Article Text

Abstract
Background Genetic studies have shown that C9orf72, SOD1, TARDBP and FUS are the most common mutated genes in amyotrophic lateral sclerosis (ALS). Here, we performed a meta-analysis to determine the mutation frequencies of these major ALS-related genes in patients with ALS.
Methods We performed an extensive literature research to identify all original articles reporting frequencies of C9orf72, SOD1, TARDBP and FUS mutations in ALS. The mutation frequency and effect size of each study were combined. Possible sources of heterogeneity across studies were determined by meta-regression, sensitivity analysis and subgroup analysis.
Results 111 studies were included in the meta-analysis. The overall pooled mutation frequencies of these major ALS-related genes were 47.7% in familial amyotrophic lateral sclerosis (FALS) and 5.2% in sporadic ALS (SALS). A significant difference was identified regarding the frequencies of mutations in major ALS genes between European and Asian patients. In European populations, the most common mutations were the C9orf72 repeat expansions (FALS 33.7%, SALS 5.1%), followed by SOD1 (FALS 14.8%, SALS 1.2%), TARDBP (FALS 4.2%, SALS 0.8%) and FUS mutations (FALS 2.8%, SALS 0.3%), while in Asian populations the most common mutations were SOD1 mutations (FALS 30.0%, SALS 1.5%), followed by FUS (FALS 6.4%, SALS 0.9%), C9orf72 (FALS 2.3%, SALS 0.3%) and TARDBP (FALS 1.5%, SALS 0.2%) mutations.
Conclusions These findings demonstrated that the genetic architecture of ALS in Asian populations is distinct from that in European populations, which need to be given appropriate consideration when performing genetic testing of patients with ALS.
Statistics from Altmetric.com
Introduction
Amyotrophic lateral sclerosis (ALS) is a syndrome characterised by progressive degeneration involving the corticospinal tract, brainstem and anterior horn cells of the spinal cord. Although most cases are sporadic (SALS), ∼5–10% of patients with ALS have a positive family history (FALS) and show a Mendelian pattern of inheritance. Since 1993, more than 20 genes have been found to be implicated in the pathogenesis of ALS.1 Recent studies have shown that C9orf72, SOD1, TARDBP and FUS are the most common mutated genes in ALS in European and Asian populations; these genes are considered as major ALS-related genes.2–7 However, the mutation frequencies varied dramatically across studies. Systematic reviews and meta-analyses are powerful tools in neuroepidemiology, by integrating and evaluating the wealth of primary research.8 Until now, no meta-analysis has been performed to determine the mutation frequencies of these major ALS-related genes in patients with ALS. Here, we performed a systematic review and meta-analysis of genetic studies screening mutations in these major ALS-related genes to determine the genetic epidemiology of ALS.
Methods
We applied the guidelines for Meta-Analyses and Systematic Reviews of Observational Studies (MOOSE).9
Systematic search
MEDLINE and EMBASE were searched to identify all published studies reporting mutation frequencies of the C9orf72, SOD1, TARDBP or FUS gene in patients with ALS before 30 April 2016. The individual search terms ‘Cu/Zn superoxide dismutase’, ‘SOD1’, ‘chromosome 9 open reading frame 72’, ‘C9orf72’, ‘TAR DNA binding protein’, ‘TARDBP’, ‘TDP-43’, ‘fused in sarcoma’, ‘FUS’, in combination with ‘amyotrophic lateral sclerosis’ OR ‘ALS’ OR ‘motor neuron(e) disease’ OR ‘MND’ AND ‘mutation’, were used. We also searched China National Knowledge Infrastructure (CNKI) and Wangfangdata (http://www.wanfangdata.com.cn/) for studies in Chinese. Hand search of the bibliographies of the identified articles was also performed.
Eligibility criteria and data collection
All studies presenting original data that reported mutation frequencies of the C9orf72, SOD1, TARDBP or FUS gene in patients with ALS were included for further review. Only studies with full text were selected in the systematic review, while abstracts presented at relevant scientific meetings were not included. Two authors (Z-YZ and C-HC) reviewed all identified studies independently to determine whether an individual study was eligible for inclusion, according to the following criteria: (1) case–control studies or case series; (2) diagnostic criteria of ALS were clearly stated, either by clinical criteria, or El Escorial criteria/revised El Escorial criteria, Awaji criteria; (3) familial history of the patients with ALS enrolled was clear, and mutations in each gene were reported in either FALS or SALS cases; (4) all exons of SOD1 should be screened since there are no definite mutational hotspot regions in the SOD1 gene. Case reports were not included in the analysis. When the same patient population was presented in more than one publication, the one with the largest sample size or most recent publication date was used as the primary study for data extraction. Since some studies reporting TARDBP, FUS or C9orf72 mutations enrolled only non-SOD1 mutated patients with FALS, which will undoubtedly overestimate the mutation frequencies, patients with FALS in these studies were excluded from the meta-analysis. Studies that enrolled special ALS population, such as early-onset ALS, or ALS-frontotemporal dementia (FTD), were excluded from the analysis due to potential selection bias.
Data extraction
While collecting data from articles included in the meta-analysis, we did not use a ‘quality score’ to evaluate included articles as its use has been criticised for being inaccurate in some cases.8 Instead, we used a table to document all aspects of the studies that might influence the mutation frequencies (see online supplementary table S1). For each eligible publication, the following information was extracted independently by two authors (Z-YZ and C-HC): name of the first author, publication year, country of the study, population, study design, detection method, exons sequenced, sample size of FALS and/or SALS cases as well as control groups, numbers of mutation carriers in FALS and/or SALS, diagnosis criteria category of ALS, criteria of FALS. The criteria of FALS proposed by Byrne et al 10 was used: definite ALS is defined as a patient with ALS with at least two first-degree or second-degree relatives with ALS; probable FALS is defined as a patient with ALS with one first-degree or second-degree relative with ALS; possible FALS means a patient with ALS with a distant relative with ALS (more distant than first degree or second degree) or a patient with ALS with a family member with FTD. The corresponding or first authors of the studies were contacted for detailed information if needed. Disagreements between two reviewers were resolved by consensus.
Statistical analysis
In each study, the mutation frequencies of the SOD1, TARDBP, FUS or C9orf72 gene were reported as the number of the mutation carriers among all cases of FALS or SALS screened. The effect sizes and corresponding 95% CI for each study were calculated. Since the mutation frequencies were in a binomial distribution rather than a normal distribution, which makes it more likely that the errors in the estimates of frequencies are not constant between studies, arcsine transformation of the frequencies was implemented to stabilise variances and normalise proportional data. Statistical heterogeneity among studies was evaluated using Cochrane's Q test (significance set at p<0.10) and I2 statistics. If I2<50%, then the studies were considered to be homogeneous, and the mutation frequencies were combined using a fixed-effects model. Otherwise, I2≥50% or p for Q test <0.10, indicating substantial heterogeneity across studies and a random-effects model was used.
To determine possible sources of heterogeneity, univariate and multivariate meta-regression analyses were adopted to assess the following demographic and clinical variables: population, study design, detection method, and selected screening or not. To assess the impact of each study on the overall result, sensitivity analysis was conducted. Subgroup analysis according to population (European or Asian) and study design (hospital-based study or population-based study) was further performed to find explanations for substantial heterogeneity across studies. Publication bias was assessed graphically using funnel plots and linear regression tests according to Egger's test. The p value <0.05 was considered statistically significant.
Statistical analysis was carried out using the Meta function of R (R Core Team (2016). R: A language and environment for statistical computing. R Foundation for Statistical Computing, Vienna, Austria. URL https://http://www.R-project.org/).
Results
Systematic review
In total, 6288 articles were identified and 2275 duplicate articles were removed. Then 3853 additional articles were excluded due to the incorrect type of studies (animal studies, in vitro studies, clinical trials) and type of articles (eg, conference proceedings, review, editorials). We retrieved 178 genetic studies providing original information on SOD1, TARDBP, FUS and C9orf72 mutations in patients with ALS. Sixty-seven articles were excluded for not meeting the inclusion criteria after depth review (see online supplementary table S1). Thus, 111 articles were included in the final analysis. In 13 studies reporting TARDBP mutations and 2 studies reporting FUS mutations, FALS were deleted from the analysis because SOD1 mutated FALS were excluded (see online supplementary table S2). A flow diagram of the literature that was searched and evaluated is presented in online supplementary figure S1.
supplementary table
Study characteristics articles included in meta-analysis
supplementary figure
Flow chart eligibility criteria of articles included in meta-analysis.
Of the 111 studies analysed, 81 enrolled patients with ALS of European origin and 30 enrolled patients of Asian origin. One hundred and five studies were hospital based and six studies were population based (see online supplementary table S2). In 7 studies, ALS was diagnosed with clinical criteria, 10 studies used E1 Escorial criteria, 92 studies used E1 Escorial revised criteria and only 2 studies used Awaji criteria. Patients with definite/probable ALS were analysed in 52 studies and patients had definite/probable/possible ALS in 11 studies. Eleven studies enrolled probable FALS and 35 studies enrolled possible FALS, while 32 studies did not clearly state the definition of FALS. Gene by gene Sanger sequencing was used in 105 studies and next generation sequencing was used in 6 studies. SOD1 mutations and C9orf72 repeat expansions in patients with ALS were reported in 53 and 40 studies, respectively. Forty-six studies screened for TARDBP mutations, including eight studies screening only exon 6 of the TARDBP gene. Thirty-four studies reported FUS mutations, including 13 studies screening only exons of mutational hotspot regions (see online supplementary table S2).
Meta-analysis
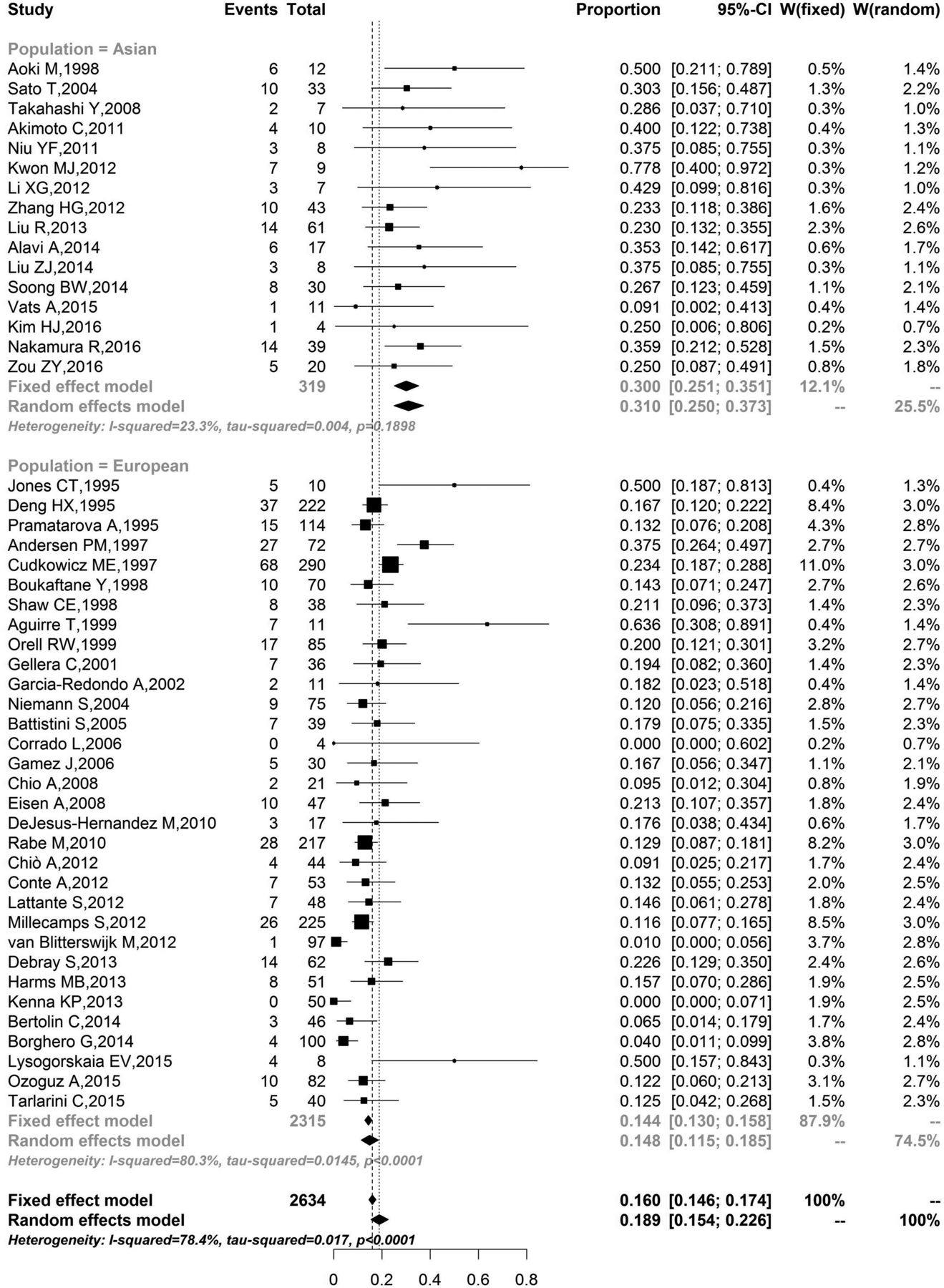
Forty-eight and 36 studies reported the frequency of SOD1 mutations in 2634 patients with FALS and 7811 patients with SALS, respectively. In pooled analysis, the frequency of SOD1 mutations was 18.9% (95% CI 15.4% to 22.6%) in patients with FALS and 1.2% (95% CI 0.8% to 1.8%) in patients with SALS (table 1). Twenty-six and 40 studies reported the frequency of TARDBP mutations in 1267 patients with FALS and 10 681 patients with SALS, respectively. In pooled analysis, 3.3% (95% CI 1.4% to 6.0%) of patients with FALS and 0.5% (95% CI 0.2% to 0.9%) of patients with SALS harboured TARDBP mutations (table 1). Twenty-nine and 26 studies reported the frequency of FUS mutations in 2107 patients with FALS and 10 877 patients with SALS, respectively. In pooled analysis, the frequency of FUS mutations was 3.0% (95% CI 2.3% to 3.8%) in patients with FALS and 0.4% (95% CI 0.2% to 0.6%) in patients with SALS (table 1). Thirty-three and 36 studies reported the frequency of C9orf72 repeat expansions in 2630 patients with FALS and 18 175 patients with SALS, respectively. In pooled analysis, 22.5% (95% CI 17.1% to 28.3%) of patients with FALS and 3.1% (95% CI 2.1% to 4.2%) of patients with SALS harboured C9orf72 repeat expansions (table 1). The individual mutation rates of these genes in FALS, as well as frequencies of SOD1 and C9orf72 mutation in SALS for each country, were plotted on a map to determine a possible geographic pattern (see online supplementary figures S2–S5).
Pooled mutated rate, heterogeneity statistics and linear regression test of funnel plot asymmetry of major ALS-related genes
Heterogeneity
Substantial heterogeneity (I2: 44–95%, all p<0.01) existed in studies screening SOD1, TARDBP, FUS and C9orf72 mutations in either FALS or SALS cases (table 1).
Sensitivity analysis
Regarding the studies reporting TARDBP mutations, sensitivity analysis revealed that when the study by Borghero et al 11 was omitted, the heterogeneity greatly reduced in studies either in patients with FALS (I2 reduced to 48%) or patients with SALS (I2 reduced to 67%), suggesting that this study may cause the instability of the results.
Meta-regression
The univariate and multivariate meta-regression analyses demonstrated a significant association between population and SOD1 mutations (p<0.0001), study design and SOD1 mutations in FALS (p<0.01). A significant association between population and C9orf72 mutation in patients with either FALS or SALS (both p<0.0001), as well as a significant association between population and FUS mutation in FALS (p<0.05), was also detected (table 2). We did not identify any heterogeneity in mutation frequencies in relation to the sequencing method (all p>0.05; table 2). Neither did any heterogeneity exist in frequencies of TARDBP or FUS mutation in relation to selective sequencing or not (all p>0.05; table 2).
Univariate and multivariate meta-regression analyses of potential sources of heterogeneity in the mutation rate of major ALS-related genes
Subgroup analysis
In European populations, the pooled mutation rate in FALS was 14.8% (11.5% to 18.5%) for SOD1 mutations, 4.2% (1.6% to 7.8%) for TARDBP mutations, 2.8% (2.1% to 3.5%) for FUS mutations and 33.7% (29.3% to 38.2%) for C9orf72 repeat expansions, while the pooled mutation frequency in SALS was 1.2% (0.7% to 1.9%) for SOD1 mutations, 0.8% (0.2% to 1.5%) for TARDBP mutations, 0.3% (0.1% to 0.5%) for FUS mutations and 5.1% (4.3% to 6.0%) for C9orf72 repeat expansions (table 3, figures 1 ⇓ ⇓–4, online supplementary figures S6–S9). In Asian populations, the pooled mutation rate in FALS was 30.0% (25.1% to 35.1%) for SOD1 mutations, 1.5% (0% to 6.0%) for TARDBP mutations, 6.4% (3.2% to 10.5%) for FUS mutations and 2.3% (0.3% to 6.3%) for C9orf72 repeat expansions, while the pooled mutation frequency in SALS was 1.5% (1.0% to 2.0%) for SOD1 mutations, 0.2% (0% to 0.3%) for TARDBP mutations, 0.9% (0.2% to 1.9%) for FUS mutations and 0.3% (0.1% to 0.6%) for C9orf72 repeat expansions (table 3, figures 1 ⇓ ⇓–4, online supplementary figures S6–S9).
Subgroup analysis of frequencies according to population and study design in patients with ALS with major ALS-related mutation
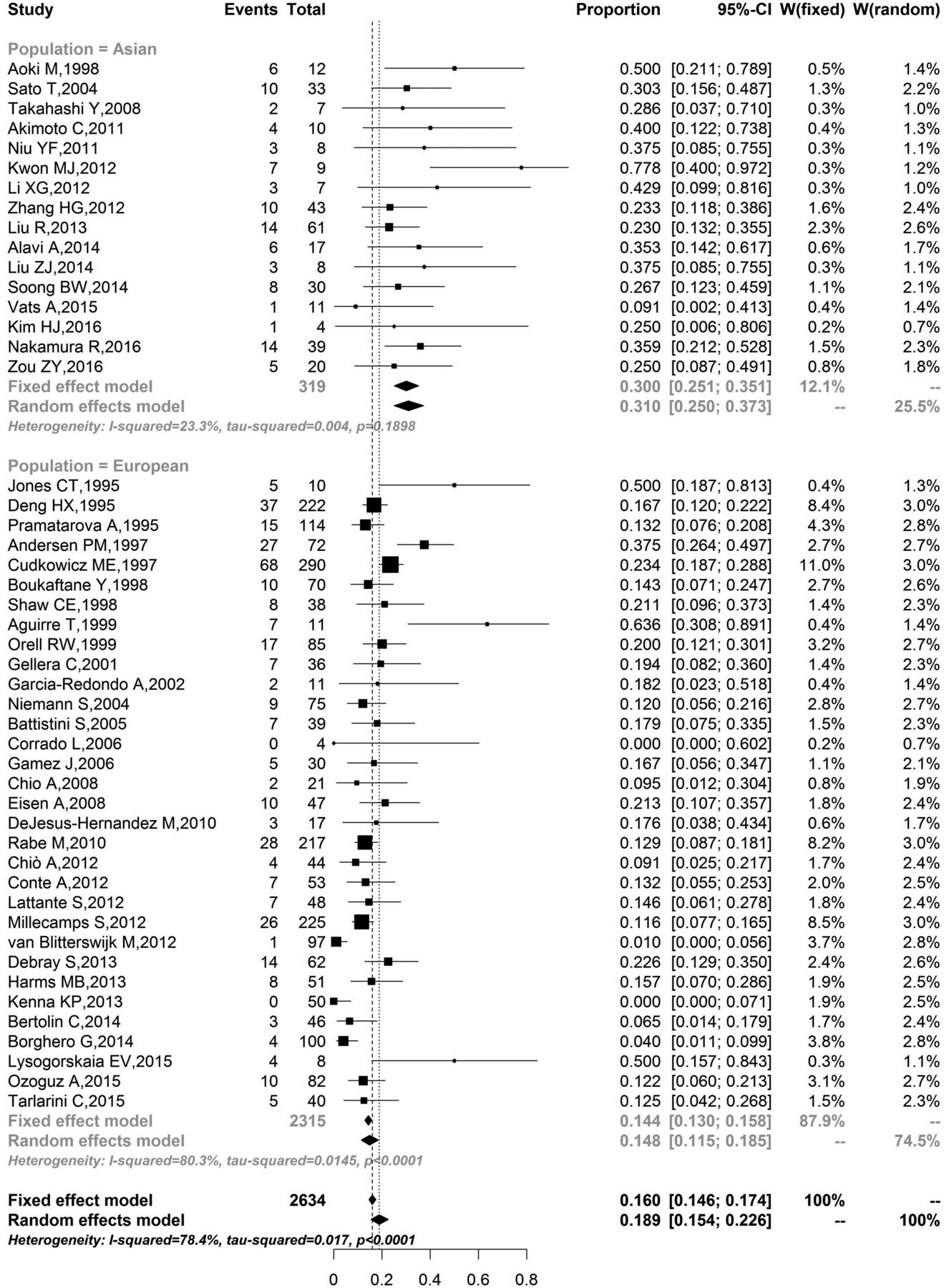
Forest plot of studies reporting SOD1 mutations in FALS in European and Asian populations. FALS, familial amyotrophic lateral sclerosis.

Forest plot of studies reporting TARDBP mutations in FALS in European and Asian populations. FALS, familial amyotrophic lateral sclerosis.

Forest plot of studies reporting FUS mutations in FALS in European and Asian populations. FALS, familial amyotrophic lateral sclerosis.

Forest plot of studies reporting C9orf72 mutations in FALS in European and Asian populations. FALS, familial amyotrophic lateral sclerosis.
Studies with European populations had more C9orf72 mutations in either FALS or SALS (both p<0.0001), more TARDBP mutations in SALS cases (p<0.05) than those with Asian populations, while studies with Asian populations had more SOD1 and FUS mutations in FALS than those with European populations (p<0.0001, p=0.02, respectively; table 3).
In hospital-based studies, the pooled mutation rate in FALS was 20.2% (17.1% to 23.6%) for SOD1 mutations, 3.3% (1.2% to 6.5%) for TARDBP mutations, 3.1% (2.4% to 3.9%) for FUS mutations and 20.0% (14.4% to 26.3%) for C9orf72 repeat expansions, while the pooled mutation frequency in SALS was 1.3% (0.8% to 2.0%) for SOD1 mutations, 0.5% (0.1% to 1.0%) for TARDBP mutations, 0.4% (0.2% to 0.7%) for FUS mutations and 2.9% (1.9% to 4.1%) for C9orf72 repeat expansions (table 3 and figures 1 ⇑ ⇑–4, online supplementary figures S6–S9). In population-based studies, the pooled mutation rate in FALS was 6.9% (0.6% to 19.2%) for SOD1 mutations, 2.7% (0% to 10.5%) for TARDBP mutations, 1.8% (0% to 7.1%) for FUS mutations and 39.6% (30.3% to 48.9%) for C9orf72 repeat expansions, while the pooled mutation frequency in SALS was 0.8% (0.1% to 2.2%) for SOD1 mutations, 0.6% (0.2% to 1.1%) for TARDBP mutations, 0.2% (0% to 0.6%) for FUS mutations and 4.6% (2.7% to 7.0%) C9orf72 repeat expansions (table 3 and figures 1 ⇑ ⇑–4, online supplementary figures S6–S9). Hospital-based studies had more SOD1 mutations but less C9orf72 mutations in FALS than population-based studies (p<0.001, p<0.05, respectively; table 3).
Publication bias
Significant funnel plot asymmetry was found in studies reporting SOD1 mutations in patients with FALS (p<0.05) and studies reporting C9orf72 mutations in FALS (p<0.01) or SALS (p=0.05; table 1). Since funnel plot asymmetry can be caused by publication bias, smaller studies with poor methodological quality as well as true heterogeneity and contour-enhanced funnel plots were made to differentiate asymmetry due to publication bias from that due to other factors (see online supplementary figure S10).12 Regarding studies reporting SOD1 mutations in FALS, publication bias, together with true heterogeneity, is the underlying cause of this funnel asymmetry (see online supplementary figure S10A). Regarding studies reporting C9orf72 mutations in patients with FALS and SALS, true heterogeneity rather than publication bias is the underlying cause of this funnel asymmetry (see online supplementary figures S10B and S10C).
Discussion
In this study, we performed a meta-analysis combining data from all eligible studies to determine the mutation frequencies of major ALS-related genes in ALS. Our analysis showed that the overall pooled mutation frequencies of these major ALS-related genes is 47.7% in FALS (C9orf72 22.5%, SOD1 18.9%, TARDBP 3.3%, FUS 3.0%) and 5.2% in SALS (C9orf72 3.1%, SOD1 1.2%, TARDBP 0.5%, FUS 0.4%). The frequencies of SOD1, C9orf72 and FUS mutations are lower than the previous estimates of the mutation rate (FALS 34.2%, SALS 5.9% for C9orf72 repeat expansions;13 FALS 20.7%, SALS 2.2% for SOD1 mutations;14 FALS 5%, SALS 1% for FUS mutations15), while the frequency of TARDBP mutations is in accordance with a previous estimate of the mutation rate of this gene (FALS 3%, SALS 1.2%).15
Interestingly, 16 patients with FALS and 2 patients with SALS harbouring double mutations have been identified in 5 out of 17 studies screening these four genes.2–7 ,11 ,16–25 Fifteen patients harboured C9orf72 repeated expansion in combination with the SOD1, TARDBP or FUS mutation,4 ,11 ,16–18 while three patients had double mutations in the TARDBP gene.4 ,11 Statistical analysis demonstrated that the frequency of double mutations in FALS is 0.4% (0% to 1.4%), which is higher than expected on the basis of chance (p=1.57×10−7), suggesting an oligogenic basis of ALS.17
Sensitivity analysis revealed that the study by Borghero et al 11 may cause the instability of the pooled frequencies of TARDBP mutations in FALS and SALS. Prior studies have identified the p.A382T mutation in the TARDBP gene as a founder mutation, which is highly prevalent in patients with ALS (39–80% FALS and 9–23% SALS) from Sardinia, a genetically isolated Mediterranean island.26 ,27 The mutation frequency for p.A382T is 25.0% in FALS and 19.3% in SALS in the Sardinia cohort by Borghero et al,11 much higher than the frequency of TARDBP mutations in other studies. Therefore, the founder effect of the p.A382T mutation in Sardinia in the study by Borghero et al may be the source of heterogeneity in studies reporting TARDBP mutations in patients with ALS.
Meta-regression analysis demonstrated a significant association between population and the C9orf72 mutation in FALS and SALS, as well as a SOD1 and FUS mutation in patients with FALS (table 2). The results suggest that population may be an important cause of heterogeneity across the studies. Subgroup analysis also showed that studies with European populations had more C9orf72 mutations in FALS and SALS, more TARDBP mutation in SALS than those with Asian populations, while studies with Asian populations had more SOD1 and FUS mutations in FALS than those with European populations (table 3). Our findings verified the distinct genetic architecture between European and Asian ALS populations.7 ,28
In European populations, the most common mutations in ALS were the C9orf72 repeat expansions (FALS 33.7%, SALS 5.1%), followed by SOD1 (FALS 14.8%, SALS 1.2%), TARDBP (FALS 4.2%, SALS 0.8%) and FUS mutations (FALS 2.8%, SALS 0.3%; table 1 and figure 5). Frequency of C9orf72 mutation in FALS is highest in Belgium and Greek (both 50.0%), followed by Finnish (46.4%); frequency of C9orf72 mutation in SALS is highest in Finnish (21.1%), followed by Greek (8.1%) and French (7.9%; see online supplementary figure S5). Prior studies have shown that most patients with C9orf72 repeat expansions in Asian populations had the same risk haplotype29–34 commonly shared by European mutation carriers,35 suggesting a common founder effect that spread from Europe to East Asia in human migration history.36

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Genetic architecture of FALS and SALS in European and Asian populations. FALS, familial amyotrophic lateral sclerosis; SALS, sporadic amyotrophic lateral sclerosis.
On the other hand, in Asian populations, the most common mutations in ALS were the SOD1 mutations (FALS 30.0%, SALS 1.5%), followed by FUS (FALS 6.4%, SALS 0.9%), C9orf72 repeat expansions (FALS 2.3%, SALS 0.3%) and TARDBP mutations (FALS 1.5%, SALS 0.2%; table 1 and figure 5). Frequency of the SOD1 mutation in FALS is highest in Koreans (54.7%), followed by Russians (50.0%) and Finnish (42.9%); frequency of SOD1 mutation in SALS is highest in Finnish (11.3%), followed by Russians (3.5%) and Iranians (3.3%; see online supplementary figure S2). Our study suggests a slight North–South gradient in the frequency of the SOD1 mutation across Europe (42.9% in Finland and 35.6% in Sweden, 24.4% in the UK, 11.6% in France, and 12.3% in Italy) as previously reported (see online supplementary figure S2).37 Interestingly, there also seems to be a North–South gradient in the frequency of the SOD1 mutation across Asia, with a higher mutation rate in Koreans (54.8%), Japanese (35.5%), Iranians (35.3%), Chinese (25.9%) and lower mutation rate in Indians (9.1%; see online supplementary figure S2).
The results highlighted important lessons regarding mutation screening in ALS of different ethnic backgrounds. In European patients with ALS, C9orf72 repeat expansions should be screened first, followed by SOD1 mutations, and then TARDBP and FUS mutations, while in Asian patients with ALS, SOD1 mutations should be screened first, followed by FUS mutations, and then C9orf72 and TARDBP mutations.
Meta-regression analysis demonstrated a significant association between study design and SOD1 mutation in FALS. Subgroup analysis showed that hospital-based studies had more SOD1 mutations but less C9orf72 mutations in FALS than population-based studies. Population-based studies include all patients in a defined geographic area in a given period of time, while hospital-based studies are supposed to be biased towards the inclusion of younger patients who are more likely to carry a genetic mutation.38 Since all of the population-based studies included in the meta-analysis were carried out in a European population,3 ,4 ,17 ,38–40 the population-based frequency of 6.9% (0.6% to 19.2%) for SOD1 mutations, 2.7% (0% to 10.5%) for TARDBP mutations, 1.8% (0% to 7.1%) for FUS mutations, and 39.6% (30.3% to 48.9%) for C9orf72 repeat expansions in FALS, 0.8% (0.1% to 2.2%) for SOD1 mutations, 0.6% (0.2% to 1.1%) for TARDBP mutations, 0.2% (0% to 0.6%) for FUS mutations and 4.6% (2.7% to 7.0%) for C9orf72 repeat expansions in SALS is likely to represent the most accurate estimation of mutation rate of ALS in European populations.
There were several limitations in this meta-analysis. First of all, regarding the studies reporting TARDBP and FUS mutations, selective detection of exons in mutational hotspot regions in some studies might underestimate the frequencies of TARDBP and FUS mutations. However, 47 out of 48 TARDBP mutations reported so far were located in exon 6 (see online supplementary figure S11), while 43 out of 68 FUS mutations reported so far were located in exons 14 and 15 (see online supplementary figure S12).41 No significant difference was found in subgroup analysis according to selective detection or not (data not shown), suggesting that selective detection of exons in mutational hotspot regions in TARDBP and FUS could represent the mutation frequencies of both genes. Second, since there is no consensus on a standard definition for FALS,42 ,43 different criteria of FALS were used in the studies included, which might influence the accurate comparison of mutation frequencies of these genes in FALS across different populations. It has been shown that probable patients with FALS had more mutations in major ALS-related genes than possible ALS.19 Unfortunately, owing to the fact that 40% of the studies included did not state how they defined FALS, subgroup analysis according to the criteria of FALS was not carried out. Third, different diagnostic criteria of ALS were used in the studies included. Although most studies included definite/probable ALS according to El Escorial criteria/revised El Escorial criteria, some studies also enrolled possible/suspect ALS according to El Escorial criteria/revised El Escorial criteria, as well as ALS diagnosed with clinical criteria. Since some studies did not clearly state the diagnostic category of ALS, subgroup analysis according to diagnostic categories of ALS was not performed and the real impact of the methodological differences is difficult to estimate. Fourth, publication bias may exist in studies reporting SOD1 mutations.
In conclusion, our findings emphasise the distinct genetic architecture between European and Asian ALS populations, which need to be given appropriate consideration when performing genetic testing of patients with ALS. Careful prospective population-based studies using valid criteria of FALS should be carried out in different populations, especially Asian populations, to determine more precise mutation frequencies of major ALS-related genes.
Acknowledgments
The authors thank Professor Zheng Lin from the Department of Epidemiology and Health Statistics, Fujian Medical University, and Professor Tiansong Zhang from Jing'an District Central Hospital of Shanghai for the help in statistical analysis of this study. The authors also thank the anonymous reviewers for their helpful suggestions on the quality improvement of our report.
References
Footnotes
Contributors Z-YZ was involved in the study concept, literature search, data extraction, analysis and interpretation of the data, statistical analysis, and drafting/revising the manuscript. Z-RZ and C-HC were involved in the literature search, data extraction, analysis and interpretation of the data and revising the manuscript. C-YL, R-LH were involved in the analysis and interpretation of the data and revising the manuscript. H-PH was involved in the analysis and interpretation of the data, as well as in revising the manuscript and study coordination.
Funding This study was supported by the National Science Foundation of Fujian (2015J01395) and National Natural Science Foundation of China (grant number 81671271).
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- Editorial commentary