Article Text

Abstract
Importance Neuromyelitis optica spectrum disorders (NMOSD) can present with very similar clinical features to multiple sclerosis (MS), but the international diagnostic imaging criteria for MS are not necessarily helpful in distinguishing these two diseases.
Objective This multicentre study tested previously reported criteria of ‘(1) at least 1 lesion adjacent to the body of the lateral ventricle and in the inferior temporal lobe; or (2) the presence of a subcortical U-fibre lesion or (3) a Dawson's finger-type lesion’ in an independent cohort of relapsing-remitting multiple sclerosis (RRMS) and AQP4-ab NMOSD patients and also assessed their value in myelin oligodendrocyte glycoprotein (MOG)-ab positive and ab-negative NMOSD.
Design Brain MRI scans were anonymised and scored on the criteria by 2 of 3 independent raters. In case of disagreement, the final opinion was made by the third rater.
Participants 112 patients with NMOSD (31 AQP4-ab-positive, 21 MOG-ab-positive, 16 ab-negative) or MS (44) were selected from 3 centres (Oxford, Strasbourg and Liverpool) for the presence of brain lesions.
Results MRI brain lesion distribution criteria were able to distinguish RRMS with a sensitivity of 90.9% and with a specificity of 87.1% against AQP4-ab NMOSD, 95.2% against MOG-ab NMOSD and 87.5% in the heterogenous ab-negative NMOSD cohort. Over the whole NMOSD group, the specificity was 89.7%.
Conclusions This study suggests that the brain MRI criteria for differentiating RRMS from NMOSD are sensitive and specific for all phenotypes.
Statistics from Altmetric.com
Introduction
Differentiating multiple sclerosis (MS) from other relapsing inflammatory conditions such as neuromyelitis optica spectrum disorders (NMOSD) is important, because treatments for both diseases differ and determine the clinical outcome.1 ,2 Imaging is one of the most important diagnostic tools. When spinal cord lesions are present, the length of the lesion can be a useful distinguisher but long lesions can also occur in MS,3 and short lesions in NMOSD.4 Similarly, although it is now accepted that the brain MRI is often abnormal in NMOSD and may have characteristic features that differ from MS,5 the Barkhof criteria for MS are satisfied in up to 42%.6 ,7 We recently identified some brain imaging characteristics that differed between MS and AQP4-ab NMOSD.6 We found that the presence of (1) at least one lesion adjacent to the body of the lateral ventricle and in the inferior temporal lobe; or (2) the presence of an S-shaped U-fibre lesion; or (3) a Dawson's finger-type lesion, distinguished patients with MS from those with AQP4-ab positive NMOSD with 92% sensitivity, 96% specificity, 98% positive predictive value (PPV) and 86% negative predictive value (NPV).6 These criteria could be applied in everyday clinical practice across centres and scanners. The aim of this study was to evaluate the presence of these features in a new cohort of RRMS and AQP4-ab NMOSD patients, recruited from three centres, and to test the criteria not only in AQP4-ab-positive NMOSD patients, but also in NMOSD patients with myelin oligodendrocyte glycoprotein (MOG)-abs or without any detectable antibody who are difficult to distinguish from MS with predominant optic nerve and/or spinal cord involvement.
Methods
Patient consents
All patients gave their written consent for the use of their anonymised MRI scans for research purposes.
Patients
A total of 112 patients (44 RRMS (Oxford and Strasbourg), 31 AQP4-ab-positive NMOSD (Oxford, Strasbourg and Liverpool), 21 MOG-ab positive NMOSD and 16 ab-negative NMOSD/MS overlap patients (both from Oxford)) were recruited from 3 European clinical MS and neuromyelitis optica (NMO) centres. MS was diagnosed on the basis of clinical and paraclinical tests including Barkhof MRI imaging criteria,8 while NMOSD was diagnosed according to the presence of long cord lesions and/or severe optic neuritis and the result of antibody testing. MRI criteria assessed in this study had no place in the clinical diagnosis. All patients were selected for the presence of brain lesions. No patients with known cerebrovascular disease have been included in the study.
Antibody testing
AQP4-antibody testing was performed using a cell-based assay with M23 isoform of AQP4 in Oxford or Strasbourg as described previously.9 MOG antibody testing was performed in Oxford using a cell-based assay detecting antibodies of IgG1 class targeting full-length MOG.10
Brain scans and scoring
Clinical brain MRI scans including T2-weighted and fluid-attenuated inversion recovery (FLAIR) sequences were acquired on various 1.5 T scanners (Siemens, GE, Philips) in multiple centres (Oxford, Liverpool, Strasbourg, but also other centres who would refer their patients to one of these and transfer images). Dual coils were typically used. Slice thickness ranged from 3 to 6 mm; in-plane resolution was 0.5–1 mm. For T2-weighted images, repetition time ranged from 2400 to 2700 ms and echo time ranged from 80 to 100 ms. For FLAIR sequence, repetition time was 6500–8800 ms and echo time was 80–120 ms. Scans were anonymised locally and transferred to the Oxford Centre for Functional MRI of the Brain (FMRIB), where they were scored by two independent raters with a third resolving discordance (MJ, GT, RG) using FSLview (FMRIB Software Library V.5.0, University of Oxford) on a set of four features previously reported to be useful differentiators of MS and AQP4-ab NMOSD brain MRI: lesions adjacent to the body of the lateral ventricle, lesions in inferior temporal lobe, S-shaped/curved U-fibre lesions and Dawson's fingers. T2-weighted and FLAIR sequences were used for scoring.
Statistics
Cohen's κ was used to assess inter-rater agreement.11 κ<0 indicates poor agreement, 0.01–0.20 slight, 0.21–0.40 fair, 0.41–0.60 moderate, 0.61–0.80 substantial and 0.81–1.0 almost perfect agreement. On the basis of the final diagnosis (MS or NMOSD), the imaging findings were classified as true positive (TP, criteria fulfilled and diagnosis MS), true negative (TN, criteria negative, diagnosis NMOSD), false positive (FP, criteria positive, diagnosis NMOSD) or false negative (FN, criteria negative, diagnosis MS). Sensitivity was determined by the ratio TP/(TP+FN) and specificity by TN/(TN+FP). PPV was defined as TP/(TP+FP), and NPV was defined as TN/(TN+FN).
Results
The inter-rater reliability was found to be κ=0.76, 95% CI (0.62 to 0.89).
The criteria were fulfilled by 90.9% RRMS, 12.9% AQP4-ab NMOSD, 4.8% MOG-ab NMOSD and 12.5% ab-negative NMOSD/MS overlap patients. Basic clinical and demographic information about the patients including gender, age at onset, median follow-up and expanded disability status scale (EDSS) is shown in table 1.
Basic clinical and demographic information about the patients included in the study
The criteria showed 90.9% sensitivity, 89.7% specificity, 85.1% PPV and 93.9% NPV in distinguishing RRMS from all types of NMOSD.
When distinguishing RRMS from AQP4-ab NMOSD the criteria had a specificity of 87.1%, PPV of 90.9% and NPV of 87.1% (table 2). When distinguishing from MOG-ab NMOSD, the specificity was 95.2%, PPV 97.6%, NPV 83.3% (table 3), and for ab-negative NMOSD/MS overlaps specificity was 87.5%, PPV 95.2% and NPV 77.8%.
Number of patients fulfilling the criteria and the sensitivity and specificity of each criterion or of combination of criteria for the discrimination between RRMS and AQP4-ab NMOSD
Number of patients fulfilling the criteria and the sensitivity and specificity of each criterion or of combination of criteria for the discrimination between RRMS and MOG-ab NMOSD
Outliers from the criteria
Four of the RRMS patients (9.1%) did not fulfil the brain imaging criteria for MS. Interestingly, three of them were diagnosed with a benign form of MS and were not on disease-modifying therapy. One patient had lesions adjacent to the body of a lateral ventricle that were not accompanied by other types of lesions included in the criteria.
Four of the AQP4-ab NMOSD patients (12.9%) fulfilled the criteria. Two of them had S-shaped U-fibre lesions (figure 1A, B), and one patient had a callosal lesion which resembled a Dawson's finger (figure 1C). One patient was scored to have lesions adjacent to the body of lateral ventricles, an inferior temporal lobe lesion and a Dawson's finger-type lesion (figure 1D).
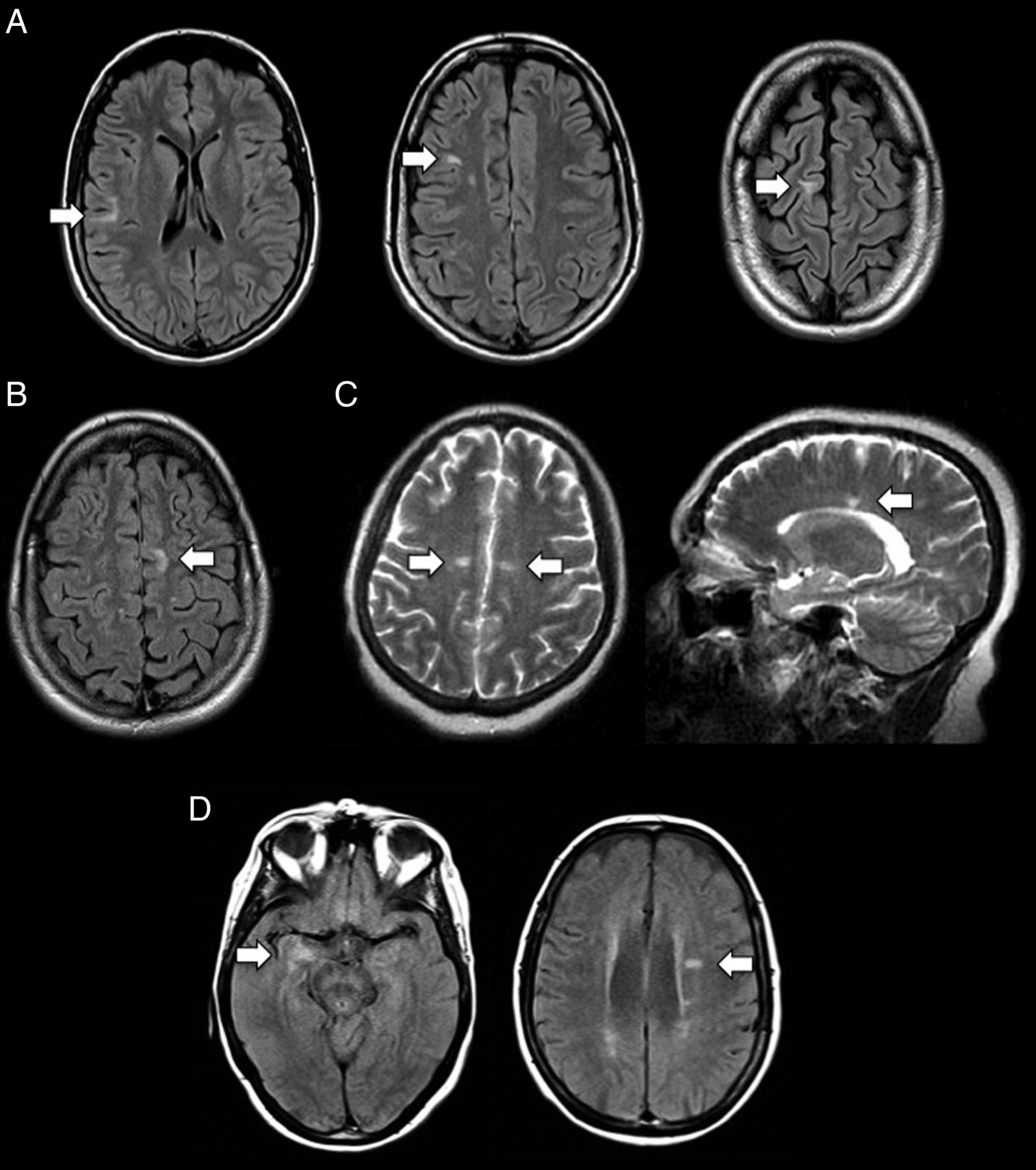
Brain MRI images of four AQP4-ab NMOSD patients who fulfilled brain lesion distribution criteria. Lesions are showed with white arrows. Patients (A) and (B) had curved U-fibre juxtacortical lesions. Patient (C) had bilateral callosal lesions in keeping with Dawson's fingers. Patient (D) had lesions in the inferior part of the right temporal lobe and adjacent to the body of a lateral ventricle. NMOSD, neuromyelitis optica spectrum disorders.
Only one MOG-ab patient (4.8%) fulfilled the criteria. He had an S-shaped lesion which involved cortex and U-fibres. This patient also had a fluffy brainstem lesion typical of MOG-ab disease (figure 2).

{kind=link}
{kind=link}
Brain MRI images of the MOG-ab NMOSD patient who fulfilled brain lesion distribution criteria. Lesions are showed with white arrows. Curved/S-shaped U-fibre lesions (left and middle image) were accompanied by a fluffy brainstem lesion (on the right). MOG, myelin oligodendrocyte glycoprotein; NMOSD, neuromyelitis optica spectrum disorders.
A total of 16 ab-negative NMOSD/MS overlap patients were included, of whom 10 had a final diagnosis of ab-negative NMOSD. The remaining six had more MS-like syndromes (opticospinal disease with MS-like features, ie, short lesions in the spinal cord, good recovery from optic neuritis, progression of disability between relapses), and two of these fulfilled the imaging criteria for MS. One of these had Dawson's fingers, lesions perpendicular to the body of a lateral ventricle and inferior temporal lobe lesions, while the other one had a lesion adjacent to the body of lateral ventricle and an inferior temporal lobe lesion.
Discussion
In this study, we confirmed in a fully coded multicentre cohort of RRMS and AQP4-ab NMOSD patients that there are imaging criteria for MS that can differentiate RRMS from AQP4-ab NMOSD patients, with high sensitivity and high specificity. The criteria can also differentiate RRMS from MOG-ab NMOSD and ab-negative NMOSD.
In clinical practice, AQP4-ab-negative NMOSD patients are a diagnostic challenge when wishing to categorise them according to their underlying pathological process. The disagreement on the diagnosis of these patients is high even among NMO and MS experts.12 The diagnostic criteria cannot be easily validated in the ab-negative patients, who are heterogenous and often have overlapping features of NMOSD and MS,12 and some turn out to have a monophasic illness.13 ,14 Moreover, many studies have now found that MOG-abs define a subgroup within this AQP4-ab negative population and it was reassuring that the imaging criteria performed well in this group distinguishing the majority from MS.10 ,15–17
Our ab-negative NMOSD group as in all such cohorts will contain a mix of pathogenic processes and so we used best clinical diagnosis made in Oxford NMO clinic, that is, ab-negative NMOSD or an ‘MS-like syndrome’. We have found that the imaging criteria were fulfilled by 33% of patients with the diagnosis of ‘MS-like syndrome’ and none of those with the diagnosis of ab-negative NMOSD.
The aim of the study was to propose criteria, which could be applied across centres and scanners. The scans came from different scanners and might have differed in parameters such as slice thickness, which might have lowered sensitivity of lesion detection. Despite that the criteria showed good discrimination, which we consider a strength of this study. The criteria could be used in everyday clinical practice across the globe (noting NMO is a worldwide disease affecting less developed countries) as they require only conventional T2-weighted and FLAIR sequences. It is worth noting that the accuracy of the criteria could be potentially further increased if more advanced, non-conventional techniques detecting cortical lesions or perivenous white matter lesions were used,7 although those are typically not available in routine clinical services.
Several limitations of this work exist. The brain MRI criteria are only useful in patients with brain abnormalities, and spinal cord imaging has not been included. We focused on brain lesions as the most challenging cases we see are those in whom typical cord lesions are absent and we aimed at assessing how brain differentiators perform independently. We expect though that the presence of longitudinally extensive transverse myelitis (LETM) would strongly discriminate in favour of NMOSD as it was already showed before and incorporated into the NMOSD criteria.3 The criteria studied here rely on the ambiguous definition of Dawson's fingers,18 although this is only one of three possible criteria and as with all imaging classifications, clinicians with experience in characterising inflammatory imaging algorithms should be used. The lack of 100% inter-rater agreement demonstrates that there is operator variability, but as neurologists without neuroradiology experience served as the scorers and obtained good agreement, the variability is likely to reduce further with more experience and training. The predictive values relate to the proportional mix of patients included in our study. This has been enriched for NMOSD patients. Thus, our predictive values are likely to be relevant in NMO clinics or in areas of the world where MS has low prevalence. In a Western Caucasian population where NMOSD is much rarer than MS the PPV would increase and NPV would decrease. Thus, the criteria should be extrapolated in context. Assessing the criteria across different ethnic groups is needed in the future. Finally, as mentioned, we cannot be sure what the underlying pathological diagnosis in the antibody negative NMOSD group to truly judge the accuracy of the criteria in this group.
In conclusion, this study has validated the MS/NMOSD criteria in an independent cohort of RRMS and AQP4-ab NMOSD patients, has extended their use into AQP4-ab negative NMOSD and thus supports their incorporation into the recently revised diagnostic criteria for NMOSD as red flags.19
Acknowledgments
The authors gratefully acknowledge the UK National Specialised Commissioning Team for funding the Neuromyelitis Optica service in Oxford. MJ received research fellowship from the Polish Ministry of Science and Higher Education programme Mobilnosc Plus (1070/MOB/B/2013/0). AQP4 and MOG antibody testing in Oxford has been established and supported partly by the NIHR Oxford Biomedical Research Centre.
References
Footnotes
Contributors MJ and JP involved in drafting the manuscript. All authors contributed to revision of the manuscript and involved in contribution of vital reagents/tools/patients. LM and JP involved in study concept or design. MJ, YK and JP contributed to analysis or interpretation of the data. MJ, GT, RG, LM and JP involved in acquisition of data. MJ performed statistical analysis. JP involved in study supervision or coordination.
Competing interests None declared.
Patient consent Obtained.
Ethics approval Oxford Research Ethics Committee C Ref: 10/H0606/56.
Provenance and peer review Not commissioned; externally peer reviewed.