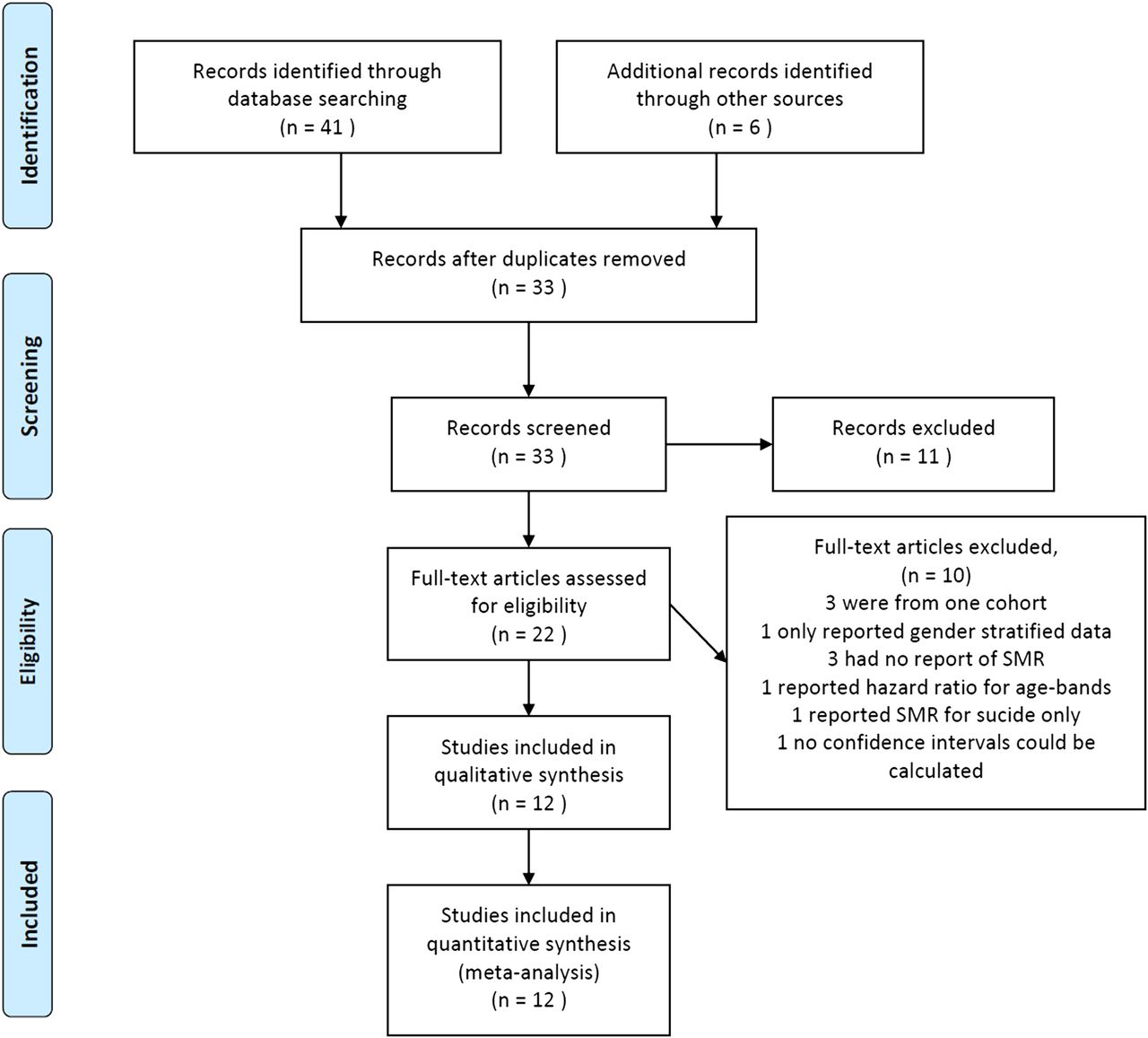
The online search identified 41 publications. Six additional articles were identified from the other sources. Eight articles were not related to mortality in MS, three were conference papers and 14 were duplicates. Full-text review was performed on the remaining 22 articles. Of these, four were from the same cohort (Danish MS cohort), hence three were excluded. One study had only reports of gender stratified regional SMRs but no reports of overall SMR.11 One study only reported mortality rates for age groups.12 No SMR was reported in two studies.13 ,14 One study was excluded due to reports of SMR for suicide only but not overall SMR.15 Three studies reported SMR but not the CI. However, 95% CI could be calculated for two,16 ,17 but the third was excluded due to lack of data.18 A recent study on causes of death in MS did not report SMRs and was therefore excluded.19
Overall, 12 studies were included3 ,4 ,16 ,17 ,20–27 (figure 1). Table 1 summarises the included studies.
Summary of the included studies
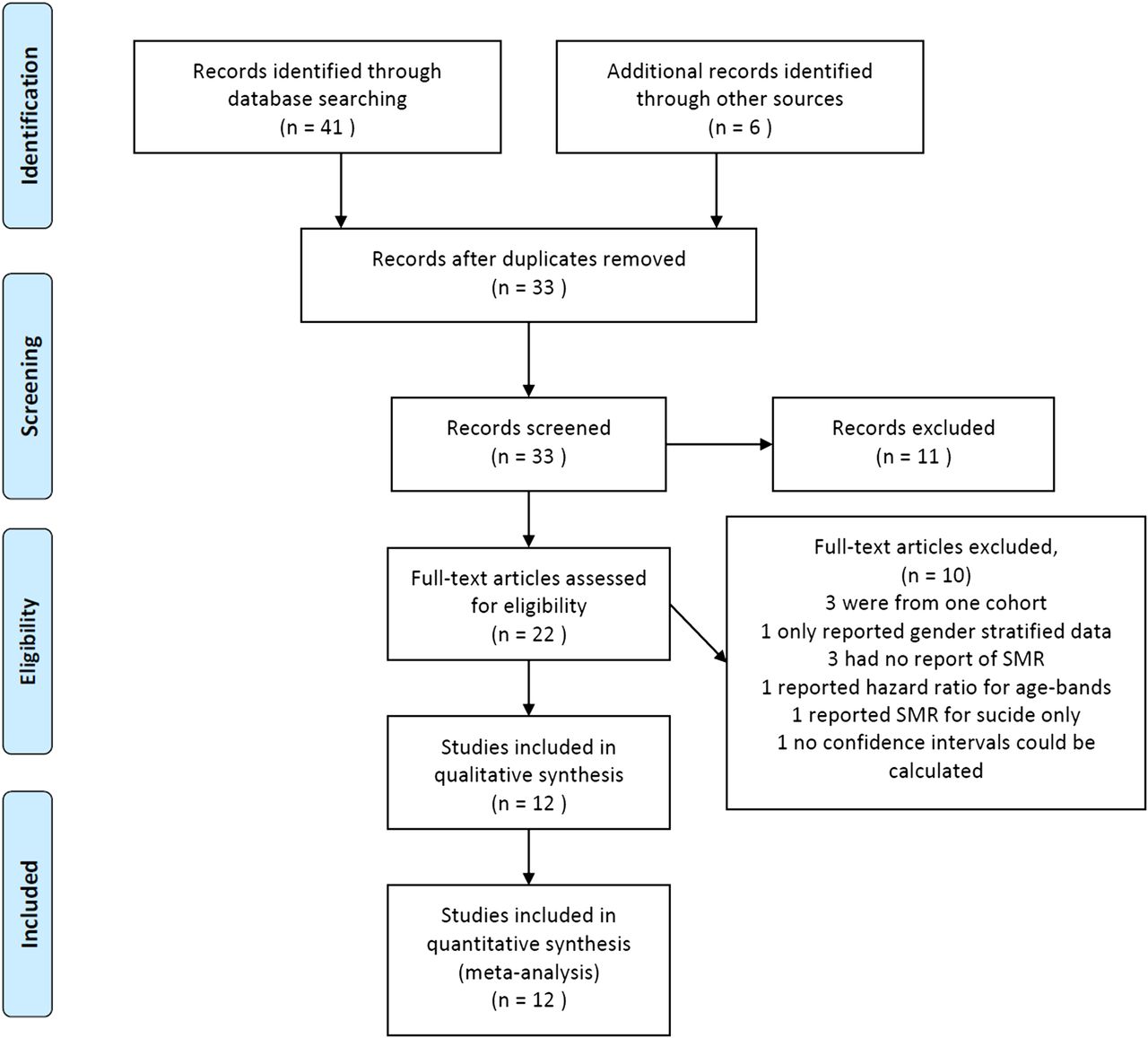
Flow chart of the study procedure.
These studies comprised data from 28 706 patients. A total of 6628 deaths occurred during 437 832 person-year follow-up time, ranging from 2.8/1000 person-years in France to 38.8/1000 person-years in Wales. The pooled CMR was 9.78/1000 person-years (95% CI 6.81 to 14.02, I2=99.2%, p<0.001) (figure 2).

Forest plot of crude mortality rates (CMR) sorted by cohort's follow-up period midpoint year.
The pooled SMR was calculated from the extracted SMRs for both sexes and each sex separately. SMRs ranged from 1.30 (95% CI 1.00 to 1.70) in France to 3.51 (95% CI 2.63 to 4.69) in the UK. The pooled SMR was 2.80 (95% CI 2.74 to 2.87, I2=85.2%, p<0.001) including both sexes (figure 3), 2.56 (95% CI 2.47 to 2.66, I2=74.7%, p<0.001) for men and 3.06 (95% CI 2.97 to 3.17, I2=77.5%, p<0.001) for women.

Forest plot of standardised mortality ratios (SMR) sorted by cohorts’ follow-up period midpoint year.
Heterogeneity in SMR
The sensitivity analysis of the models showed that three studies16 ,22 ,27 explained the high heterogeneity. Therefore, in the subset analysis, the SMRs from these three articles were excluded and the pooled SMR was calculated. This resulted in slightly higher pooled SMRs but with almost no significant heterogeneity. The pooled SMR in the subset analysis was 2.86 (95% CI 2.79 to 2.93, I2=4.5%) including both genders, 2.60 (95% CI 2.50 to 2.70, I2=49.1%) for men and 3.12 (95% CI 3.02 to 3.22, I2=0.0%) for women.
Cause-specific SMRs
Seven studies reported SMRs for cancer and six studies reported SMRs for cardiovascular diseases. The suicide specific SMRs were obtained for five cohorts (two studies21 ,23 reported accident and suicide combined, and one study had no case of suicide,20 and no SMR for suicide was reported). SMR for suicide was not reported in our original paper and, therefore, it was calculated from the raw data. The suicide-specific SMRs for the British Columbia and Danish cohorts were obtained from their related publications.29 ,30
Five studies had reports of SMRs related to infection and respiratory disease. The pooled SMR was 0.89 (95% CI 0.83 to 0.97, I2=81.3%) for mortality due to cancer, 1.29 (95% CI 1.20 to 1.38, I2=60.8%) for mortality due to cardiovascular diseases, 2.13 (95% CI 1.80 to 2.51, I2=8.9%) for mortality due to suicide and 2.91 (95% CI 2.60 to 3.26, I2=97.6%) for mortality due to infection and respiratory diseases (figure 4).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Forest plot of cause specific standardised mortality rates (SMR) due to cancer, cardiovascular diseases, infection, respiratory diseases and suicide. SMR, standardised mortality ratio; CVD, cardiovascular disease; *SMR from accident and suicide combined, ¤Infection and respiratory diseases combined.
Trends over the time period covered by the studies
No evidence of trend towards change in CMR (coefficient 0.01 (deaths/1000 person/year), 95% CI −0.82 to 0.85), all-cause SMR (coefficient 0.002 (change in log-SMR/year), 95% CI −0.01 to 0.02), SMR in males (coefficient 0.002, 95% CI: −0.01 to 0.02), or SMR in females (coefficient −0.001, 95% CI −0.02 to 0.01) was found in the time period covered by the studies using meta-regression models (see online supplementary figure e-1).
Publication bias
Visual inspection of the funnel plot (see online supplementary figure e-2) revealed an asymmetry in the result of all-cause SMR. Further inspection of the data using Egger's regression test confirmed the presence of small study bias where small studies consistently reported lower SMR (p=0.02). Exclusion of the three studies16 ,22 ,27 that were identified as the source of heterogeneity resulted in a non-significant Egger's test (p=0.17). Therefore, the asymmetry of the funnel plot and possibly the heterogeneity of the results are more likely to be due to the small study effect than publication bias.
Discussion
We performed, to the best our knowledge, the first meta-analysis of mortality studies in MS that pools all-cause and cause-specific SMRs. The pooled all-cause SMR of 2.80 suggests that patients with MS are at higher risk of death compared to their age-matched and sex-matched counterparts in the general population. While this is not altogether unexpected, in view of available mortality studies in people with MS, we show that over the past 50 years, the mortality in MS has not changed when compared to the general population, despite changes in MS epidemiology and overall increase in patients’ life span. The lack of change in SMR over the time-period covered by this meta-analysis suggests that the reported increase in MS survival rates parallels the increased life expectancy in the general population.
We used SMRs to study the impact of gender on MS mortality. This meta-analysis shows that women with MS have survival disadvantage compared to males. Although female patients with MS may have a better clinical prognosis in terms of reaching long-term disability,31 they have higher SMR than males. This contributes to the clarification of the conflicting reports about the relationship between sex and mortality in people with MS.4 ,22–24 ,28 ,32 ,33 The variability of reported survival rates of women with MS can be attributed to differences in methodology (eg, calculating CMR only) or changes in sex ratio in MS over time reported by some epidemiological studies in MS.34 The increased mortality in women with MS cannot be explained by an increase over time in the number of female patients with MS in the studied cohorts, as it derives from the SMRs that are independent of gender ratio. Studies are needed to clarify the effect of ageing and comorbidities on MS gender-specific mortality.
Survival has unambiguous face validity and can be a valuable outcome measure when assessing the effect of treatments.5 The follow-up of the original interferon β trial,5 an investigation in our centre of the impact of smoking on mortality27 and a follow-up study of patients with MS in Taiwan,35 have all shown lower mortality risks in patients who have been exposed to DMTs. In this meta-analysis, data were not sufficient to allow for measuring the effect of treatments on survival in patients with MS. However, we show a survival disadvantage in patients with MS that is sustained over time and suggests that, although the life span of people with MS has improved compared with a generation ago, the increased mortality in MS remains an actual and stringent unmet need. The results of this meta-analysis set a benchmark for future population studies taking on DMT effects of mortality in patients with MS.
Considerable heterogeneity was present in some of the analyses, possibly caused by the studies being small. Studies by Leray et al,22 Sadovnick et al16 and our data,27 explained much of the heterogeneity (almost 65%). The subset analysis of pooled SMRs after exclusion of these three studies resulted in slightly higher pooled SMR (2.86 vs 2.80) and almost no significant heterogeneity, and confirmed the sustained survival disadvantage in patients with MS.
We show that while the mortality due to cancer was decreased (SMR 0.89) in patients with MS, the mortalities due to cardiovascular diseases, suicide and infection and respiratory diseases were, respectively, increased by 1.29, 2.13 and 2.90-times in people with MS compared with the general population.
The increased mortality due to infection and respiratory disease is in line with previous epidemiological and mortality reports in MS.19–21 ,23 This might be explained in part by MS being a direct cause of respiratory dysfunction.36 ,37
The different categorisation of infection and respiratory diseases may be responsible for the heterogeneous distribution of SMRs (figure 4). For example, Smestad et al23 and Lalmohamed et al,21 reported SMR for all infections without including respiratory diseases other than infection as cause of death. This may suggest that the cumulative contribution to overall mortality of infections and non-infectious respiratory disease (including aspiration) could be in fact higher.
There is conflicting evidence regarding cancer as cause of death in patients with MS. UK and Norwegian observational studies21 ,26 found an increased cancer-related mortality rate in patients with MS versus matched controls, whereas data from the Danish cohort showed the opposite.3 This discrepancy may partially be explained by the difference in utilising all21 or only the first entry3 of death certificate data, and differences in duration of follow-up (shorter follow-up is less likely to capture patients with advanced MS who are more likely to die from MS-related conditions).21
We use SMRs to show that mortality from cancer is decreased in patients with MS when compared with matched controls from the general population. This finding is in agreement with the lower risk for malignancies in people with MS, as previously described.38 A recent mortality study following the diagnosis of brain tumour in patients with MS showed that brain tumours and associated treatment do not increase mortality risk in patients with MS more than in people without MS, and that earlier detection due to more frequent MS-related investigations may even contribute to a reduced mortality risk in this group.39
The results of this meta-analysis show SMR of 1.29 for mortality due to cardiovascular disease in patients with MS compared to the general population. A systematic review of epidemiological studies examining comorbidities in people with MS recently pointed out that patients with MS have an increased risk for cardiovascular disease.40 However, it is not clear if this risk is related to a clustering of vascular risk factors or changes in body composition in patients with MS.40 Women with MS seem at higher cardiovascular risk. A recent nationwide study in Sweden reported that female patients with MS had an elevated risk of myocardial infarction, stroke and heart failure compared to men.41 In the Danish cohort, the higher mortality from cardiovascular disease among patients with MS was more pronounced among women.3 ,42 The lack of reported specific cause-related and gender-related SMR did not allow us to weigh the impact of gender on mortality from cardiovascular causes. However, the increased SMR related to cardiovascular disease suggests that careful surveillance and preventive measures for cardiovascular disease are warranted for patients with MS. Further research should be performed to explore the cause of this association between MS and cardiovascular disease, in particular with regard to the risk of premature death in women with MS.
The risk of suicide is increased in patients with MS compared with the general population and it has been previously suggested that suicide should be included among MS-related causes of death.1 This meta-analysis of SMRs shows that patients with MS have two times higher risk of suicide than matched controls. Regional variations must be considered when mortality ratios from suicide are analysed, as the varying crude rates reported in different populations may reflect ethnic and cultural differences. While very small numbers of suicide cases were reported from the studies performed in the UK (one study reported no case of suicide among 379 deaths),20 the SMR due to suicide is significantly increased in the studies conducted in Canada and Denmark. The results of our analysis warn against underestimating suicide as a cause of mortality in patients with MS.
A limitation of our study is that most of the cohorts included in our analysis were from Northern Europe and Canada, with no reports of SMR available from the USA or from countries with lower incidence and prevalence of MS. A recent study on commercially insured patients with MS in the USA used a novel algorithm for identifying from death certificates the cause most directly leading to death.19 Differences in mortality rates between patients with MS and non-MS matched controls were explained by infections, pulmonary disease and cardiovascular conditions.19 However, this study was not included in this meta-analysis as it did not report SMRs.
Secondly, pooling SMRs from different populations may be biased by differences in methodology between individual studies. SMR reflects a relative ratio and depends on duration of follow-up, as well as on the mortality rates in the reference population. In addition, 79% of the deaths contributing to the overall SMRs are derived from Danish and Canadian (British Columbia) cohorts contributing the highest number of patients. Therefore, our overall estimates are largely dominated by these cohorts. On the other hand, these studies may provide more accurate estimates than others due to their large sample size and population-based nature.
The studies included in the meta-analysis were carried out at different time periods and this may account in part for SMRs heterogeneity, as more recent studies may have better ascertainment. Some duplicate deaths have also been included in the meta-analysis as the cohorts in References 4 and 16 overlap partially. As the older results from 16 were removed in the sensitivity analysis, the inclusion of these duplicate cases has not influenced the final results of the overall SMR.
A limitation is the study of secular trends from different study cohorts by the means of a single measure. Averaged SMRs generated over long periods of time may not detect absolute changes in mortality over time in a given cohort, as they are a rather crude measure of change in relative mortality risk over time. Nevertheless, a single summary statistic of available SMRs is highly informative. We show that the reported SMRs from available mortality studies in MS are essentially the same over almost 50 years, and this is consistently shown by the subset analysis with low heterogeneity.
Excess death rates (EDRs) were not used in our analysis, since they were not reported by the studies included in the meta-analysis. EDRs are calculated as a difference between the observed death rates and the expected number of deaths based on age, sex, race and other covariates, and would allow comparisons of excess mortality for different periods of time.1 ,23 To provide a comprehensive and quantitative analysis of survival in MS, future mortality studies should include EDRs, SMRs and gender stratified CMRs, among the variables reported.
Despite the number of studies that have been conducted on causes of death in people with MS, environmental and life-style parameters that could impact survival have not been thoroughly evaluated. Chronic tobacco use, obesity, sedentary lifestyle and insufficient levels of vitamin D, may contribute to the maintenance of a proinflammatory state, and have been associated with a worse disease course and worse general health. As awareness increases, patients’ attitude towards those factors may change over time. We recently showed smoking being a risk determinant for all-cause and MS-related death.27 Modifiable life-style factors (eg, body mass index), which may influence mortality, need to be thoroughly addressed.
The current availability of DMT is likely to change future mortality figures in people with MS. This meta-analysis of SMRs provides valuable information regarding mortality in MS mostly in the absence of DMT, which should be considered when survival is used as long-term end point in large clinical trials. Based on our results, there is strong epidemiologic evidence that, regardless of gender, patients with MS have significantly higher mortality rates compared with the general population, and this has not changed over the past 50 years. Mortality due to cardiovascular diseases and suicide should be further investigated, as those are modifiable factors that can impact long-term prognosis and survival in people with MS.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online figures
Footnotes
Contributors AM was involved in study concept and design, acquisition, analysis and interpretation of the data and critical revision of the manuscript for important intellectual content. RT was involved in acquisition of data, study concept and design, analysis and interpretation of the data, and critical revision of the manuscript for important intellectual content. CRT was involved in critical revision of the manuscript for important intellectual content. CSC was involved in developing the study concept and design, acquisition of data and critical revision of the manuscript for important intellectual content.
Competing interests None.
Provenance and peer review Not commissioned; externally peer reviewed.