Article Text

Abstract
Background and Objective The relationship between repeated concussions and neurodegenerative disease has received significant attention, particularly research in postmortem samples. Our objective was to characterise retired professional ice hockey players’ cognitive and psychosocial functioning in relation to concussion exposure and apolipoprotein ε4 status.
Methods Alumni athletes (N=33, aged 34–71 years) and an age-matched sample of comparison participants (N=18) were administered measures of cognitive function and questionnaires concerning psychosocial and psychiatric functioning.
Results No significant group differences were found on neuropsychological measures of speeded attention, verbal memory or visuospatial functions, nor were significant differences observed on computerised measures of response speed, inhibitory control and visuospatial problem solving. Reliable group differences in cognitive performance were observed on tests of executive and intellectual function; performance on these measures was associated with concussion exposure. Group differences were observed for cognitive, affective and behavioural impairment on psychosocial questionnaires and psychiatric diagnoses. There was no evidence of differential effects associated with age in the alumni athletes. Possession of an apolipoprotein ε4 allele was associated with increased endorsement of psychiatric complaints, but not with objective cognitive performance.
Conclusions We found only subtle objective cognitive impairment in alumni athletes in the context of high subjective complaints and psychiatric impairment. Apolipoprotein ε4 status related to psychiatric, but not cognitive status. These findings provide benchmarks for the degree of cognitive and behavioural impairment in retired professional athletes and a point of comparison for future neuroimaging and longitudinal studies.
Statistics from Altmetric.com
Introduction
Each year, 1.6–3.8 million individuals in the USA sustain a mild traumatic brain injury (TBI) or sports-related concussion.1 TBI is associated with deficits in speed, attention and executive functioning that typically recover with time,2 as well as psychosocial impairments and psychiatric symptoms.3 ,4 In mild TBI and sports-related concussion, these impairments are typically short-lived,5 ,6 with full recovery for most expected within months.7
Relatively little research has been conducted on the remote effects of repetitive mild TBI or sports concussion on neuropsychological and cognitive function with ageing. Individuals who have participated in high-level (ie, university or professional) contact sports provide a unique opportunity to assess these effects, as they have a wide range of concussion exposure that can be related to remote outcome. Research findings concerning cognitive and neurological outcomes of these individuals are heterogeneous. While there is evidence for greater than expected cognitive impairment in former university and professional athletes8–10 (for exception, see Casson et al,11) interpretation of these data is affected by small sample sizes, the use of subjective cognitive ratings or psychiatric comorbidity. Turning to neuropathology, a high proportion of brains donated by former athletes show evidence of chronic traumatic encephalopathy (CTE),12 yet the true incidence of brain disease in the population of individuals with a history of remote repetitive TBI cannot be estimated from these data, as those donating their brains to registries for dementia and CTE are most likely unrepresentative of this population.13–15 More generally, remote TBI has been associated with increased incidence or earlier onset of neurodegenerative disease (MCI,8 ,16–18 AD,19 ALS,20 except see Crane et al,21) especially among those at elevated genetic risk due to possession of one or two apolipoprotein ε4 alleles.22 ,23
The majority of recent published research on retired professional athletes concerns football players (for exception, see De Beaumont et al9 and Tremblay et al,24) with earlier literature focusing on boxing.22 In order to determine the generalisation of findings in professional athletes, there is a need to extend this research to other contact sports. In the present study, we administered a comprehensive battery of neuropsychological, computerised cognitive and psychosocial tests along with a psychiatric interview to retired professional ice hockey players and age-matched comparison participants. The goal of this study was to characterise the presence and nature of cognitive and psychosocial deficits in alumni athletes and their relationship to ageing and concussion history. Given the interaction of the apolipoprotein ε4 allele with neurodegenerative disease and cognitive impairment following TBI,22 ,23 ,25 we considered ε4 status in exploratory analyses.
Methods and materials
Participants
The alumni group (N=38) was largely composed of former National Hockey League players (NHL; N=32), with the remainder from other professional and minor professional leagues. The alumni athletes were recruited through the NHL Alumni Association by email, media presentations, participation in local pro-AM hockey tournaments and word of mouth. An age-matched comparison group of healthy males (N=20) was recruited from the community. These comparison participants were screened for neurological conditions (including significant TBI as defined by loss of consciousness >5 min or post-traumatic amnesia >24 hours) and other medical conditions affecting cognitive functioning. Ultimately, none of our comparison participants had a significant TBI (max loss of consciousness=2 min; max post-traumatic amnesia=6 hours), although one was excluded due to a history of concussion with extended postconcussion symptoms. Another comparison participant was diagnosed with Parkinson's disease shortly after completing testing and was thus excluded. Two alumni (aged 65 and 85 years) were severely cognitively impaired (Montreal Cognitive Assessment scores of 7 and 12 out of 30) and did not participate in the study due to inability to complete the testing. An additional alumnus was excluded due to lingering effects of major surgery. Two alumni who enrolled in the study did not return to complete testing and were therefore excluded. The final N's were 33 in the alumni group and 18 in the comparison group. All participants were told that the overall aim of the study was to understand brain health in ageing alumni athletes. They provided informed consent in accordance with the institutional ethics guidelines and were compensated for participation.
Participants completed a standard neurological examination as well as two MRI scans of the brain (one structural and one combined EEG/fMRI), a blood draw for genotyping and (when possible) a lumbar puncture for analysis of cerebrospinal fluid proteins related to dementia. Aside from one incidental finding (arachnoid cyst in the left temporal lobe of one alumnus), no other gross abnormalities were found on structural MRI. Six alumni and one comparison participant could not have structural scans due to MRI exclusion (eg, implants).
On neurological examination one alumnus participant had mild Parkinsonism features, but not a diagnosis of Parkinson's disease. One alumnus had a long-standing seizure disorder that was controlled by medication. Otherwise, all participants were neurologically normal, with no evidence of dementia or other neurological disorders affecting cognitive functioning. (The neurological examination was not completed in one alumnus and six comparison participants). As shown in table 1, the two groups were age-matched, but the alumni had significantly lower education. This finding was expected, as NHL players are typically drafted out of high school. We also coded participants’ occupation according to the United States Department of Labor Occupational Information Network (O×NET) Job Zone classification, a five-level rating that reflects the degree of education, training and experience required for a given profession. By this measure, there was no difference between the alumni and comparison participants, t(49)=1.21, p=0.30, suggesting that they have a similar level of lifetime cognitive engagement in spite of the difference in educational attainment.
Participant characteristics
We administered the Structured Clinical Interview of the Diagnostic Statistical Manual-IV Axis I disorders—clinician version (SCID-IV)26 for psychiatric diagnosis according to DSM-IV criteria. (Two comparison participants and one alumnus did not complete the SCID.) We identified 19 alumni (59%) and 3 comparison participants (19%) with current or past psychiatric diagnoses, a significant difference, χ2(1, N=48)=7.09, p=0.008. Among alumni, the psychiatric diagnoses included alcohol abuse (6 past, 1 current), alcohol dependence (6 past, 1 current), non-alcoholic substance abuse (2 past, 1 current), non-alcoholic substance dependence (1 past), major depressive disorder (4 past, 4 current), antidepressant-induced mood disorder with depressive features (1 past), panic disorder (1 current), bipolar disorder (2 current), post-traumatic stress disorder (2 past) and obsessive compulsive disorder (1 current). Altogether, 10 alumni had a SCID-based diagnosis at the time of testing. One alumnus reported steroid use and nine (27%) reported a history of opiate use, four (12%) of whom were taking opiates at the time of testing. Among comparison participants, two had past major depressive disorder (single episode) and one had past alcohol abuse.
A lifespan TBI history was garnered from all participants, including TBI experienced outside of sport, the approximate date of each injury along with post-traumatic symptoms. Concussion was defined as a blow to the head followed by clinical symptoms, including altered consciousness, confusion, dizziness, headache, fogginess, memory problems and sensitivity to light or sound.27 ,28 Only concussions reported from ≥15 years of age were included in the analyses. Subconcussive impacts were not quantified. As expected, there were significantly more concussions among the alumni relative to comparison participants (see table 1).
Neuropsychological, computerised and psychosocial measures
Participants completed a battery of standardised neuropsychological tests, computerised cognitive tests and psychosocial outcome questionnaires (see tables 2⇓–4). The neuropsychological test battery assessed intellectual functioning, speeded attention, memory, visuospatial processing and executive functioning (see table 2). Computerised tests included measures from the CogState battery29 and selected measures from the Cambridge Brain Sciences (CBS) battery30 (see table 3) implemented locally on a standalone machine. A battery of psychological and psychosocial outcomes included measures of psychiatric symptoms and self-reported and informant-reported cognitive and behavioural deficits (see table 4). One alumnus and one comparison participant did not complete the computerised tests, and one comparison participant did not complete the questionnaires.
Factor loadings for the neuropsychological measures
Factor loadings for the computerised cognitive measures
Factor loadings for the psychosocial measures
Principal components analysis (PCA) was used to identify the latent structure within each of the neuropsychological, computerised and psychosocial batteries for the purpose of dimensionality reduction. To increase the stability of the factor structure, we added data from other participants tested in neuropsychological research conducted in our laboratory (for neuropsychological tests: N=52; mean age=54.2 years, SD=10.3; for computerised tests: N=193; mean age=44.5, SD=21.3; for questionnaires: N=51; mean age=54.4, SD=10.4). To avoid listwise deletion of participants, missing values were replaced with group means. This affected 0.34%, 0.43% and 3.64% of scores from the neuropsychological, computerised and psychosocial tests, respectively, for the alumni and comparison participants. Data were transformed if significantly skewed (p<0.05; using square root, arcsine or log10) to improve estimation of correlation structure. Cognitive test scores were inverted where necessary so that high scores always indicated good test performance. Point of inflection on a scree plot was used to determine the salient number of factors. After extracting this number of factors, a direct oblique (non-orthogonal) rotation with max iterations of 50 for convergence, a delta=0 (ie, direct quartimin rotation) and Kaiser normalisation were performed using the Statistical Package for the Social Sciences (SPSS; V.22) on the psychosocial, neuropsychological and computerised test batteries.
For the neuropsychological battery, four factors were identified: visuospatial, verbal memory, speeded attention and executive/intellectual function. As seen in table 2, this latter factor included tests of executive functioning (Wisconsin Card Sorting Test (WCST) perseverative errors) and intellectual ability (Wechsler Abbreviated Scale of Intelligence (WASI) vocabulary, similarities and matrix reasoning subtests). Since these measures can be considered to reflect independent neuropsychological constructs, we examined them individually to determine their contribution to the identified effects with this factor. For the computerised test battery, three factors were identified: response speed, inhibitory control and visuospatial problem solving (table 3). For the psychosocial battery, the factors were self-report, informant-report and psychiatric symptoms (table 4).
Participants donated a 30 mL sample of blood. DNA was extracted from the whole blood following standard high salt procedures. The apolipoprotein gene was amplified and genotyped using ABI TaqMan 5í-exonuclease Assays-by-Design™ using the ABI-7500 Sequence Detection System (Applied Biosystems, Canada). Nine alumni and four comparison participants had an apolipoprotein ε4 allele; one alumnus had two ε4 alleles and two had an ε2/ε4 profile; the remainder were classified as ε2/ε3 or ε3/ε3 (blood samples were not collected from three comparison participants and one alumnus). Participants were not informed of their apolipoprotein ε4 status, which can influence subjective cognitive performance.31
We first examined differences in cognitive performance and psychosocial function between alumni and comparison participants using three mixed-model multivariate analyses of variance (MANOVA) for neuropsychological, computerised and psychosocial tests, with factor scores (see above) as a within-participants factor and group (alumni vs comparison participants) as a between-participants factor. These tests were repeated for two groups of alumni defined by apolipoprotein ε4 status. Post hoc tests were evaluated after correcting for family-wise error using the Bonferroni correction. We next conducted regression analyses in which factor scores within each of the neuropsychological, computerised and psychosocial batteries were predicted using mean-centred age and group (coded as 0 and 1 for alumni and comparison participants, respectively), followed by the Age×Group interaction to test the hypothesis of differential ageing effects across groups.32 Finally, we used regression to assess the relationship of concussion history to neuropsychological, computerised and psychosocial factor scores after accounting for variance due to age in the alumni group.
Results
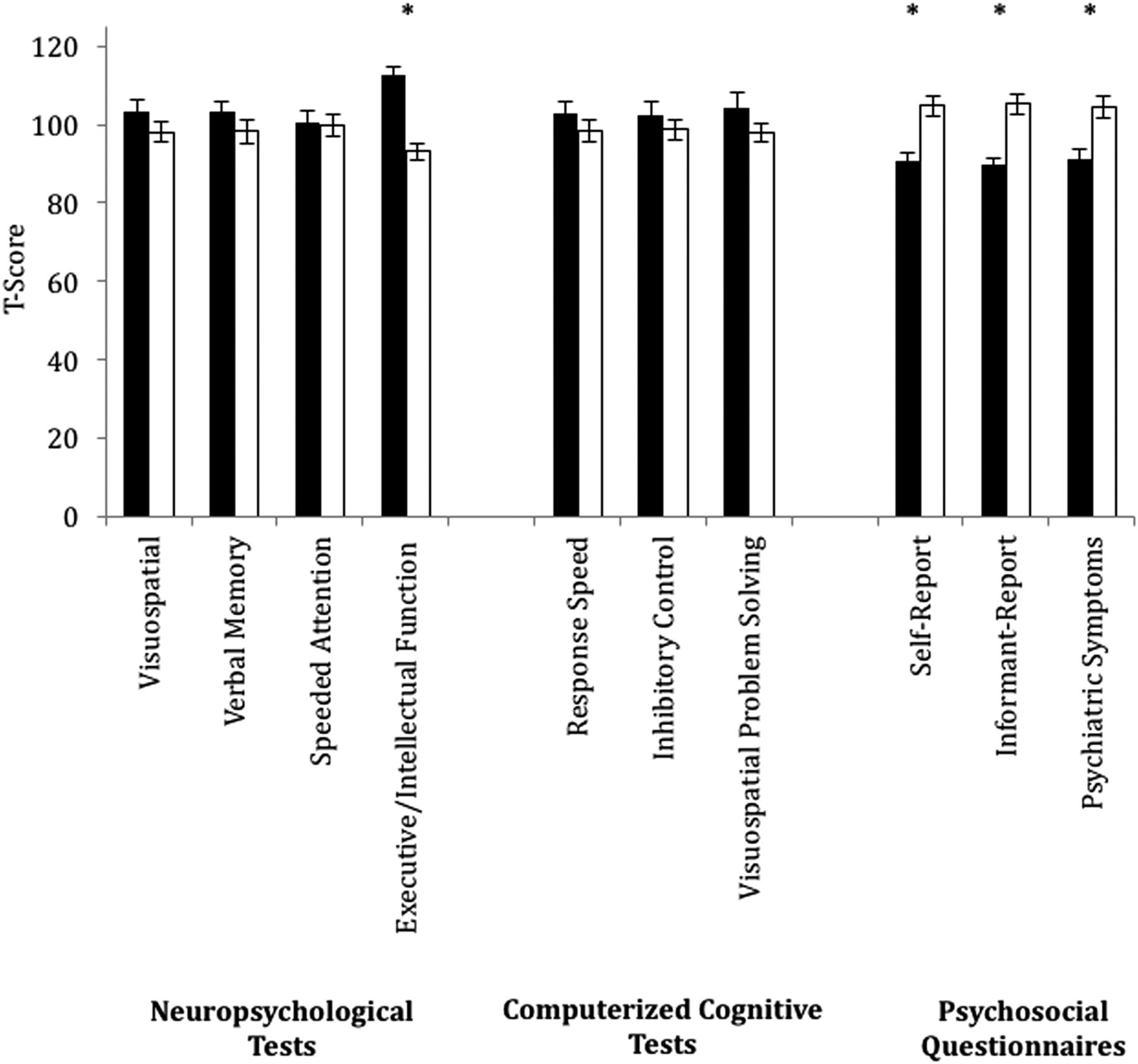
There was a significant main effect of group on neuropsychological performance, F(1, 49)=7.39, p=0.009, η2=0.131, which was qualified by a Group × Factor interaction, F(3,147)=4.39, p=0.005, η2=0.082 (figure 1). Follow-up tests using an adjusted α of 0.013 indicated lower performance on the executive/intellectual function, t(49)=5.53, p<0.001, in alumni relative to comparison participants. Since this factor score comprised one executive function (WCST) and three intellectual tests (WASI vocabulary, similarities and matrix reasoning), we probed these measures separately to determine if the results were specific to one or the other of these two domains. The group effect was evident on the WCST, t(43.41)=6.08, p<0.001; and WASI vocabulary, t(49)=4.43, p<0.001 and similarities, t(49)=2.17, p=0.035, but not matrix reasoning t(49)=1.95, p=0.057. There were no significant differences for the other factors (visuospatial, t(49)=1.18, p=0.25; verbal memory, t(49)=1.16, p=0.25; speeded attention, t(49)=0.16, p=0.87).
{kind=link}
Plots show mean scores for the four neuropsychological factors (visuospatial, verbal memory, speeded attention and executive/intellectual function), three computerised cognitive factors (response speed, inhibitory control and visuospatial problem solving) and three psychosocial factors (self-report, informant-report and psychiatric symptoms) for comparison participants (black bars) and alumni (white bars). For descriptive purposes, factor scores were transformed to standard scores (M=100, SD=15). The alumni participants performed similarly to the comparison participants on objective measures of cognitive performance, with the exception of executive/intellectual functioning, where their test scores were significantly lower than those of the comparison participants. The alumni participants showed greater endorsement across subjective measures of cognitive and psychiatric functioning relative to the comparison participants. Note: * represents a significant group difference (p<0.005).
There were no significant effects or interactions involving Group detected on the computerised cognitive test battery. For the psychosocial measures, there was a significant main effect of Group, F(1,48)=23.21, p<0.001, indicating generally elevated item endorsement on the psychosocial questionnaires in the alumni relative to the comparison group; the Group × Factor effect was not significant (see figure 1).
Expected effects of age were observed across alumni and comparison participants. For the neuropsychological tests, these included visuospatial (β=−0.67, t(48)=−6.42, p<0.001), speeded attention (β=−0.42, t (48)=−3.24, p=0.002) and executive/intellectual functions (β=−0.23, t(48) =−2.15, p=0.036). For the computerised tests, these included response speed (β=−0.47, t(46) =−3.64, p=0.001) and inhibitory control (β=−0.51, t(46) =−4.05, p<0.001). For psychosocial questionnaires, younger age was related to item endorsement on the psychiatric factor (β=−0.31, t(47) =−2.49, p=0.016). None of the Age × Group interactions were significant.
Considering the effects of concussion within alumni, executive/intellectual functioning from the neuropsychological battery was significantly associated with the number of concussions after accounting for variance due to age (β's=−0.55 and −0.39, t's (30)=−3.04, p=0.005 and −2.16, p=0.039 for concussion and age, respectively). No association was found between concussion history and performance for any of the other measures.
We examined the association of apolipoprotein ε4 status on the neuropsychological, computerised and psychosocial factors in exploratory analyses. Apolipoprotein ε4 status was not significantly associated with performance on neuropsychological or computerised test performance. There was a significant effect of ε4 status on the psychosocial measures, F(1, 30)=4.76, p=0.037, η2=0.137, with follow-up tests significant for the psychiatric factor, F(1, 30)=7.73, p=0.009, η2=0.205, but not the self-report or informant-report factors. The lack of association between apolipoprotein ε4 status and cognition could not be accounted for by low power; as seen in online supplementary figure S1, there were minimal differences between those with and without an ε4 allele. Indeed, exploratory probing indicated that those with an apolipoprotein ε4 allele had higher test performance than those without on the executive/intellectual functioning factor of the neuropsychological test battery, F(1, 30)=4.82, p=0.036, η2=0.138.
supplementary figure
Discussion
Participation in high-level contact sports is associated with later cognitive impairments and the development of earlier onset of dementia,8 ,16 ,20 especially CTE.12 ,33 Considering that most of these studies concern postmortem samples, there is a need for comprehensive neurobehavioural characterisation of former professional athletes from contact sports during life. Such studies have shown evidence in support of cognitive impairment above that expected with ageing alone8–10 ,18 (but see Casson et al)11 and, more consistently, neuropsychiatric symptoms.10 ,11 ,22 ,34 ,35 This research has included studies based on survey methods, limited batteries and no control groups. Furthermore, it has focused on boxing and football; the extent to which these results generalise to other contact sports is unknown.
We administered neuropsychological tests, computerised cognitive tests and questionnaires assessing psychosocial function in a sample of retired professional hockey players and age-matched comparison participants as part of a larger study on brain function and behaviour. Considering performance measures, there was little evidence of cognitive impairment in alumni athletes; their performance on neuropsychological and computerised tests of memory, attention, response speed and visuospatial functioning could not be differentiated from that of comparison participants. One exception was a composite measure of executive/intellectual function, where the alumni group's performance was lower than that of the comparison group. There was no evidence that these group differences were accentuated with advanced age, but concussion history was inversely related to performance on executive/intellectual function measures.
There were marked differences between alumni and comparison participants observed for measures of psychological distress and cognitive complaints. This finding is consistent with psychopathology, as identified in this alumni athlete sample by the structured clinical interview (ie, the SCID for DSM-IV diagnosis), and it was apparent for self-reported cognitive changes as well as psychiatric complaints. This suggests that measures of self-reported cognitive, social and emotional impairment are more sensitive to group differences as assessed here than is objective cognitive testing.
The effects on psychosocial measures held regardless of age and concussion history, and were supported by informants’ endorsement on measures of executive dysfunction, apathy, arousal and physical dependency. Although psychosocial impairments, including depression, anxiety, impulsivity and disinhibition, are characteristic of TBI4 and other forms of neurodegenerative diseases such as CTE, AD and behavioural variant FTD,33 ,36 our data alone cannot speak to causation. Thus, we cannot determine if the greater endorsement of psychosocial changes was due to injuries sustained as a professional athlete versus other unique elements of this sample, such as the stress associated with high-level athletic performance and retirement from professional sports.37
The presence of an apolipoprotein ε4 allele is a risk factor for neurodegenerative disease23 and cognitive impairment following TBI,22 ,25 although the incidence of ε4 was not elevated in the largest neuropathological series of CTE cases.38 The incidence of the ε4 allele in the alumni group was 28%, consistent with expectation based on the population incidence of ε4 being ∼23%.39 We found that psychiatric complaints in alumni athletes were associated with possession of the ε4 allele. While it is possible that psychiatric complaints reflect an early manifestation of concussion-related neurodegeneration33 potentiated by genetic risk, this is speculative, given the small sample size; it is equally plausible that genetic risk, concussion and other factors interact in a non-progressive manner.40 ,41 Contrary to research demonstrating an association between apolipoprotein ε4 status and cognitive impairment in TBI,22 ,23 ,25 we found that apolipoprotein ε4 carriers performed at the same level or, in the case of executive/intellectual functioning, better than those without the apolipoprotein ε4 allele, possibly reflecting antagonistic pleiotropy, whereby possession of the apolipoprotein ε4 allele is advantageous in youth and middle age and disadvantageous later in life, eg, Evans et al,42 but see Ihle et al.43 Longitudinal testing is required to determine whether such an effect will hold in this sample.
Concussion history was related to neuropsychological impairment on the executive/intellectual function factor that differentiated the groups, but not other factors. Impaired executive functioning is a hallmark feature of the post-TBI neurocognitive profile44 that has been reported in retrospective interviews by family members of individuals diagnosed with CTE33 and in retired American professional football players with head impact exposure beginning in early life.45 On the other hand, such impairment is also seen in association with psychiatric conditions such as depression.46 Therefore, non-concussion factors cannot be ruled out as contributing to this finding. Moreover, there was no evidence of memory impairment (another cardinal symptom of neurodegenerative disease) either in the alumni as a group or in relation to concussion history.
Although expected age effects were observed on most measures, we found no evidence in support of differential ageing effects in the alumni athletes relative to the comparison group. While past work assessing the long-term effects of sports-related concussion has shown accelerated age-related changes in brain structure24 (for review, see Esopenko and Levine),47 to the best of our knowledge, this has not been shown in neuropsychological or cognitive assessments.
The alumni athlete participant sample reflects those interested and available to participate in a lengthy research study and therefore is not necessarily representative of the population of alumni athletes. We acknowledge that our comparison participants were not matched to the alumni athletes for years of education. The recruitment of matched comparison participants in studies of professional athletes presents significant challenges. Many professional hockey players have lower education due to their pursuit of successful athletic careers and recruitment opportunities at a younger age than is the case for other sports. Thus, the lower education in our alumni athletes sample does not have the same meaning as it does in individuals who failed to pursue higher education due to lack of ability or interest. Indeed, our analysis of occupational status indicated that following retirement, alumni athletes and comparison participants’ occupations reflected a similar degree of cognitive engagement.
Athletes, by definition, possess a unique profile of neurocognitive and neuromuscular capacities. They are exposed to stressors and occupational characteristics that are not typical in a healthy comparison group sample. Many have experienced a number of injuries that have lasting physical and emotional effects and have greater wear and tear on their bodies from excessive and intense training, all of which are difficult to match with healthy control populations. Finally, we noted that many of our alumni participants were highly engaged, motivated and even competitive research volunteers, a profile that is not as common among comparison participants.
Another limitation of this study is the retrospective assessment of frequency and severity of concussion. Individuals may not accurately recall characteristics of remote injuries, such as post-traumatic amnesia and duration of unconsciousness. Finally, previous works have reported a high degree of substance and alcohol use in athletic populations.48 ,49 Alumni in our sample have reported a past history of alcohol and substance abuse to varying degrees, with 12% of our sample taking opiates at the time of testing. Substance abuse and psychiatric dysfunction itself cannot be ruled out as contributing to the impairments observed here, independent of concussion history.37
Although these data alone cannot speak to causation, detailed brain imaging studies in this sample will provide further information regarding the neural correlates of the observed changes. Moreover, longitudinal assessment of this sample will enable us to detect changes in function over time, if any occur. Collection of detailed behavioural and brain data across different groups of professional athletes is necessary to determine the frequency and course of cognitive and behavioural changes that may be associated with pathological ageing during life to complement the postmortem studies of dementia in athletes that have been widely reported.
Acknowledgments
This research was supported by a catalyst grant from the Canadian Institutes of Health Research (CIHR; Grant # CBT 127060), the Ontario Neurotrauma Foundation (Grant # 2012-ABI-CAT3-973), an operating grant from CIHR (Grant # MOP133728), research support from Baycrest Hospital to BL, the Women of Baycrest (TWC) and an Alzheimer's Society of Canada's Research Program Post Doctoral Fellowship awarded to CE. DJM is supported by the Canadian Institutes of Health Research. JLK is supported by a grant from the Ministry of Research and Innovation of Ontario. The authors thank Drs. Adrian Owen and Adam Hampshire for providing us with the Cambridge Brain Sciences (CBS) battery and Dr Paul Maruff for providing us with the CogState battery. Mark Napier and the NHL Alumni Association are thanked for their support in recruitment. Finally, the alumni athletes and comparison participants are thanked for volunteering their time and effort to this research.
References
Footnotes
Contributors CE and BL were responsible for study design, data collection, data analysis and manuscript preparation; TWC and MCT were responsible for neurological data collection and manuscript preparation; AB and PK were responsible for data collection and data analysis; MAB was responsible for data analysis; JLK and DJM were responsible for genetic data analyses.
Funding Canadian Institutes of Health Research Catalyst (CIHR; Grant # CBT 127060) Ontario Neurotrauma Foundation (Grant # 2012-ABI-CAT3-973) CIHR Operating Grant (Grant # MOP133728) Alzheimer’s Society of Canada’s Research Program Post Doctoral Fellowship awarded to CE.
Competing interests BL provides expert consultation on medicolegal cases involving brain injury and neurodegenerative disease, and he receives royalties for sales and training for the Goal Management Training® intervention for executive function impairments. JLK has received speaker fees from pharmaceutical companies.
Ethics approval Baycrest Health Sciences IRB.
Provenance and peer review Not commissioned; internally peer reviewed.