Article Text

Abstract
Objective To investigate the association between physical activity (PA) and amyotrophic lateral sclerosis (ALS) in population-based case–control studies in three European countries using a validated and harmonised questionnaire.
Methods Patients with incident ALS and controls were recruited from five population-based registers in The Netherlands, Ireland and Italy. Demographic and data regarding educational level, smoking, alcohol habits and lifetime PA levels in both leisure and work time were gathered by questionnaire, and quantified using metabolic equivalent of task scores. Logistic regression models adjusting for PA-related factors were used to determine the association between PA and ALS risk, and forest plots were used to visualise heterogeneity between regions.
Results 1557 patients and 2922 controls were included. We found a linear association between ALS and PA in leisure time (OR 1.07, P=0.01) and occupational activities (OR 1.06, P<0.001), and all activities combined (OR 1.06, P<0.001), with some heterogeneity between regions: the most evident association was seen in the Irish and Italian cohorts. After adjustment for other occupational exposures or exclusion of patients with a C9orf72 mutation, the ORs remained similar.
Conclusion We provide new class I evidence for a positive association between PA and risk of ALS in a large multicentre study using harmonised methodology to objectively quantify PA levels, with some suggestions for population differences.
Statistics from Altmetric.com
Introduction
Ever since American baseball player, Lou Gehrig, and later many other professional athletes developed amyotrophic lateral sclerosis (ALS), physical activity (PA) has been hypothesised as a risk factor for this fatal neurodegenerative disease.1 Numerous studies have reported on the association between PA and ALS with conflicting results, describing PA as either increasing or decreasing the risk of developing ALS.2 It is important to elucidate the direction of this association, since this could support pathophysiological mechanisms underlying ALS, such as oxidative stress and glutamate excitotoxicity or glial activation and altered levels of antiapoptotic proteins or neurotrophic factors.3 4
The previous conflicting results may be due to differences in study design and methods.2 These include various types of PA quantification, no specification of activities to allow a distinction to be made between leisure-related and job-related activities, hospital-based cohorts or case studies without (matched) controls, or different ways of considering confounding PA-related factors such as smoking and alcohol. Moreover, PA may only be a risk factor in certain populations, depending on their genetic background or environmental or lifestyle factors and may (partly) explain the observed phenotypic heterogeneity between populations.5
We, therefore, investigated the association between PA and ALS in a multicentre and cross-cultural setting, in ongoing population-based case–control studies in The Netherlands, Ireland and Italy, using a validated and methodologically harmonised questionnaire.
Methods
Study population
Participants were recruited as part of a case–control study undertaken by the Euro-MOTOR consortium (FP7/2007–2013; grant agreements no. 259867) initiated in February 2011 and concluded in February 2014. Incident cases (18 years and older) representing patients with definite, (laboratory-supported)probable or possible ALS, according to the revised El Escorial Criteria,6 were matched to controls based on age, gender and residency. Controls were identified and enrolled by local general practitioners during routine visits. The study consists of a written survey carried out in three European countries: The Netherlands, Ireland and Italy (in particular Apulia, Lombardy and Piedmont and Valle d’Aosta Italian regions). The aim and a more extensive description of this project are presented elsewhere.7 All participants gave written informed consent.
Data collection
The same structured questionnaire was used by the different study centres (Dublin, Utrecht, Bari, Milan and Turin) to collect demographic characteristics of participants and data on their educational level, smoking and alcohol history and lifetime physical activities. Highest educational level completed was categorised into International Standard Classification of Education (ISCED) 0–4 and ISCED 5–8 according to the ISCED 20118 in order to allow comparability between countries. Detailed data were collected on age at the start and cessation of smoking and alcohol drinking. Smoking and alcohol status were categorised as never, former or current. Additionally, participants were asked to state the numbers of cigarettes smoked daily. Lifetime cigarette smoking was expressed in pack-years (number of packs of cigarettes, years spent smoking, defining a pack as 20 cigarettes and including periods of light and heavy smoking).
Participants were asked to recall all their jobs and to describe the various work activities they had to perform. They were also asked to list all their leisure time activities, consisting of sports and hobbies, and to state the number of years and how many hours per week each activity had been performed.
In Ireland and Italy, face-to-face interviews were held to gather the data. In The Netherlands, due to feasibility reasons, participants filled in the questionnaire on paper. Participants were approached by telephone to complete or clarify the data. In cognitively impaired individuals, the data were obtained by an informed caregiver (1.6% of all participants). In addition to the above-mentioned topics, the questionnaire contained questions on several other exogenous factors. Participants were, therefore, blinded to the specific hypotheses being tested. Clinical data were collected through the patients’ medical records.
Classification of physical activities
In an attempt to quantify the cumulative lifetime PA level of participants objectively, all reported activities were scored and coded based on the Compendium of Physical Activities.9 The Compendium provides a coding scheme that links specific activities performed in various settings with their respective metabolic equivalent of task (MET), an expression of the energy expenditure as a ratio of the standard resting metabolic rate (sitting quietly). A MET score of 1.0 is defined as 1 kcal/kg body weight/h. The lifetime scores per participant were calculated as follows:

where k represents an activity from the lifetime PA history. Because of the magnitude of the lifetime score, it was divided by 1000. Military service, for which specific tasks were not available, or periods spent as a homemaker were excluded because of difficulties quantifying these activities.
Statistical analysis
All exposures were calculated up to 3 years prior to survey participation for both cases and controls. Logistic regression for lifetime MET scores for the different categories of activities, that is, leisure time (sport and hobbies), occupational and all combined, was used to determine the association between PA and risk of ALS. We adjusted for confounding variables age, gender, education, smoking and alcohol (current, former and never) and the five regions. We visualised possible heterogeneity between regions using forest plots. For the category of occupation-related activities, we also created a model adjusting for never/ever occupational exposure to: mineral dusts, asbestos and silica, organic dusts, animal contacts and endotoxin, pesticides, herbicides, insecticides and fungicides, gasses and fumes, diesel motor exhaust and polycyclic aromatic hydrocarbons, metals, chromium and nickel, solvents, aromatic solvents and chlorinated solvents, extremely low-frequency magnetic fields, electric shocks and benzene. These exposures were assessed through job exposure matrices (JEMs) and methodologically described elsewhere, with the exception of the JEM for benzene, which has been newly developed by RCH Vermeulen.10–13 Restricted cubic spline regression models were used to study how the dose–response relationship between PA and ALS could best be described.
Several sensitivity analyses were performed. First, we tested whether the association between PA and ALS was different for men and women using an interaction term and used the likelihood ratio test to compare the models with and without the interaction term. Second, since C9orf72 repeat expansions are the most common genetic abnormality in ALS, and patients with this mutation may represent a subgroup with different lifestyle and environmental factors, we performed a separate analysis excluding ALS patients with a C9orf72 repeat expansion, determined by methods described elsewhere.14 15 Third, to explore the effect of educational level on the association between PA and risk of ALS, we matched one patient to one control based on age, gender, region and educational level, ending up with 1487 matched pairs. In these ‘matched’ analyses, all exposures were calculated up to onset (of the patient) for both the patient and the matching control. The models were adjusted for smoking and alcohol (current, former and never). Fourth, above-mentioned models were based on complete case analyses, but we also multiply imputed the raw data of all PA-related data in the ‘original’ dataset, such as hours per week, start and stop year, as well as the confounding variables using multivariate imputation by chained equations and used Rubin’s rules to combine the estimates.16 17 Lastly, we investigated whether PA modifies the phenotype of ALS. Using bulbar or spinal site of onset as dependent variable in a multivariate model with the same confounders as previously described, we determined if the association between PA and ALS is different for bulbar and spinal patients. Additionally, we formally tested whether PA is associated with age at onset in patients using an interaction term between age of survey (for patients this is highly correlated with age at onset) and the lifetime MET scores. To calculate the MET scores for this specific analysis, we used the previously described formula without the activity duration (in years), because the duration of participation in an activity could be influenced when PA results in a younger age at onset.
The level of significance was set at P<0.05, and hypothesis tests were two sided. The analyses were performed in R with the stats and psych package for the descriptive statistics, the lmtest package for the main analyses and the survival package for the ‘matched’ analyses.
Results
Baseline characteristics and confounding factors
In total, 1557 patients and 2922 controls were included. Baseline characteristics of the study population per region can be found in table 1. Since PA of military activities were difficult to quantify, these were not included in the MET calculation in the 28.7% of patients and 29.7% of controls who were engaged in active military service (χ2 test: P=0.51). Compared with controls, patients were more often smokers, they also smoked more (in pack-years) and drank less alcohol (table 1).
Baseline characteristics
Physical activity and ALS risk
Table 2 shows that lifetime PA was found to increase ALS risk in the complete case dataset, for leisure time (sports and hobbies; OR 1.07, 95% CI 1.02 to 1.12, P=0.01), occupational activities (OR 1.06, 95% CI 1.03 to 1.09, P<0.001) and for all activities combined (OR 1.06, 95% CI 1.04 to 1.09, P<0.001). In addition, excluding smoking and alcohol from the model, we found similar effects: leisure time: OR 1.05, 95% CI 1.00 to 1.10, P=0.06; occupational activities: OR 1.06, 95% CI 1.03 to 1.09, P<0.001; and all activities combined: OR 1.06, 95% CI 1.03 to 1.09, P<0.001. As shown in figure 1, the ORs from the different regions point consistently in the same direction, but results are heterogeneous: an effect of PA increasing the risk of developing ALS is most evident in the Irish and Italian cohorts and less in the Dutch cohort. Adding other occupational exposures to the model for occupational activities left the risk estimates relatively unchanged (OR 1.04, 95% CI 1.00 to 1.07, P=0.05). The association between PA and ALS was found to be linear: the more active a person has been, the higher their risk of having ALS (figure 2).
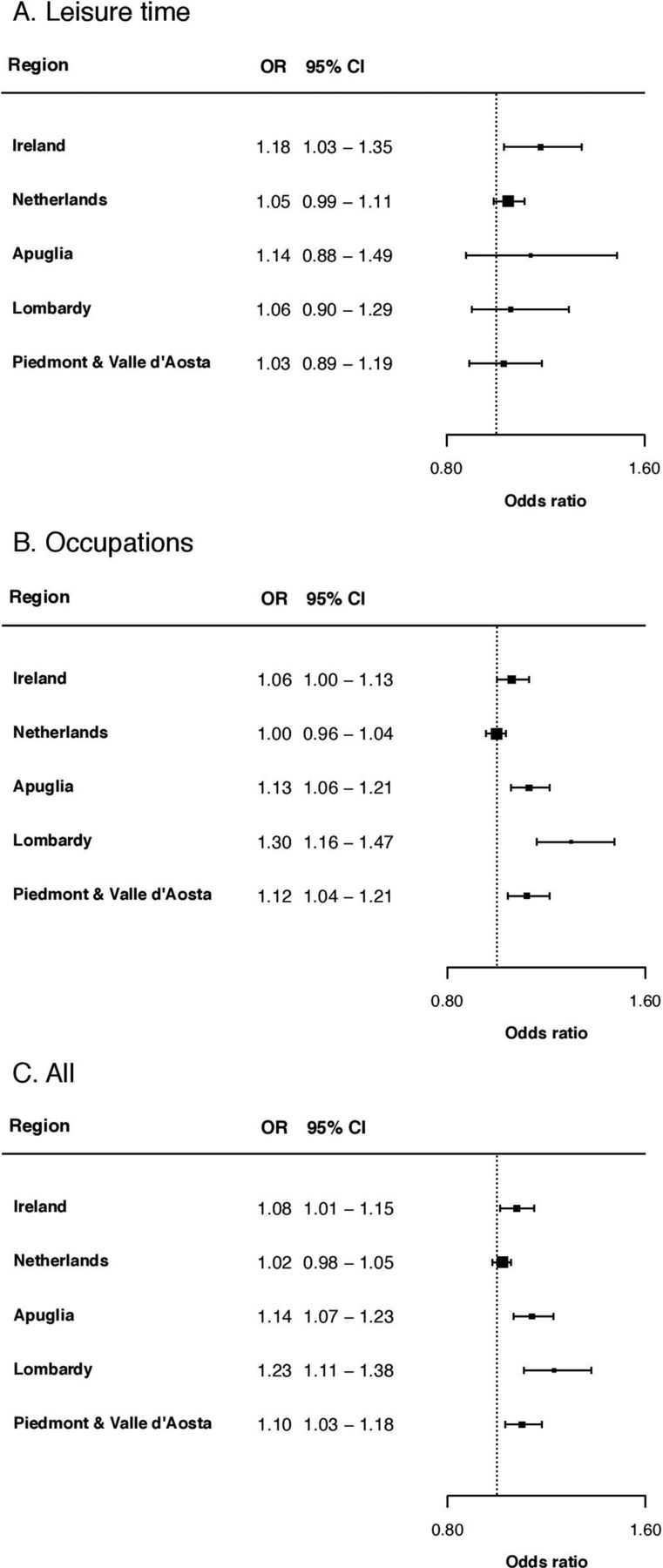
Forest plot showing centre-specific ORs and 95% CIs for physical activity and ALS, adjusted for age, gender, education, smoking, alcohol and centre. (A) Leisure time activities: combination of sports and hobbies. (B) Occupations. (C) All activities: combination of sports, hobbies and occupations. ALS, amyotrophic lateral sclerosis.

{kind=link}
{kind=link}
The risk of amyotrophic lateral sclerosis (OR) associated with a certain lifetime MET score of all activities combined (in the complete case dataset) using a lifetime MET score of zero as the reference. MET, metabolic equivalent of task.
ORs for lifetime physical activities
Sensitivity analyses
We found no effect modification by gender as indicated by the absence of model improvements when an interaction term between PA and gender was included (P values for the different categories of PA >0.05; data not shown). Excluding C9orf72 patients, we found similar effect sizes for leisure time activities (OR 1.07, 95% CI 1.02 to 1.13, P=0.01), occupations (OR 1.06, 95% CI 1.03 to 1.09, P<0.001) and for all activities combined (OR 1.07, 95% CI 1.04 to 1.10, P<0.001). Maximal adjustment for educational differences between patients and controls using the one-to-one matched model resulted in a minimal increase in ORs for leisure time (OR 1.11, 95% CI 1.04 to 1.18, P=0.002), occupational activities (OR 1.08, 95% CI 1.03 to 1.12, P<0.001) and all activities combined (OR 1.07, 95% CI 1.03 to 1.12, P=0.001; table 2). Moreover, after imputation, the ORs remained similar for leisure time activities (OR 1.03, 95% CI 1.00 to 1.06), occupations (OR 1.06, 95% CI 1.03 to 1.08) and the activities combined (OR 1.04, 95% CI 1.02 to 1.06). PA did not influence the ALS phenotype as expressed by the site of onset or age at onset (data not shown).
Discussion
In this large, multicentre, population-based case–control study, we found a linear association between lifetime PA and the risk of ALS. The increase of ALS risk associated with PA was independent of important confounders, such as age, gender, education, smoking and alcohol, gathered using a validated and methodologically harmonised questionnaire.
Through this multicentre collaboration and by examining different categories of PA (leisure time or occupational), we were able to gain greater insight into population heterogeneity and specific categories of activities as possible explanations for the conflicting earlier reported results. We found the association between PA and ALS to be most evident in the Irish and Italian cohorts. Although the forest plots showed some heterogeneity between the five regions, the patterns among the different categories of activities were divergent. This observation makes heterogeneity due to a systematic measurement bias, such as face-to-face interviews in Ireland and Italy and self-administered questionnaires in The Netherlands, unlikely.
The effect of occupational PA on ALS is similar after correction for other occupational exposures and also leisure time activities increase the risk of having ALS. These findings indicate that PA is not simply a proxy for exposures that increase the risk of ALS in active jobs, for example, exposure to pesticides when performing heavy work as a farmer. However, unaccounted confounding by medical events (trauma) or diet18–20 cannot be ruled out, nor some metabolic or energy deficit that is activity induced, which might render motor neurons susceptible.
We found a linear association between PA and ALS risk supporting the hypothesis that vigorous PA increases the risk of ALS most significantly. This is in line with reports that describe a higher prevalence of patients with ALS among (former) professional athletes.21–26 Previous studies, showing a positive association between leisure time or occupational PA and ALS risk or mortality,21 27–30 mostly found associations with strenuous activities only.21 29–31 In our multicentre, cross-cultural, population-based study including 1557 patients with ALS and 2922 controls, however, we also found a significant increase in ALS risk for persons who exercise recreationally (moderate activity).
We could only speculate on the mechanism by which PA leads to ALS. As is becoming increasingly recognised, ALS is a disorder of the brain (neocortex) and more specifically of cortical networks.32 33 The hypothesis about the role of cortical mechanisms underlying the association between PA and ALS is clinically supported by the finding of concordance between hand dominance (relatively greater use than the other hand) and upper limb onset.34
Our findings are at variance with recent analyses within a large European cohort study, for which a weakly inverse association between total PA and ALS mortality was reported.35 Also in a previous case–control study, including 652 patients and 1166 controls, without overlap of included participants with this study, done in five European countries (Italy, Ireland, UK, France and Serbia),36 an inverse correlation was found between leisure time PA and ALS. Data were adjusted for age, education, smoking, alcohol and centre as in the current study, and for traumatic events. The difference could, at least in part, be explained by the adverse effects of trauma. Traumatic injury acted as effect modifier in that study: those who were not physically active, but did experience traumatic injuries, were at risk of developing ALS. As history of trauma has been associated with an increased risk of ALS in some studies,37 a possible role of trauma as a risk factor cannot be entirely excluded. However, adjusting for ever having experienced a traumatic injury in our study did not change the odds ratios for PA (data not shown). This could be investigated further in prospective studies not tainted by recall bias.
Strengths of our study are the relatively large sample size of clinically confirmed patients and population-based controls, availability of the C9orf72 genotype in most patients, the use of the same definitions of exposures and the harmonised methods for data collection across centres.
The increased risk associated with PA found in our study may suggest that this is not a major factor in the pathogenesis of ALS. An OR of 1.06 for all activities combined can be translated in a 26% increase in risk when comparing a person who is more active than average (as defined by the 75th percentile) and a person who is less active than average (as defined by the 25th percentile). PA may have a larger effect in presently unidentified, potentially genetically enriched, subgroups of patients. The ORs are consistent between sensitivity analyses, which we performed to study the effect of educational level, C9orf72 genotype or missing data on the association between PA and ALS risk. The fact that we found similar effect sizes in the complete case analyses and the analyses with the imputed data suggests that the missings are not merely dependent on how active a person has been, and although we had missing data on C9orf72 for 41.6% of the Italian patients (missings per region/centre: 98.6% in Apulia/Bari, 57.0% in Lombardy/Milan, 0% in Piedmont and Valle d’Aosta/Turin), the ORs did not change for the Irish (2.3% missing) and Dutch (7.2% missing) cohorts after exclusion of patients with a C9orf72 repeat expansion (data not shown). The genetic background may differ between the five cohorts studied, for example, mutations in the gene encoding Cu/Zn superoxide dismutase (SOD1) are common in Italy but rare in Ireland and The Netherlands.38–40 Differences in the effect of gene–environment interaction due to variable genetic background of the five regions could explain the heterogeneity of results between the five regions in our study.
A limitation of this study could be a possible influence of recall bias on the results, which might explain the variance in the results when compared with previous studies. However, to minimise the role of recall bias, patients were kept unaware of the objectives of the study. For example, instead of asking participants directly how active they have been in leisure time or occupational activities, recall bias was reduced by using the Compendium of Physical Activities to quantify PA objectively. Another limitation could be the presence of interview bias as interviews were done by research assistants. Interview bias is difficult to control for because a blind interview is not feasible when one is in direct contact with patients with ALS. To minimise interview bias, research assistants did not participate in research meetings or analyses of results. In addition to the strengths mentioned above, other strengths are the use of a questionnaire carefully validated in Dutch, Italian and English, the population-based setting with controls being representative of the general population and relatively complete data on a number of possible confounders gathered by using the same methods of collection.
In this study, we provide new class I evidence for a linear association between PA and risk of ALS in a large multicentre, population-based, cross-cultural, case–control study using harmonised methodology to objectively quantify PA levels, with some suggestions of population differences. Overall, PA has been demonstrated to be protective against many diseases including cardiovascular disease, diabetes and a variety of cancers. Decreasing the risk of these common conditions may be a trade-off with increasing the risk of a relatively rare disease such as ALS.
References
Supplementary materials
Press release
Files in this Data Supplement:
Footnotes
JHV and LHB contributed equally.
AEV, JPKR and FD’O contributed equally.
Contributors AEV: study concept and design, data collection and processing, statistical analyses, contribution to the analysis and interpretation of data and writing of the manuscript. JPKR and FD: study concept and design, data collection and processing, statistical analyses, contribution to the analysis and interpretation of data, revision of the manuscript for important intellectual content. HJW: study concept and design, statistical analyses, contribution to the analysis and interpretation of data, revision of the manuscript for important intellectual content. RCHV: study concept and design, contribution to the analysis and interpretation of data, revision of the manuscript for important intellectual content and provided study supervision. EB, AC, GL, OH, JHV and LHvdB: study concept and design, data collection and processing, contribution to the analysis and interpretation of data, revision of the manuscript for important intellectual content, provided study supervision and obtained funding.
Funding The research leading to these results has received funding from the European community’s health seventh framework programme (FP7/2007–2013; grant agreements no. 259867), The Netherlands ALS foundation and The Netherlands Organisation for Health Research and Development (Vici Scheme, JPND (STRENGTH)).
Competing interests AEV, FD, HJW, RCHV and GL report no disclosures. JPKR reports grants from health research board, during the conduct of the study. EB reports grants from UCB-Pharma, grants from Shire, grants from EISAI, personal fees from Viropharma, grants from Italian Ministry of Health, grants from European Union, grants from Fondazione Borgonovo, grants from Associazione IDIC 15, outside the submitted work. AC reports personal fees from Biogen Idec, personal fees from Cytokinetics, grants from Italfarmaco, personal fees from Mitsubishi, outside the submitted work. OH reports grants from framework 7 EUROMOTOR project, grants from Health Research Board Ireland, grants from Science Foundation Ireland, during the conduct of the study; personal fees from ALS FTD Journal, outside the submitted work. JHV reports other from Vertex Pharmaceuticals, outside the submitted work. LHvdB reports grants from Netherlands ALS Foundation, grants from The Netherlands Organisation for Health Research and Development, during the conduct of the study; grants from Baxalta, grants from Prinses Beatrix Spierfonds, grants from European Community’s Health Seventh Framework Programme, outside the submitted work; LHvdB serves on scientific advisory boards for the Prinses Beatrix Spierfonds, Thierry Latran Foundation, Biogen and Cytokinetics and serves on the editorial board of amyotrophic lateral sclerosis and frontotemporal degeneration and the journal of neurology, neurosurgery and psychiatry.
Patient consent Obtained.
Ethics approval The relevant institutional review boards gave ethical approval.
Provenance and peer review Not commissioned; externally peer reviewed.
Collaborators SCILLA Working Group collaborators: Andrea Bruno, MD (Department of Nuclear Medicine, Papa Giovanni XXIII Hospital, Bergamo, Italy); Carlo De Fanti, MD, Sara Fascendini, MD, Angela Tomasoni, MD (European Foundation for Biomedical Research, Alzheimer Center of Excellence, Briolini Hospital of Gazzaniga, Bergamo, Italy); Marco Arnaboldi, MD, Manuela Valsecchi, MS (Department of Neurology and Stroke Unit, Sant’Anna Hospital, Como, Italy); Massimo Moleri, MD (Neurology Unit, San Francesco Clinic, Bergamo, Italy); Marco Poloni, MD, Dario Alimonti, MD (Department of Neurology, Papa Giovanni XXIII Hospital, Bergamo, Italy); Fabrizio Tagliavini, MD, Veronica Redaelli, MD, Giuseppe Di Fede, MD, Ilaria Bizzozero, PsyD, Sara Prioni, PsyD (Division of Neurology V/Neuropathology, Scientific Institute for Research, Hospitalization, and Care (IRCCS), Foundation "Carlo Besta" Neurological Institute, Milan, Italy); Euro-MOTORconsortium: Anneke J van der Kooi, MD, PhD (Department of Neurology, Amsterdam Medical Center, University of Amsterdam, Amsterdam, The Netherlands); Joost Raaphorst, MD, PhD (Department of Neurology, Donders Institute for Brain, Cognition and Behavior, Center for Neuroscience, Radboud University Nijmegen Medical Center, Nijmegen, The Netherlands); Andrea Calvo, MD, PhD (“Rita Levi Montalcini” Department of Neuroscience, University of Torino, Torino, Italy); Cristina Moglia, MD, PhD (“Rita Levi Montalcini” Department of Neuroscience, University of Torino, Torino, Italy); Federico Casale, PhD (“Rita Levi Montalcini” Department of Neuroscience, University of Torino, Torino, Italy); Antonio Canosa, MD, PhD (“Rita Levi Montalcini” Department of Neuroscience, University of Torino, Torino, Italy); Umberto Manera, MD (“Rita Levi Montalcini” Department of Neuroscience, University of Torino, Torino, Italy); Davide Bertuzzo, MD (“Rita Levi Montalcini” Department of Neuroscience, University of Torino, Torino, Italy); Letizia Mazzini, MD (ALS Centre, Department of Neurology, "Maggiore della Carità", University Hospital, Novara, Italy); Enrica Bersano, MD (ALS Centre, Department of Neurology, "Maggiore della Carità", University Hospital, Novara, Italy); Mark Heverin (Academic Unit of Neurology, Trinity Biomedical Sciences Institute, Trinity College, Dublin, Ireland); Alice Vadja, PhD (Academic Unit of Neurology, Trinity Biomedical Sciences Institute, Trinity College, Dublin, Ireland); Elisabetta Pupillo (Department of Neurosciences, IRCSS, Mario Negri Institute of Pharmacological Research, Milan, Italy); Giancarlo Comi, MD; Nilo Riva MD, (IRCCS San Raffaele Hospital, Milan, Italy); Christian Lunetta, MD (NEMO Clinical Center, Serena Onlus Foundation, Niguarda Ca’ Granda Hospital, Milan, Italy); Francesca Gerardi, DrBT (NEMO Clinical Center, Serena Onlus Foundation, Niguarda Ca’ Granda Hospital, Milan, Italy); Massimiliano Filosto, MD (Civil Hospital of Brescia, Brescia, Italy); Maria Sofia Cotelli, MD (Civil Hospital of Brescia, Brescia, Italy); Fabrizio Rinaldi, MD (Civil Hospital of Brescia, Brescia, Italy); Luca Chiveri, MD (Ospedale Valduce, Como, Italy); Maria Cristina Guaita, MD (A.O. Civil Hospital, Legnano, Italy); Patrizia Perrone, MD (A.O. Civil Hospital, Legnano, Italy); Ceroni Mauro, MD (IRCCS National Neurorological Institute “C.Mondino”, Pavia, Italy); Luca Diamanti, MD (IRCCS National Neurorological Institute “C.Mondino”, Pavia, Italy); Carlo Ferrarese, MD (University of Milano-Bicocca, "San Gerardo" Hospital, Monza, Italy); Lucio Tremolizzo, MD (University of Milano-Bicocca, "San Gerardo" Hospital, Monza, Italy); Maria Luisa Delodovici, MD (“Ospedale di Circolo, Fondazione Macchi”, Varese, Italy); Giorgio Bono, MD (“Ospedale di Circolo, Fondazione Macchi”, Varese, Italy); Chiara Zecca, DrBiol (Department of Clinical Research in Neurology, University of Bari "A. Moro" at Pia Fondazione "Card. G. Panico", Tricase, Italy); Rosanna Tortelli, MD (Department of Clinical Research in Neurology, University of Bari "A. Moro" at Pia Fondazione "Card. G. Panico", Tricase, Italy).
Correction notice Since this paper was first published online, Nilo Riva has been added as a collaborator.
Linked Articles
- Editorial commentary