Article Text

Abstract
Importance Chronic, intractable neuropathic pain is a common and debilitating consequence of neuromyelitis optica spectrum disorder (NMOSD) myelitis, with no satisfactory treatment; few studies have yet to explore its aetiology.
Objective To establish if myelitis-associated chronic pain in NMOSD is related to the craniocaudal location of spinal cord lesions.
Method (1) Retrospective cohort of 76 aquaporin 4-antibody (AQP4-Ab)-positive patients from Oxford and Liverpool's national NMOSD clinics, assessing current pain and craniocaudal location of cord lesion contemporary to pain onset. (2) Focused prospective study of 26 AQP4-Ab-positive Oxford patients, a subset of the retrospective cohort, assessing current craniocaudal lesion location and current pain.
Results Patients with isolated thoracic cord myelitis at the time of pain onset were significantly more disabled and suffered more pain. Cervical and thoracic lesions that persisted from pain onset to ‘out of relapse’ follow-up (current MRI) had highly significant (p<0.01) opposing effects on pain scores (std. β=−0.46 and 0.48, respectively). Lesion length, total lesion burden and number of transverse myelitis relapses did not correlate with pain.
Conclusions Persistent, caudally located (ie, thoracic) cord lesions in AQP4-Ab-positive patients associate with high postmyelitis chronic pain scores, irrespective of number of myelitis relapses, lesion length and lesion burden. Although disability correlated with pain in isolation, it became an insignificant predictor of pain when analysed alongside craniocaudal location of lesions.
Statistics from Altmetric.com
Introduction
Neuromyelitis optica spectrum disorder (NMOSD) is a relapsing inflammatory central nervous system disorder preferentially involving the optic nerve and spinal cord, the latter typified by longitudinally extensive transverse myelitis (TM). Chronic neuropathic pain is a common and disabling consequence of NMOSD myelitis and is often refractory to treatment.1 The mechanism of myelitis pain is not fully understood, and may vary across the different neurogenic types reported, all of which may be present in a single patient. These include ‘hug-like’ pain at the level of TM, and dysaesthesias and painful tonic muscle spasms below the TM level.2
In contrast, pain in multiple sclerosis (MS) myelitis is less prevalent and less severe.3 Known differences in NMOSD and MS cord lesions potentially provide insights into this disparity and the observation that MS lesions predominantly involve the cervical cord, whereas NMOSD lesions are frequently thoracic4 might be a contributor, particularly as a recent paper implicated thoracic cord lesions in the aetiology of MS chronic pain.5
Here, we investigate whether the craniocaudal location of spinal cord lesions influences pain in NMOSD TM, first in a retrospective cohort and then in a prospective subgroup.
Methods
Subjects
Seventy-six aquaporin 4-antibody (AQP4-Ab)-positive patients from Oxford and Liverpool's national NMOSD Clinics consented to the use of their demographic, clinical and imaging data (Oxfordshire REC 07/Q1604/28; London-Hampstead REC 15/L01433). An n=26 subset consented to be studied prospectively (Berkshire REC 13/SC/0238). AQP4-Ab tests were performed by cell-based assay.6
Study assessments
All subjects were selected to have had at least one attack of TM, with MRI available at the attack related to pain onset. Spinal segments with T2-weighted hyperintensities at the time of the TM attack associated with pain onset were recorded (the selection was performed by a clinician at each centre; GT and SH).
Current pain was assessed at the time of the study by the Brief Pain Inventory's (BPI) Pain Severity Index (PSI, 0–40). The PSI consists of four components separately rated between 0, no pain, to 10, worst pain imaginable, these are: pain on average, pain ‘now’, maximal pain in the last 24 hours and minimal pain in the last 24 hours; the score thus captures pain severities ranging from trivial to very severe.7 Patients were requested to score the pain related to their myelitis rather than non-myelitis pain problems (eg, migraine, joint pain, etc), focusing on non-spasm-related pain. The type of pain was confirmed ‘neuropathic’ in line with the International Association for the Study of Pain (IASP) definitions.8 All subjects also had current documented physical disability ratings in the form of an European Database for MUltiple Sclerosis (EDMUS) score, an integer ambulation-dominant score equivalent to the Expanded Disability Status Scale (EDSS).9 ,10 We confirmed that no subject had clinically detectable or diagnosed peripheral neuropathy.
Prospective imaging
Participants in the prospective subset underwent additional imaging at the time of recruitment: T1-weighted three-dimensional isotropic MRIs of the whole cord (MP-RAGE: TR: 2.3 s, TE: 3.9 ms, flip angle 8o, voxel 1.0×1.0×0.9 mm) and T2-weighted sagittal and axial MRIs of the cervical cord, and sagittal MRIs of the thoracolumbar cord (T2 TSE: sagittal whole cord: TR: 4.6 s, TE: 68 ms, voxel=0.7×0.7×3.0 mm; axial cervical cord: TR=9.17, TE=70, voxel=0.6×0.6×4 mm). Scans were performed on a 3T Siemens MAGNETOM Verio. Prospective MRIs were performed outside of relapse during remission.
T2 hyperintense lesion locations were identified by a clinical researcher (GT) and validated by a blinded clinical neurologist (MJ). Prescribed antineuropathic medications were recorded.
Analyses and statistics
All statistical analyses were performed using R (http://www.r-project.org).
Subjects were grouped by gross location of TM (isolated cervical, isolated thoracic or cervicothoracic) and additionally the lesions midpoint was noted (eg, a lesion from C3 to C7 gives a C5 midpoint; for two lesions, a C5–6 and a T1–2 gives a C7 midpoint). The lesions midpoint is mathematically the lesion load ‘centre of mass’ and provided a helpful univariate measure in carefully selected correlations and regression models; it does not encapsulate the extent or distribution of the lesion/s. Clinical features were compared across groups using χ2 for sex and analysis of variance (ANOVA) with post hoc Tukey's honest significance test11 (Tukey HST) for continuous data. Data included in parametric testing were assessed normally distributed by the Shapiro-Wilk test.12
Pearson's r was calculated for pain versus number of attacks, disease duration, length of longest lesion and total TM lesion burden; variables we considered likely predictors of pain. Additional correlations between pain and persistent lesions midpoint and number of antineuropathic medications were performed on the prospective subset.
Predictors of pain (PSI) were assessed using multiple regression with independent variables: current age, age at disease onset, EDMUS, thoracic (y/n) and cervical (y/n) lesion location (lesion length, etc, were not included having shown no correlation).
Results
Of the 76 patients, 66 were women, reflecting the recognised female predominance of NMOSD. Mean age was 55 years, and mean disease duration 10.4 years. Patients had a median EDMUS of 5 at the time of pain assessment (range 0–9) (table 1).
Clinical variables of retrospective study according to transverse myelitis (TM) location
All patients were on long-term immunosuppressive treatments (IST): 20/26 (77%) on prednisolone, of whom 18 were on prednisolone plus another IST. Other ISTs included azathioprine (12/26), methotrexate (5/26), mycophenolate (4/26) and rituximab (3/26).
Eleven patients had no pain; for these the latest TM-associated MRI was used. Only one of the 11 had an isolated thoracic lesion. Five of the 11 had >1 attack of TM, only two of whom had attacks of TM in cervical and thoracic regions at different times; in both instances the selected MRI showed cervicothoracic lesions. Two patients had a previous cervical TM without pain and then developed pain after a subsequent thoracic TM attack, but no patients with thoracic myelitis at onset without pain developed pain with a subsequent cervical myelitis. For all subjects with pain, the pain was anatomically attributable to a TM lesion. Most suffered multiple neuropathic pain characteristics included circumferential thoracic bands of dysaesthesia (colloquially termed the myelitis ‘hug’), dysaesthesias of the limbs, especially the legs (burning, pins and needles, etc), areas of allodynia and patches of hyperalgesia. Painful spasms, though typical in recovering NMO myelitis, were infrequently reported in this stable population of patients.
Within the 76 patients analysed, TM onset attack lesions affected the cervical and thoracic cord in 54% (41/76), were limited to the cervical cord in 21% (16/76) and to thoracic segments in 25% (19/76). Sixty-five patients (86%) suffered on-going pain, with more than a fifth (21%) suffering pain equivalent to 7–10 on a 0–10 scale (10 rated as ‘worst pain imaginable’). Pain was most commonly felt in the trunk (akin to the myelitis ‘hug’), and in the limbs, especially distally and with a predilection for the legs (see e-figure 1). Mean duration of chronic pain was 6 years (SD 4.2). More than 50% of patients with chronic pain developed pain associated with their first TM attack.
supplementary data
Their clinical profile according to TM location is shown in table 1.
Patients with isolated cervical, isolated thoracic or cervical plus thoracic myelitis did not differ for sex, disease duration, number of attacks or number of TM episodes. However, patients with isolated thoracic TM were more disabled and older at the time of study and at disease onset (table 1).
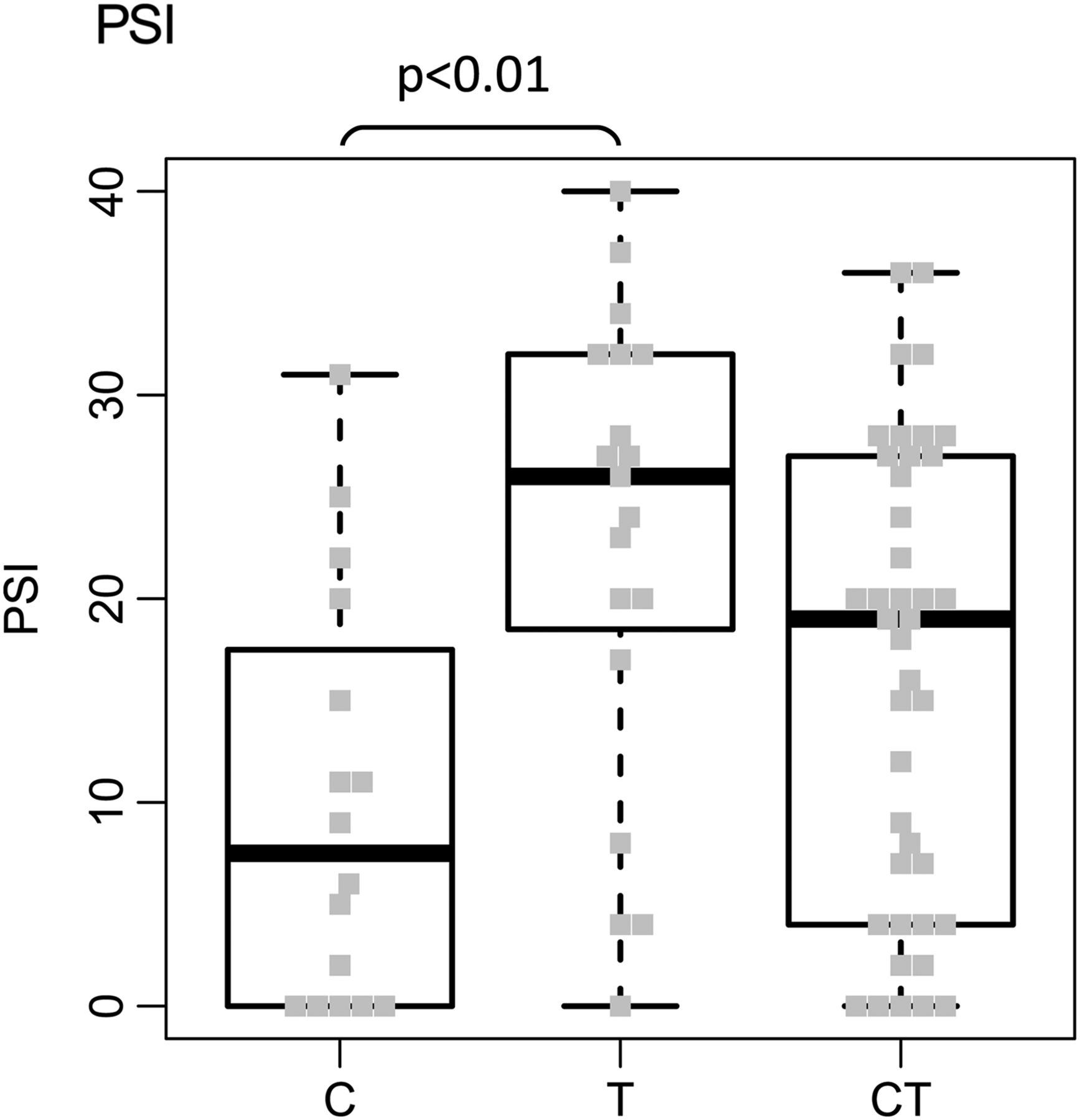
Pain scores (PSI) were significantly greater in patients with isolated thoracic lesions than in those with isolated cervical lesions (table 1 and figure 1).

PSI score distribution according to pain-onset transverse myelitis (TM) location (whole cohort, n=76). Boxplot figure calculated using first and third quartile, and median. C, isolated cervical; CT, cervicothoracic; PSI, Pain Severity Index; T, isolated thoracic.
Pain (as assessed by PSI) did not correlate with number of TM attacks, disease duration, length of longest TM lesion or total TM lesion burden. There was no significant difference in mean number of TM attacks between those with and without pain.
As the isolated thoracic lesion group in addition to suffering greater pain was also older with greater disability, we performed a multivariate analysis including these variables with PSI as the dependent variable. The regression model described 19% of PSI variance (adjusted r2 0.19; p<0.01). The only significant independent predictor of PSI was EDMUS (p<0.05). Thoracic lesions had a trend towards a positive contribution (p=0.09), with an opposing negative effect seen for cervical lesions (ns) (data not shown). Using the same model with the lesions midpoint explained 22% of the PSI variance (r2=0.22; p<0.05) and found EDMUS and lesions midpoint to be significant independent predictors of PSI (p<0.05 and p<0.01, respectively), with standardised β coefficients of 0.33 and 0.29 (data not shown).
Prospective subset
Of the 76 patients, 26 consented to have a current spinal cord MRI at the time of pain assessment (see e-table 1 and e-figure 2 for prospective subset characteristics). The mean duration between pain-associated MRI and current MRI was 3.77 years (SD 3.63).
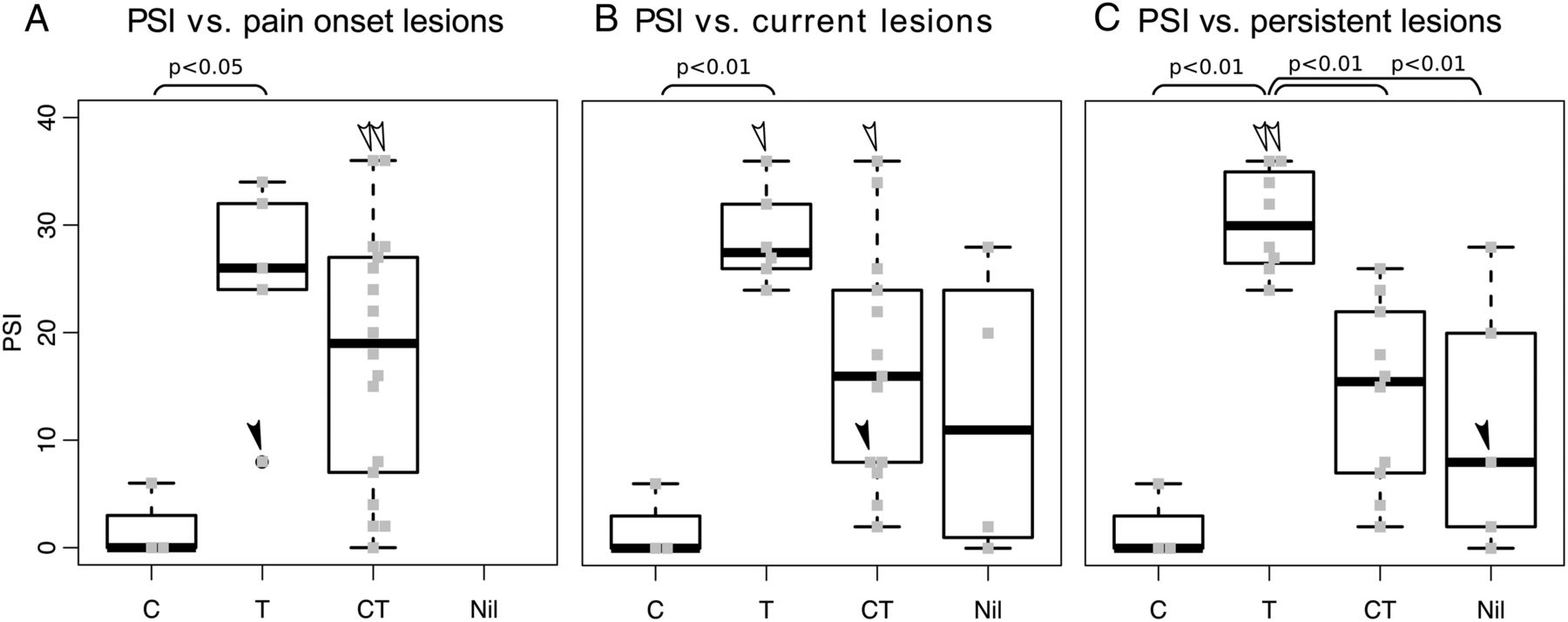
In line with the full cohort, PSI was significantly different across cord location groups for lesions associated with pain onset. PSI was also significantly different across cord location groups when assessing current (prospective) lesion location and, most strikingly, with persistent lesions (ie, lesions present at onset and still visible at prospective MRI). Remarkably, the isolated cervical and isolated thoracic groups for current and persistent lesions dissociated entirely when plotted against PSI (figure 2B, C).

PSI versus onset (A), current (B) and persistent (C) cord lesion locations for prospective subset. See text for description of white and black arrows. Boxplot figure calculated using first and third quartile, and median. C, isolated cervical; CT, cervicothoracic; Nil, no visible lesions; PSI, Pain Severity Index; T, isolated thoracic.
The only subject with a low current pain score and an isolated thoracic lesion associated with pain onset moved out of the isolated thoracic group as the lesion did not persist, instead a distinct cervicothoracic lesion was present at the time of current MRI (black-filled arrowheads in figure 2). The two subjects with the highest pain scores had cervicothoracic lesions associated with pain onset; however, only thoracic portions of these lesions persisted until the time of current MRI (unfilled arrowheads in figure 2; note one developed a new cervical lesion by the time of the current MRI).
The lesions midpoint strongly correlated with PSI. The correlation was strongest for persistent lesions with an r squared of 0.52 (r=0.72; p<0.01; figure 3).

{kind=link}
{kind=link}
{kind=link}
Current PSI versus persistent lesions midpoint. C, cervical level; PSI, Pain Severity Index; T, thoracic level; ▪, continuous isolated thoracic lesion; •, continuous isolated cervical lesion; ▴, continuous cervicothoracic lesions; ▵, discontinuous cervicothoracic lesion.
Again, lesion length as determined by longest lesion and total lesion burden did not correlate with pain scores (r<0.1 for both). Disease duration in the prospective cohort correlated negatively with pain (r=−0.41; p<0.05). EDMUS again correlated with PSI (r=0.56; p<0.01) as did the number of antineuropathic pain medications (r=0.66; p<0.01) and may reflect the resistant nature of NMOSD pain given the currently available pain treatments.
A multiple regression analysis with PSI as the dependent variable, and EDMUS, current age, age of onset, persistent thoracic lesions (y/n) and persistent cervical lesions (y/n) as independent variables produced a robust (adjusted R-squared 0.64) and significant (p<0.01) model, with highly significant (p<0.01) opposing contributions from cervical lesions (std. β=−0.46) and thoracic lesions (std. β=0.48) (table 2). Interestingly, EDMUS was now non-significant (p=0.231).
Summary for multiple regression statistics of prospective data (PSI as dependent variable)
When lesions midpoint was used in place of cervical and thoracic lesion variables, an equally predictive regression model resulted (adjusted R-squared 0.66; p<0.01) with significant factors (p<0.05) for lesions midpoint and current age, and a highly significant (p<0.01) effect from age of onset (data not shown).
Discussion
We report a significant relationship between the craniocaudal location of myelitis lesions and the severity of neuropathic pain: the presence of thoracic lesions predicts greater myelitis-associated chronic pain than the presence of cervical lesions. This relationship is strongest with persistent lesions and suggests that MRI evidence of chronic thoracic lesions represents lingering cord pathology that exacerbates the pain experience, with a converse and perhaps protective effect seen with some cervical lesions.
As documented in other neuromyelitis optica cohorts, a large percentage of our AQP4-Ab-positive TM patients suffer pain (86%); for a quarter of whom this pain is severe.1 ,3 ,13 This reinforces the importance of unravelling the aetiology of pain in NMOSD as a stepping-stone towards effective therapy development. There are scant published data about craniocaudal location of myelitis and pain. We suggest that one reason NMOSD TM sufferers experience more pain than MS patients might relate to the differing proportions of cervical and thoracic cord involvement in the two conditions.4 In support of this hypothesis, Okuda et al5 have reported that pain in MS associates with upper/mid-thoracic damage and propose an autonomic aetiology. A large number of autonomic areas receive information about the body's sensory state, including pain, directly or indirectly from ascending lamina I neurons of the spinal dorsal horn. There is a respected caucus of work that posits this afferent autonomic information as the source of the body's representational state of well-being, motivating behaviour to maximise comfort or to minimise pain.14 Ascending lamina I afferents project first to the sympathetic cell columns, autonomic nuclei found exclusively in the thoracolumbar cord, and there is evidence to suggest that some of these connections might be bidirectional.5 Damage to these autonomic thoracolumbar nuclei or their projections may have a dysregulative effect on pain information processing in the cord and a knock-on effect on one's qualitative experience of pain.
In this study, disability and age appeared to be greater in those with thoracic cord lesions; the disability effect survived regression analysis in the full cohort and appeared also to associate with pain. Alongside pain and disability in the regression analyses, however, an independent effect on pain intensity of lesions midpoint was evident in the whole group of 76 patients, and also for grouped cord location and lesions midpoint for the longitudinally imaged group. Indeed, in the longitudinally imaged group, disability was no longer a significant predictor of pain when analysed alongside grouped cord location.
There exists a large number of validated neuropathic pain screening questionnaires, such as PainDETECT,15 helpful when screening for a neuropathic aetiology with limited investigations (eg, without MRI or nerve conduction studies) but probably less relevant to our study. The definition of neuropathic pain as defined by the IASP, and the gold standard against which these neuropathic pain screening measures are validated, is ‘pain caused by a lesion or disease of the somatosensory nervous system … which requires a demonstrable lesion …’.8 As all of our patients met this gold-standard criterion, that is, all had pain attributable to confirmed myelitis lesions, we have not reported other neuropathic screening measures here.
Our study had some limitations. We did not have multiple pain scores throughout and thus it was difficult to unravel the effects of multiple TM attacks. Thus, we focused on the TM attack which the patient attributed to the start of their current pain. This assumes that only one attack causes current pain; however, perhaps surprisingly patients rarely recalled more than one TM attack having an effect on pain. In any case, this should not produce a bias towards one cord region unless lesion location was related to first or subsequent attack and this was not the case.
We did not have prospective axial imaging through the thoracic cord nor axial images of all patients to assess the additional effect of axial lesion location on pain severity. However, in our clinical experience, the vast majority of AQP4-Ab-positive TM patients have central lesions; some with whole-diameter cord involvement and some with more confined central grey matter involvement. Of the available high-resolution axial cervical images of lesions from the prospective cohort (14/16; two excluded due to movement artefact), all were central except a single patient with a dorsally located lesion. Of the pain onset clinical-grade MRIs with axial slices through lesions, again focusing on the prospective group (22/26; four patients had no axial imaging available), one had a dorsally located lesion (same patient as above) and the remainder were central or whole-diameter; there was no significant difference between the pain scores of whole-diameter and central lesions (Student's independent t-test, p=0.68), or between all three subgroups (three-way ANOVA, p=0.39; data in electronic supplement, e-table 2). Although the single dorsal cord lesion was associated with a zero pain score, the remainder of isolated cervical lesions were central and there was no other structured bias in terms of cervicothoracic and axial location that might confound our conclusion.
Formal testing of cognition was not performed. However, none of the patients in out cohort had apparent cognitive problems. Not all patients in this study had contemporary depression and anxiety measures or pain catastrophising scores, and we know that pain and emotional state have a complicated bidirectional relationship. However, in a recent study by our group, these factors did not independently predict PSI in AQP4-Ab-positive TM patients.16 Indeed, if these factors were confounders, this would reduce any effect of location on pain severity and should not detract from this study's conclusion.
In conclusion, the craniocaudal location, in particular persistent thoracic lesions, may be an important determinant of postmyelitis chronic pain severity. The possibility of cervical involvement playing a role in modifying pain is of interest and needs validating in further cohorts. The potential role of the autonomic nervous system in postmyelitis pain is intriguing and could provide additional therapeutic candidates for future pain studies.
References
Footnotes
GT and DV contributed equally.
Twitter Follow George Tackley at @gtackley
Contributors GT and DV involved in design of the study, data acquisition, analysis and interpretation of the data, drafting and revising the manuscript for intellectual content. SH involved in data acquisition and revising the manuscript for intellectual content. MJ, AV and MIL involved in analysis and interpretation of the data, and revising the manuscript for intellectual content. YK involved in design of the study, data acquisition and interpretation of the data. RG and KM involved in design of the study and data acquisition. MW involved in data acquisition, analysis and interpretation of the data. PW involved in data acquisition, analysis and interpretation of the data, and revising the manuscript for intellectual content. IT involved in conceptualisation of the study. AJ involved in design of the study and revising the manuscript for intellectual content. JP involved in conceptualisation of the study, interpretation of the data and revising the manuscript for intellectual content. Statistical analysis was conducted by GT.
Funding Guthy-Jackson Charitable Foundation.
Competing interests GT is funded by NHS National Specialised Commissioning Group for Neuromyelitis Optica, UK.SH is funded by NHS National Specialised Commissioning Group for Neuromyelitis Optica, UK. RG is funded by NHS National Specialised Commissioning Group for Neuromyelitis Optica, UK. KM is funded by NHS National Specialised Commissioning Group for Neuromyelitis Optica, UK. MW is funded by NHS National Specialised Commissioning Group for Neuromyelitis optica, UK. PW is supported by NHS National Specialised Commissioning Group for Neuromyelitis Optica, UK, and by the NIHR Oxford Biomedical Research Centre. He is a named inventor on patents for antibody assays (No: 20120114666, application No: 1310855.0) and has received royalties. He has received speaker honoraria from Biogen Idec and Euroimmun AG, and travel grants from the Guthy-Jackson Charitable Foundation. AV sat on the Advisory Editorial Board Neurology 2014 and was associate Editor for Brain (2013). She holds a patent with Oxford University for LGI1/CASPR2 antibodies, licensed to Euroimmun AG, and for GABAAR antibodies, in negotiation with Euroimmun AG. She receives royalties from Athena Diagnostics (MuSK assays), Euroimmun AG (LGI1 and CASPR2 assays), and publishing royalties from Clinical Neuroimmunology (Blackwell Publishing, 2005) and Inflammatory and Autoimmune Disorders of the Nervous System in Children (Mac Keith Press 2010). She did consultancy work with Athena Diagnostics for assessing their antibody assays (Ended 2014). She has received speakers' bureaus for scientific conference expenses only. She received funding support from NIHR for antibody work. MIL is involved in AQP4 testing; is supported by the National Health Service National Specialised Commissioning Group for Neuromyelitis Optica and by the National Institute for Health Research Oxford Biomedical Research Centre; and has received speaking honoraria from Biogen Idec and travel grants from Novartis. AJ has received honoraria for speaking on NMO from Biogen Idec and Chugai Pharmaceuticals. He has received a grant from Biogen. He is partly funded by NHS National Specialised Commissioning Group to run a national NMO service, and NIHR to run the Strive clinical trial 2014 (UK). JP is partly funded by highly specialised services to run a national congenital myasthenia service and a national neuromyelitis optica service. She has received conference funding for scientific meetings and honoraria for advisory work from Bayer Schering, Biogen Idec, Chugai Pharma, Merck Serono, Novartis, Ono Pharmaceutical Co. and Teva. She has received unrestricted research grants from Bayer Schering, Biogen Idec, Merck Serono and Novartis. Prospective imaging funded by Guthy-Jackson Charitable Foundation. YK has no competing interests.
Ethics approval Oxfordshire REC 07/Q1604/28; London-Hampstead REC 15/L01433; Berkshire REC 13/SC/0238.
Provenance and peer review Not commissioned; externally peer reviewed.