Article Text

Abstract
Objective To determine the diagnostic and prognostic performance of serum neurofilament light chain (NFL) in amyotrophic lateral sclerosis (ALS).
Methods This single-centre, prospective, longitudinal study included the following patients: 124 patients with ALS; 50 patients without neurodegenerative diseases; 44 patients with conditions included in the differential diagnosis of ALS (disease controls); 65 patients with other neurodegenerative diseases (20 with frontotemporal dementia, 20 with Alzheimer’s disease, 19 with Parkinson’s disease, 6 with Creutzfeldt-Jakob disease (CJD)). Serum NFL levels were measured using the ultrasensitive single molecule array (Simoa) technology.
Results Serum NFL levels were higher in ALS in comparison to all other categories except for CJD. A cut-off level of 62 pg/mL discriminated between ALS and all other conditions with 85.5% sensitivity (95% CI 78% to 91.2%) and 81.8% specificity (95% CI 74.9% to 87.4%). Among patients with ALS, serum NFL correlated positively with disease progression rate (rs=0.336, 95% CI 0.14 to 0.506, p=0.0008), and higher levels were associated with shorter survival (p=0.0054). Serum NFL did not differ among patients in different ALS pathological stages as evaluated by diffusion-tensor imaging, and in single patients NFL levels were stable over time.
Conclusions Serum NFL is increased in ALS in comparison to other conditions and can serve as diagnostic and prognostic biomarker. We established a cut-off level for the diagnosis of ALS.
Statistics from Altmetric.com
Introduction
Amyotrophic lateral sclerosis (ALS) is a neurodegenerative disease causing demise of motor neurons of the cerebral cortex, brainstem and spinal cord. This leads to progressive paralysis ending with death from respiratory failure after a median of 30 months. Up to 10% of patients with ALS are also affected by frontotemporal dementia (FTD),1 while 5%–10% of ALS cases are familial and caused by mutations in known genes.2 The diagnosis of ALS is primarily clinical; fluid biomarkers have not yet entered clinical practice, but they are urgently needed for diagnosis, prognosis, patient stratification in clinical trials and monitoring of drug effects.3 The most promising biomarkers in ALS are the light chain and phosphorylated heavy chain of neurofilaments (NFL and pNFH, respectively), cytoskeletal proteins of large myelinated axons of neurons and therefore axonal impairment markers.4 NFL and pNFH are elevated in the cerebrospinal fluid (CSF) of patients with ALS relative to controls, with diagnostic sensitivities and specificities >80%; they also correlate with disease progression rate and survival.5–7 Likewise, blood NF levels are higher in ALS in comparison to controls, but to date they have not been studied in a systematical comparison between ALS and several neurological control groups.8–11 Therefore, we evaluated the usefulness of serum NFL in the diagnosis of ALS, as well as its role as prognostic biomarker and its stability over time.
Methods
Participants and clinical characterisation
This prospective longitudinal study included 283 patients investigated in the Department of Neurology of Ulm University Hospital, Germany, between 2010 and 2016. Patients were subdivided as follows: 124 patients (74 (59.7%) male (M) and 50 (40.3%) female (F)) with ALS; 50 patients (23 (46%) M and 27 (54%) F) admitted to a neurological inpatient clinic but without a final diagnosis of degenerative or inflammatory central nervous system (CNS) disease (non-neurodegenerative controls); 44 patients (32 (72.7%) M and 12 (27.3%) F) with conditions included in the differential diagnosis of ALS (disease controls); 20 patients (11 (55%) M and 9 (45%) F) with FTD; 20 patients (8 (40%) M and 12 (60%) F) with Alzheimer’s disease (AD); 19 patients (12 (63.2%) M and 7 (36.8%) F) with Parkinson’s disease (PD); and 6 patients (4 (66.7%) M and 2 (33.3%) F) with Creutzfeldt-Jakob disease (CJD).
Patients with ALS were selected according to availability of blood samples and MRI examinations taken at the same time points. Patients of all other disease categories were selected according to a random criterion.
Patients with ALS had a diagnosis of definite or probable ALS according to the revised El Escorial criteria12; among them, four also had concomitant FTD. Disease severity was expressed by the score on the Revised ALS Functional Rating Scale (ALSFRS-R),13 which was measured at sampling for 97 patients and enabled calculation of progression rate as follows: (48−ALSFRS-R score at the time of sampling)/months elapsed between disease onset and sampling.14 For 38 patients with ALS the date of death was known. All patients with ALS underwent mutation screening for the two most common ALS-causing genes, that is, C9orf72 and SOD1. Five patients (4%) carried a pathogenic hexanucleotide repeat expansion in C9orf72 and three (2.4%) carried SOD1 mutations; further three patients had a positive family history of ALS but carried no mutations in either of the two genes. In 29 patients (20 M and 9 F), NFL concentrations were also measured on a second serum sample obtained later in the disease course.
The FTD group comprised the following patients: 12 with behavioural-variant FTD (bvFTD), among whom two carried a hexanucleotide repeat expansion in C9orf72; 4 with non-fluent-variant primary progressive aphasia (nfvPPA); 2 with semantic-variant PPA (svPPA); and 2 with PPA without further characterisation.
Sample collection and analysis
Serum was obtained from peripheral blood by centrifugation (800 g, 5 min) and stored within 2 hours at −80°C. Biobanking was conducted according to current recommendations.3
Serum NFL concentrations were measured with the single molecule array (Simoa) platform provided by Quanterix (Lexington, MA, USA).15 Measurements were performed on the fully automated instrument HD-1 Analyzer (Quanterix)16 using the NF-L Beta kit from Quanterix, which employs an anti-NFL monoclonal antibody produced by UmanDiagnostics (Umeå, Sweden). The interassay coefficients of variation (CV) were <15%. Clinical information, including diagnostic category of any sample, was not available to the performers of the measurements.
Assessment of disease stage by diffusion-tensor imaging
For patients with ALS, disease pathological stage was assessed according to the fibre tract-based diffusion-tensor imaging (DTI) protocol developed at our centre,17 using a 3 T scanner (n=30) or a 1.5 T scanner (n=94). The different stages describe which fibre tracts are affected in an individual patient with ALS assuming a sequential progression of pathology: the corticospinal tract (stage 1), the corticorubral and corticopontine tracts (stage 2), the corticostriatal pathway (stage 3) and the proximal portion of the perforant path (stage 4). Patients who could not be classified by DTI (eg, due to movement artefacts) were grouped into stage 0.
Statistical analysis
Two-tailed unpaired Mann-Whitney U test and Kruskal-Wallis test were used to determine differences in serum NFL levels or other quantitative variables between two or more groups, respectively. Dunn’s multiple comparison test was performed following Kruskal-Wallis test in case of significant differences. Sensitivity and specificity accompanied by their 95% CIs, as well as positive and negative predictive values (PPV and NPV, respectively) accompanied by their 95% CIs, were calculated for different cut-off levels of serum NFL. Varying sensitivity and specificity according to different cut-offs were plotted on the receiver operating characteristic (ROC) curve. The optimal cut-off levels were chosen as those maximising the Youden index (sensitivity+specificity–1). Correlation between parameters was calculated by Spearman rank correlation coefficient (rs). The Kaplan-Meier method was applied for estimating survival curves, which were then compared by means of the log rank test; censoring was applied for patients who were alive at last follow-up. Wilcoxon matched-pairs signed-rank test was used to compare pairs of basal and follow-up serum NFL measurements. The level of significance for statistical tests was set at 0.05. The program Prism V.7 (GraphPad Software, La Jolla, CA, USA) was used to perform statistical calculations.
Results
Patient characteristics
The characteristics of the study population are summarised in table 1; table 2 shows the single diagnoses within the disease control group. The ages of the groups differed significantly (p<0.0001). Post hoc comparison showed that patients with ALS did not differ in age from non-neurodegenerative controls, disease controls, and patients with FTD, PD and CJD; however, they were younger than patients with AD (p=0.0005). Both patients with AD and PD were also significantly older than non-neurodegenerative controls (p<0.0001 and p=0.0026, respectively).
Demographic characteristics and serum NFL levels of the different diagnostic groups
Demographic characteristics and serum NFL levels of disease controls
Among patients with ALS, median age of onset was 60 years (range, 26–74 years). Site of onset was bulbar in 39 (31.5%) cases and spinal in 85 (68.5%) cases. Median disease duration at sampling was 13 months (range, 2–145 months). Median ALSFRS-R score at sampling was 43 (range, 24–48; n=97) and median progression rate was 0.375 points/months (range, 0–6 points/month). Seventy-five (60.5%) of the 124 patients with ALS were not being treated with riluzole at the time of blood sampling whereas 49 (39.5%) were taking the drug. Median survival was 27 months (range, 10–52 months; n=38). Among patients who were alive at last follow-up, median disease duration at last follow-up was 28.5 months (range, 7–155 months; n=86).
Comparison of NFL levels between ALS and other categories and establishment of a cut-off for diagnosis
NFL levels differed significantly among the diagnostic categories (p<0.0001). Post hoc analysis shows that in ALS the levels were higher than in non-neurodegenerative controls (p<0.0001), disease controls (p<0.0001), AD (p=0.0006), FTD (p=0.0063) and PD (p<0.0001), whereas ALS and CJD did not differ (p>0.9999) (figure 1A).
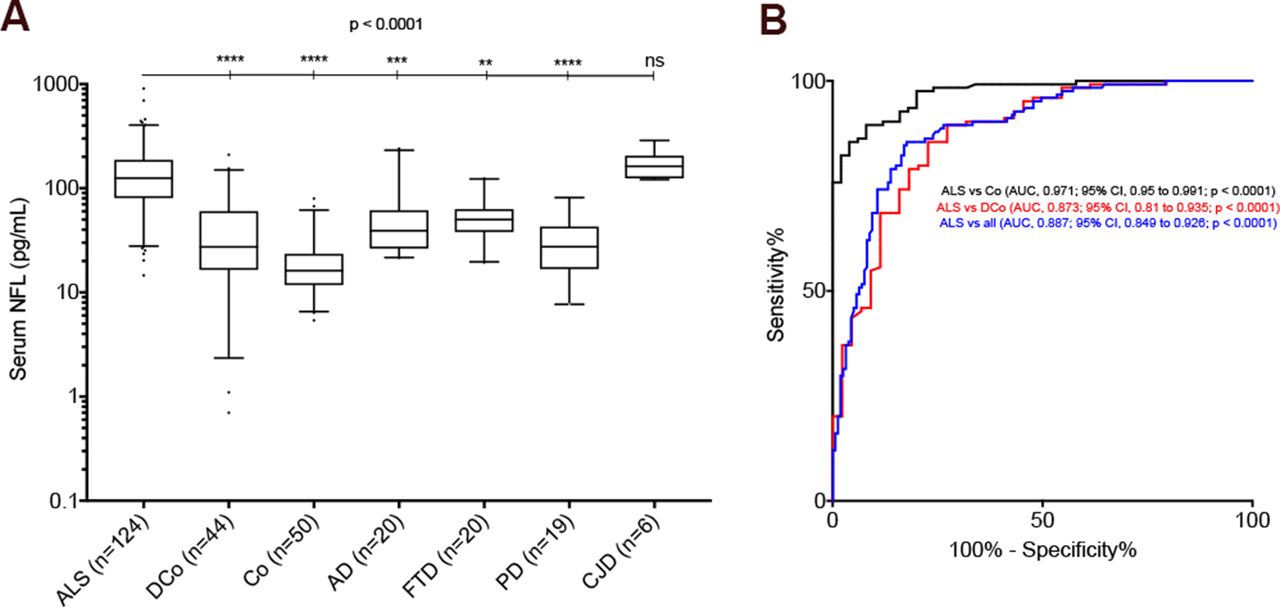
Serum neurofilament light chain (NFL) in the diagnosis of ALS. (A) Serum NFL levels in the different diagnostic categories. NFL levels are plotted on a 10-logarithmic scale. Given are the median concentrations, 25th and 75th percentiles, and 5% and 95% whiskers. Points represent values below 5% percentile and above 95% percentile. Statistically significant differences are marked with ****p<0.0001, ***p<0.001 or **p<0.01. (B) Receiver operating characteristic (ROC) curves of serum NFL for discrimination between ALS and non-neurodegenerative controls, ALS and disease controls, and ALS and all other diagnostic categories considered together.
A cut-off level of 49 pg/mL discriminated between ALS and non-neurodegenerative controls with 89.5% sensitivity (95% CI 82.7% to 94.3%), 92% specificity (95% CI 80.8% to 97.8%), 96.5% PPV (95% CI 91.5% to 98.6%), 78% NPV (95% CI 67.8% to 85.6%) and 0.971 area under the ROC curve (AUC) (95% CI 0.95 to 0.991; p<0.0001). More importantly, a cut-off of 62 pg/mL discriminated between ALS and disease controls with 85.5% sensitivity (95% CI 78% to 91.2%), 77.3% specificity (95% CI 62.2% to 88.5%), 91.4% PPV (95% CI 85.9% to 94.8%), 65.4% NPV (95% CI 54.5% to 74.9%) and 0.873 AUC (95% CI 0.81 to 0.935; p<0.0001). The same cut-off of 62 pg/mL resulted in 85.5% sensitivity (95% CI 78% to 91.2%) and 81.8% specificity (95% CI 74.9% to 87.4%) in discriminating between ALS and all other categories considered together, with 78.5% PPV (95% CI 72.3% to 83.7%), 87.8% NPV (95% CI 82.4% to 91.8%) and 0.887 AUC (95% CI 0.849 to 0.926; p<0.0001) (figure 1B).
Correlation between age and NFL levels
In the non-neurodegenerative control group a moderate positive correlation between age and serum NFL level was observed (rs=0.5307; 95% CI 0.2884 to 0.7092; p<0.0001). This held true also for AD (rs=0.578; 95% CI 0.169 to 0.817; p=0.0076), PD (rs=0.466; 95% CI 0.001 to 0.766; p=0.0442) and disease controls (rs=0.3754; 95% CI 0.07937 to 0.6106; p=0.012), but not for patients with FTD (p=0.9723), CJD (p=0.2417) or, most importantly, ALS (p=0.4865).
NFL levels in relation to ALS patient characteristics
Serum NFL levels did not differ significantly between patients with bulbar and with spinal onset (n=39 and n=85, respectively; p=0.1850). Patients with ALS-FTD displayed a median serum NFL level higher than those with ALS alone (290.5 and 124 pg/mL, respectively), but the difference did not reach statistical significance (p=0.0759); however, the size of the ALS-FTD group was very small (n=4).
Serum NFL levels correlated negatively with disease duration from onset to sampling (rs=−0.3534; 95% CI −0.5026 to −0.1837; p<0.0001) (figure 2A), most likely as a reflection of the positive correlation with disease progression rate (rs=0.3359; 95% CI 0.1404 to 0.5062; p=0.0008) (figure 2B), as more aggressive disease courses are expected to bring patients earlier to medical attention; indeed, disease duration from onset to sampling and progression rate correlated negatively with one another (rs=−0.5222; 95% CI −0.657 to −0.3551; p<0.0001). In agreement with this, patients sampled within 6 months from disease onset (n=20) showed higher serum NFL levels than the rest of the cohort (n=104; median, 221.5 and 114 pg/mL, respectively; range, 34.5–460 and 14.6–908 pg/mL, respectively; p=0.0002), and those of them for whom the ALSFRS-R score was calculated at sampling (n=15) also had higher progression rates than the rest of the cohort (n=82; median, 0.75 and 0.36 points/month, respectively; range, 0–6 and 0–2.25 points/month, respectively; p=0.0025). Patients with serum NFL above the median (125 pg/mL) had a shorter survival than patients with NFL≤125 pg/mL (p=0.0054), with an HR of 2.392 (95% CI 1.236 to 4.63) (figure 2C). Serum NFL levels did not correlate with absolute ALSFRS-R score at sampling (p=0.1284) and were not associated with pathological stage as assessed by DTI (p=0.872) (figure 2D).
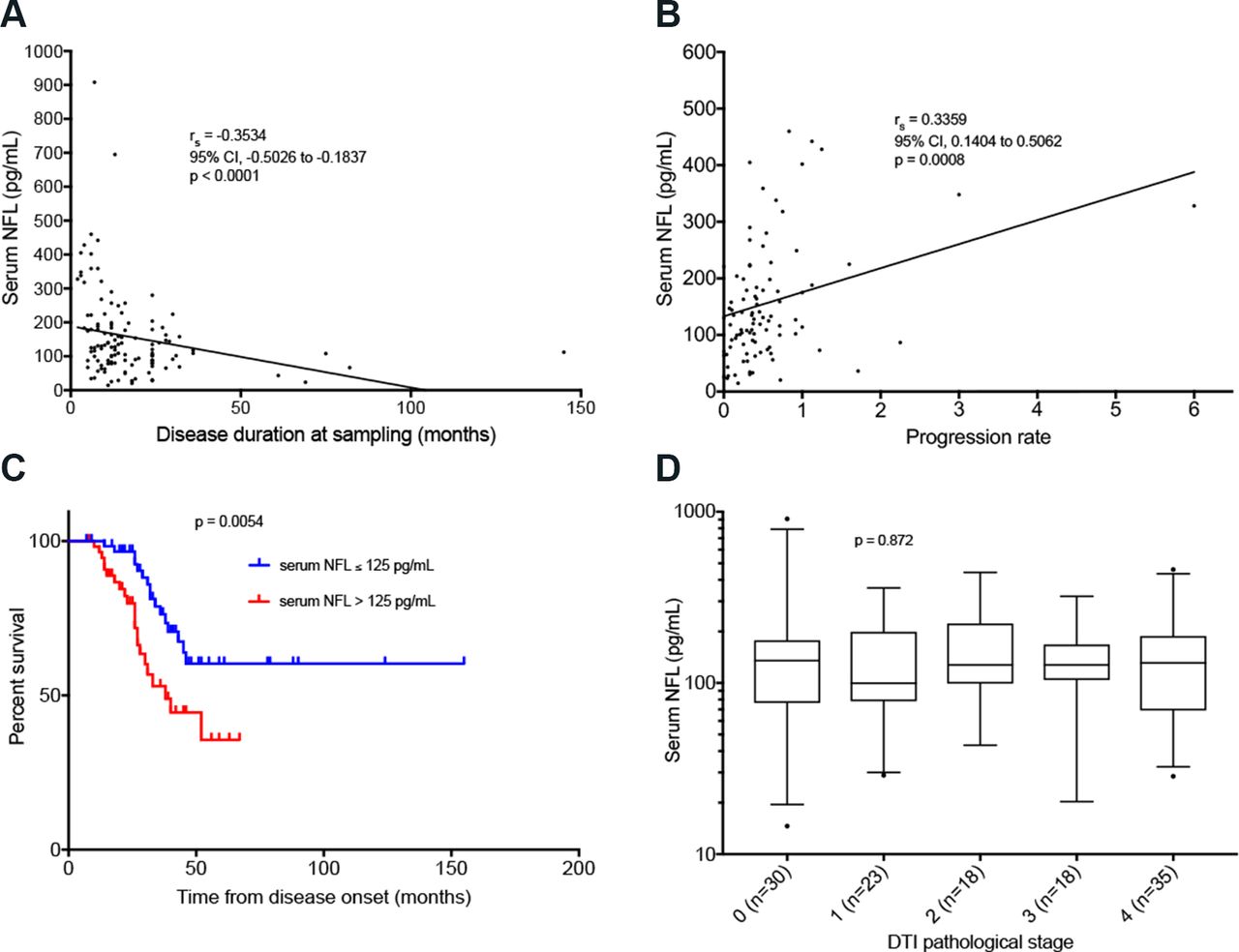
Serum NFL and disease parameters in amyotrophic lateral sclerosis (ALS). (A) Correlation between disease duration at sampling and serum NFL levels. (B) Correlation between progression rate and serum NFL levels. (C) Survival curves for patients with serum NFL levels ≤ median (125 pg/mL) and >125 pg/mL. Vertical ticks represent censored data. (D) Serum NFL levels in patients with different DTI pathological stages. NFL levels are plotted on a 10-logarithmic scale. Given are the median concentrations, 25th and 75th percentiles, and 5% and 95% whiskers. Points represent values below 5% percentile and above 95% percentile. DTI, diffusion-tensor imaging; NFL, neurofilament light chain.
Serum NFL levels did not differ between patients with a C9orf72 repeat expansion, patients with SOD1 mutations and patients negative for both (p=0.7656). NFL also did not differ between patients already taking and those not taking riluzole at the time of blood sampling (p=0.8736).
Follow-up NFL levels
The 29 patients who underwent a second blood sampling later in the disease course were composed of 9 patients with bulbar onset and 20 with spinal onset. Median age at sampling was 64 years (range, 35–71 years). Median disease duration at first sampling was 16 months (range, 5–69 months). Median interval between first and second sampling was 8.1 months (range, 4–54.9 months). They had a median basal serum NFL level of 83.4 pg/mL (range, 14.6–402 pg/mL) and a median follow-up level of 85.5 pg/mL (range, 22.4–591 pg/mL). The variations in NFL levels from first to second sample for the 29 patients ranged from −69.3 to +189 pg/mL (median, −0.1 pg/mL). Hypothesising linear trajectories of increase or decrease of serum NFL levels over time, we calculated from measured follow-up NFL levels the expected levels after a normalised time interval of 8 months from first sampling (ie, a time approaching the median interval of 8.1 months between basal and follow-up samples). This resulted in a median follow-up level of 93.7 pg/mL (range, 16.7–553.2 pg/mL). In this case, the variations in NFL levels from first to second sample ranged from −62.4 to +156 pg/mL (median,+0 pg/mL) (figure 3A). For 28 of the 29 patients, basal serum NFL levels ranged from 14.6 to 198 pg/mL and follow-up levels ranged from 22.4 to 186 pg/mL (with calculated NFL levels after 8 months ranging from 16.7 to 223 pg/mL). One further patient started from a basal NFL level of 402 pg/mL and reached a level of 591 pg/mL after 10 months (from which a time-normalised level of 553.2 pg/mL after 8 months was calculated).

{kind=link}
{kind=link}
{kind=link}
Follow-up serum NFL levels. (A) Basal serum NFL levels and calculated follow-up levels after a normalised time of 8 months from basal sampling. (B) Variations from basal serum NFL levels at different time points after basal sampling. The table depicts variations–expressed as mean with 95% CI–for patients whose follow-up samples were taken less than 5 months after the first sample (n=5), between 5 and 7 months after the first sample (n=8), between 7 and 12 months after the first sample (n=7) and more than 12 months after the first sample (n=8). The outlier described in the text was removed from the representation. NFL, neurofilament light chain.
Comparison of the pairs of basal and time-normalised follow-up measurements resulted in no statistically significant differences between the two sets (Wilcoxon matched-pairs signed-rank test, p=0.7213) and demonstrated the strong positive correlation between basal and follow-up levels (rs=0.8773, p<0.0001), suggesting stability of the biomarker over time in individual patients (figure 3B). This held true also when separate analyses were conducted for patients divided into upper and lower 0.5 quantiles according to basal NFL level, disease duration at first sampling, ALSFRS-R score at first sampling and progression rate at first sampling (p>0.05 in the Wilcoxon matched-pairs signed-rank test in all comparisons and presence of strong positive correlation between basal and follow-up levels with p<0.05 in all comparisons). Basal and follow-up serum NFL levels also did not differ when considering separately patients who were already taking riluzole at the time of blood sampling (Wilcoxon matched-pairs signed-rank test, p=0.8984; rs=0.7902, p=0.0017) and patients who were not taking riluzole (Wilcoxon matched-pairs signed-rank test, p=0.6869; rs=0.9167, p<0.0001).
Discussion
Our findings indicate that serum NFL levels are higher in patients with ALS in comparison to non-neurodegenerative controls, patients with conditions included in the differential diagnosis of ALS and patients with other neurodegenerative diseases (AD, FTD and PD), and demonstrate that serum NFL can serve as diagnostic biomarker for ALS. Importantly, this enabled us to establish a cut-off level of serum NFL for the diagnosis of ALS. In ALS, serum NFL is associated with progression rate and survival but not with pathological stage, and it is generally stable over the disease course, as indicated by a recent report.18
The high levels of NFL in CSF and serum in ALS seem to be due to release from impaired axons rather than to increased neuronal production, as NFL has been demonstrated to be reduced both at mRNA and at protein level in the spinal cord of patients with ALS.19 20 However, it is conceivable that alterations of NFL metabolism play a role in ALS pathogenesis, especially considering that TDP-43, the hallmark protein of ALS, interacts directly with NFL mRNA,21 and mutations in its gene TARDBP result in altered axonal transport of NFL mRNA.22 One might even speculate that the release of NFL is an active process aiming to restore impaired axonal transport, given that removal of the heavily phosphorylated NF tail domains has been shown to slow ALS progression in SOD1-mutant mouse models.23 Such an assumption would explain why NFL levels are stable over time after a sudden initial rise at disease onset.11 24 On the other hand, the marked increase of NFL observed in CJD is possibly due to massive neuronal destruction, analogous to what happens for tau in the same disease.25 This time course of NF elevation in ALS was investigated in a study conducted by our group on carriers of mutations in SOD1, C9orf72, TARDBP and FUS genes, demonstrating that pNFH in CSF and NFL in CSF and serum are normal in the presymptomatic stage and rise soon after symptom onset.24 The findings of that study, however, have to be interpreted with the caveat that it was a cross-sectional study in which the expected age of onset of presymptomatic carriers of gene mutations was determined based on parental age of onset. Therefore, a future study on presymptomatic carriers of pathogenic gene mutations conducted in a longitudinal prospective way would be more informative and could add invaluable information in the field of ALS biomarkers and in the study of ALS pathogenesis.
Differently from what has been reported for CSF, we could not find a significant difference in serum NFL values between AD and FTD.26 This might be caused by the lower number of patients with AD and FTD in our cohort; moreover, our patients with FTD might be at an earlier disease stage with less brain atrophy.
The diagnostic performance of serum NFL in ALS is similar to that of CSF NFs in ALS,5 and to that of the three well and long-established CSF biomarkers for AD (ie, A-beta 1–42, total tau and phosphorylated tau, which have become part of the clinical and diagnostic criteria for this disease and are routinely used internationally in the diagnostic workup of patients with cognitive impairment) when they are considered individually,27 and is not much inferior to that of the three markers measured in combination.28–30 The AUCs for the three AD CSF biomarkers with respect to their ability to detect AD pathological changes in the brain are comparable to those obtained with serum NFL in our study.31 For these reasons, we think that serum NFL deserves consideration for introduction into clinical practice and ALS diagnostic criteria. Moreover, it should be considered that our work aims at mimicking the real clinical situation in which ALS has to be differentiated not from the virtual category of normal controls, but rather from the much more relevant categories of other neurological patients, especially those with conditions included in the differential diagnosis of ALS itself. All disease controls in our cohort were actually patients referred to our centre with an initial clinical suspicion of ALS. These considerations make the diagnostic performance of serum NFL as emerging from our investigation even more interesting. Finally, it should be taken into account that our study is a prospective one and, as such, no specific clinical selection was performed on the cohort of patients with ALS (except from that imposed by availability of an MRI study), with patients from the other categories being selected using a random criterion. Therefore, our cohort reflects the real-world heterogeneous population of ALS and other patients evaluated at a neurological centre.
Despite the limitation given by the small numbers of patients in the single categories of disease controls, our finding of normal serum NFL levels in patients with fasciculations without ALS and in patients with hereditary spastic paraparesis (HSP) is an encouraging pilot result because of the clinical relevance of discriminating between ALS and these conditions. In HSP, NFL is probably not raised because of the very slow rate of degeneration of the corticospinal axons in this disease or because of the existence of a different pathophysiological process. On the other hand, a caveat about use of serum NFL for ALS diagnosis is represented by its consistently high levels in CJD: this is in agreement with recent data32 and should be taken into consideration in the rare cases of CJD presenting with features of MND.33 As regards the single case of limb-girdle muscular dystrophy (LGMD) with a high serum NFL value, it should be noted that some cases of LGMD are characterised by brain involvement represented by white matter hyperintensities which can be extensive, sometimes with accompanying neuropsychological deficits.34 It is, therefore, possible that in this case the elevation of serum NFL reflects underlying damage of the cerebral white matter, as suggested by studies reporting a correlation between CSF NFL and white matter hyperintensities.35
The very small numbers of components of single categories of the disease control group are due to the single-centre nature of our study and to our aim to consider only cases within the differential diagnosis of ALS. We think that it would be very informative to collect in the future larger and more homogeneous cohorts of disease controls or ideally of ALS mimics stricto sensu, most practically through a multicentre effort, in order to evaluate more precisely the diagnostic performance of serum NFL in differentiating ALS from selected categories of differential diagnoses.
Measurement of serum NFL in ALS diagnosis could prove useful in the future as a screening test in selected at-risk populations, for example, patients with a family history of ALS, and/or as an early diagnostic test in patients reporting symptoms with recent onset and limited extent and not fulfilling the criteria for ALS diagnosis.11 This could apply also to patients presenting only with fasciculations, in whom finding an elevated serum NFL level could prompt a fast track for referral to an ALS centre for further evaluation. As demonstrated by an American study on 304 patients with ALS, the median delay between symptom onset and diagnosis of ALS is 11.5 months, at least half of patients initially receive an alternative diagnosis before the correct diagnosis of ALS is made, and each patient is seen on average by three different physicians before definitive diagnosis.36 As CSF and serum NFs seem to rise soon after symptom onset in ALS,24 NF levels are already high in patients with a disease duration of less than 6 months, and do not differ between El Escorial diagnostic categories,11 early finding of raised levels in conjunction with new diagnostic criteria37 could accelerate the diagnostic workup resulting in reduction of diagnostic delay; this would enable earlier institution, and therefore possibly higher efficacy, of neuroprotective therapies. However, we acknowledge that more robust data from larger and more homogeneous cohorts would be needed to support this use of serum NFL as an early screening test. In general, measurement of serum NFL would be more valuable in contexts were lumbar puncture is not routinely performed or is risky for medical reasons, impeding measurement of CSF NFs. Indeed, serum NFL could be considered as a valid substitute of CSF NFs in reflecting axonal degeneration and therefore pointing to the presence of ALS. This would be particularly valuable in cases where diagnostic doubt exists: although for the experienced ALS neurologist ALS diagnosis is in most cases straightforward, the diagnostic process is still problematic in a minority of patients,38 also because of the clinical heterogeneity of the disease.39 40 It would be highly informative to investigate the value of NF measurement in a specific cohort of patients with a challenging diagnosis, especially in order to determine to what extent the result of this test would influence or change the diagnosis, analogous to studies performed on amyloid positron emission tomography examination in cases of dementia with conflicting results on investigations for AD (eg, non-conclusive CSF results).41 Furthermore, in a public health and organisation perspective, it should be considered that–notwithstanding the progressive homologation of healthcare measures, especially through adoption of common international guidelines–measurement of serum NFL could be performed with slightly different criteria and aims in the context of different healthcare systems and organisational realities.
Our results show a lack of association between serum NFL and ALS pathological stage as defined by DTI MRI measurements of the integrity of relevant white matter tracts of the brain. While some authors have reported an association between CSF NFs and the number of body segments showing upper and lower motor neuron involvement42 or a correlation between CSF NFL and MRI measures of degeneration of the corticospinal tract,43 our results support the view that NF levels reflect the rate of motor neuron degeneration, that is, the biological aggressiveness of the disease (and therefore the rate of clinical deterioration), rather than its anatomical extent (and the clinical stage),5 being already high in patients with recent onset of symptoms and not differing between El Escorial diagnostic categories.11 This is also in agreement with stability of serum NFL over time,18 which seems to reflect the linear progression of clinical deterioration in ALS.44 However, we acknowledge that our finding of stability of serum NFL in the disease course is based on analysis of a small subcohort of patients and should therefore be interpreted with caution.
Given its correlation with disease progression rate, its independence from disease stage, its stability over disease course and ease of accessibility through a blood draw, serum NFL could prove useful in the future as prognostic biomarker (especially considering that prognostic information in ALS is still based mainly on traditional clinical data),45 and find an application in the field of clinical trials. In the latter case, one can speculate that serum NFL could be used for patient stratification, demonstration of pharmacological target engagement and/or detection of drug effects, possibly earlier and with higher sensitivity than allowed by current clinical parameters.46 However, we acknowledge that our results are very preliminary and do not still currently allow to consider serum NFL as a reliable tool in the field of clinical trials. Moreover, pertaining to potential use of serum NFL as a marker of drug effect, more laboratory research on animal models is needed in order to validate the hypothesis of a modification (ie, a lowering) of NFL levels in response to a pharmacological intervention targeting mechanisms of motor neuron degeneration. Finally, the potential usefulness of serum NFL measurement as a resource for clinical trials should be investigated in the real-world context of a trial itself.
Acknowledgments
We are thankful to Stephen Meier for his excellent technical assistance in the measurements, and to Dagmar Schattauer, Sandra Hübsch, Mehtap Bulut and Alice Pabst for their invaluable biobanking work. We thank the patients and their families for participation in this study.
References
Footnotes
Contributor Study conception and design: MO, ACL, FV. Acquisition and analysis of data: FV, PS, JHW, JK, SH, JD, BM, HPM, MG, AEV, ACL, MO. Writing of the manuscript: FV, PS, MO. Critical revision of the manuscript: FV, PS, JHW, JK, PO, SH, HT, CAFvA, JD, EF, BM, HPM, MG, AR, AEV, VS, ACL, MO.
Funding The study was supported by grants from the German Federal Ministry of Education and Research (project FTDc 01GI1007A, MND-Net 01GI0704), the EU Joint Programme–Neurodegenerative Diseases network PreFrontAls (01ED1512), the German Research Foundation (VO 2028/1-1), the Foundation of the State of Baden-Wuerttemberg, the Thierry Latran Foundation, the ALS Association, the Virtual Helmholtz Institute ‘RNA Dysmetabolism in FTD and ALS’ and Boehringer Ingelheim Ulm University BioCenter.
Competing interests None declared.
Patient consent Obtained.
Ethics approval Ethics Committee of Ulm University (proposal number 20/10, year 2010).
Provenance and peer review Not commissioned; externally peer reviewed.