Article Text

Abstract
Objective Early diagnosis of natalizumab-related progressive multifocal leucoencephalopathy (NTZ-PML) in multiple sclerosis has been deemed a major priority by the regulatory agencies but has yet to become a reality. The current paper aims to: (1) investigate whether patients with NTZ-PML pass through a prolonged presymptomatic phase with MRI abnormalities, (2) estimate the longitudinal PML lesion volume increase during the presymptomatic phase and (3) estimate the presymptomatic phase length and its impact on therapy duration as a risk stratification parameter.
Methods All Italian patients who developed NTZ-PML between 2009 and 2018 were included. The data of patients with available prediagnostic MRI were analysed (n=41). Detailed clinical and neuroradiological information was available for each participant.
Results (1) PML lesions were detectable in the presymptomatic phase in 32/41 (78%) patients; (ii) the lesion volume increased by 62.8 % for each month spent in the prediagnostic phase; (3) the prediagnostic phase length was 150.8±74.9 days; (4) PML MRI features were detectable before the 24th month of therapy in 31.7 % of patients in our cohort.
Conclusions Considering the latency of PML clinical manifestation, the presymptomatic phase length supports the usefulness of MRI surveillance every 3–4 months. Early diagnosis could prompt a better outcome for patients due to the relationship between lesion volume and JC virus infection. The insight from this study might also have an impact on risk stratification algorithms, as therapy duration as a parameter of stratification appears to need reassessment.
Statistics from Altmetric.com
Introduction
Progressive multifocal leucoencephalopathy (PML) is an opportunistic infection caused by the JC virus (JCV), emerging as a severe adverse event of natalizumab (NTZ), which is a monoclonal antibody that is effective in controlling the course of multiple sclerosis (MS).1–4
To date, the majority of research has focused on risk stratification with the aim of closely monitoring patients at high risk of developing PML.5–9 In this population, clinicians often prefer to interrupt NTZ therapy rather than address this potentially severe adverse event.10 11 Moreover, NTZ discontinuation is linked to MS pathology resumption, which occurs a few months after the end of the treatment.12 MS resumption can cause permanent cumulative disability and can be detrimental to the patient’s quality of life.13
According to the European Medicines Agency, early PML identification14 15 is a critical step in reducing mortality and residual disability.16–18 Early identification would be particularly useful for patients who cannot withdraw from NTZ treatment. As previous research has demonstrated that asymptomatic patients have smaller lesions17 and better outcomes compared with symptomatic patients,17 18 the aim of pharmacovigilance should be to identify PML MRI lesions before patients become symptomatic.19 This would also safeguard effective therapy continuation for patients with low to medium PML risk and promote withdrawal of NTZ only when strictly necessary.11
Critically, emerging data propose that MRI signs suggestive of PML may be evident up to 5 months before the onset of symptoms.16 17 19–21 However, this evidence is based primarily on anecdotal case reports19–21 or on a small subset of patients (8.4% of the total number of patients with PML17) diagnosed with PML but withdrawn from NTZ treatment while still asymptomatic.
Currently, there is a lack of data investigating if all or most of the PML patients pass through a prolonged presymptomatic phase with MRI abnormalities or whether PML lesion volume increases prior to clinical significance in those already receiving treatment with NTZ.
To investigate these issues, we retrospectively analysed brain MRI scans pre-PML and post-PML diagnosis in the Italian PML cohort. We aimed to identify the proportion of patients with PML lesions detectable in the presymptomatic phase and to estimate the rate of PML lesion volume increase during the presymptomatic phase.
Methods
Patients and data collection
The data of patients included in the Italian PML cohort18 22 23 up to May 2018 were retrospectively analysed. Clinical and MRI data of NTZ-treated patients were retrospectively collected from 36 Italian sites. Retrospective analysis of patients’ data was conducted in accordance with the ethical standards laid down in the 1964 Declaration of Helsinki and its subsequent amendments.
Patients were included in the study if they met the American Academy of Neurology (AAN) criteria24 for definite, probable or possible PML. As these criteria have recently been found to have suboptimal sensitivity for PML in a real world setting25 in the absence of detectable JCV copies in the cerebrospinal fluid (CSF), we followed recently proposed diagnostic criteria26 as follows: patients were included if they: (1) had a high risk of developing PML (positive serostatus and NTZ therapy length >12 months); (2) had no disease activity during NTZ treatment and presented at MRI with a new lesion highly suggestive of PML and the absence of lesion characteristics suggestive of other diseases27 and (3) the clinical and radiological longitudinal evolution of the patient was the one expected for PML (ie, the patients manifested clinical and radiological immune reconstitution syndrome 2–3 months after withdrawal of NTZ18 22).
All patients were tested with STRATIFY (an ELISA assay for the detection of JCV antibodies in human serum and CSF28), while data concerning JCV index were available for a few subjects (n=14). Relevant to the current study, the following features were available for this cohort: gender; age at MS onset; age at PML diagnosis; Expanded Disability Status Scale (EDSS29) prior to NTZ beginning, at PML diagnosis and at 12-month follow-up (M12); prior immunosuppressant use (mitoxantrone, methotrexate, azathioprine or cyclophosphamide); length of NTZ therapy; number of NTZ infusions; CSF JC viral copies/mL at PML diagnosis; clinical status at PML diagnosis (symptomatic or asymptomatic); and MRI scans at PML diagnosis. CSF samples were collected on suspicion of PML and sent to the National Institutes of Health Laboratory of Molecular Medicine and Neuroscience (Bethesda, Maryland, USA) or to the Unilabs Laboratory (Copenhagen, Denmark).
We defined the diagnostic MRI as the MRI performed concomitantly with the suspicion/diagnosis of PML. In symptomatic patients, the diagnostic MRI was performed when patients manifested a new symptom suggestive of PML. In asymptomatic patients, the MRI was performed during routine surveillance, and PML was suspected due to MRI findings. A lumbar puncture was performed immediately following the MRI in all cases.
Sites were contacted again in 2017 and asked for the MRIs taken prior to the diagnostic MRI (defined as the prediagnostic MRI). The prediagnostic images were acquired during routine surveillance while all patients were asymptomatic. The prediagnostic images of 37 patients were analysed, and information was extracted from retrospective radiological reports in four cases (see Results section). The following data were recorded: presence/absence of PML lesion in the MRI and time (in days) elapsed between the prediagnostic and the diagnostic MRIs.
Although brain MRI scans were based on local protocols, T1-weighted, T2-weighted, Fluid-attenuated inversion recovery (FLAIR) and Diffusion weighted images (DWI) sequences were present for each patients. T1-weighted sequences with contrast enhancement were performed in the majority of patients during the diagnostic MRI (95.12% of patients) but not during the prediagnostic MRI (9.75% of patients). The diagnostic and the prediagnostic MRIs were independently analysed retrospectively by two expert neuroradiologists (SG and MC). All lesions considered to be PML were identified in consensus according with shared neuroradiological criteria,24 27 and lesion dissemination was scored as unilobar, multilobar or widespread.30 To verify PML lesion identification, the raters also reviewed the preceding and subsequent MRI scans.26
Lesion volume calculation
Prediagnostic and diagnostic lesions were traced on the T1-weighted template MRI scan from the Montreal Neurological Institute provided with the MRIcron software31 32 (available at http://www.mricro.com/mricron). Superimposing each patient’s lesion onto the standard brain enabled the estimation of the total brain lesion volume (in cubic millimetres) removing intersubject variability in total head size; this strategy also allowed us to remove potential bias due to different acquisition parameters at each site.
Statistical analysis
Demographic and clinical features of patients with and without prediagnostic MRIs were compared. The same features were also compared between patients with and without PML lesions at the prediagnostic MRI. Variables were analysed by means of χ2 test or Mann-Whitney U test depending on whether the variables were dichotomous or continuous.
The percentage of patients with and without apparent PML lesions in the prediagnostic MRI was computed. In order to estimate how long the infection had been detectable before symptom onset, the time elapsed (in days) between the prediagnostic and diagnostic MRIs was calculated: the average length and SD are presented. The time elapsed from PML diagnosis to symptom onset was added only for patients that were asymptomatic at diagnosis.
Furthermore, for patients with a positive prediagnostic MRI, the length of NTZ therapy at PML insurgence was calculated by subtracting the months elapsed between prediagnostic and diagnostic MRIs from the months of therapy duration at PML diagnosis (therapy length at diagnosis (dTL)), so that iTD=dTD (months from prediagnostic to diagnostic MRI).
A mixed regression model with random intercept and random slope was used to estimate the mean volume change between prediagnosis and diagnosis. To test if inclusion of the random slope into the mixed model improved the goodness of fit, a likelihood ratio (LR) test was performed. The volume was log-transformed before application of the model. The analysis was adjusted to include previous immunosuppressant use, gender and age at PML onset into the mixed model. The interaction between previous immunosuppressant use and time was added to the model to assess if previous treatment with immunosuppressive drugs had an impact on volume increase. The mean change was expressed as volume percentage change for 1 month of prediagnostic phase. Stata (v.14) was used for the computation.
Finally, a partial correlation between lesion volume at PML diagnosis and disability increase between beginning of NTZ and 12-month follow-up (ΔEDSS), controlling for lesion localization, was performed to investigate the impact of lesion volume on clinical outcome (represented by the EDSS change between the beginning of NTZ and 12-month follow-up after PML onset). EDSS at the beginning of NTZ was used as a pre-PML baseline condition, as the patients in the current cohort were clinically stable during NTZ treatment.18 22
Results
The results are described in accordance with Strengthening the Reporting of Observational Studies in Epidemiology guidelines.33
The patients’ inclusion procedure are summarised in figure 1. All the included patients (n=54) were positive for the STRATIFY test sampled prior to PML onset. For the few subjects with a JCV index (n=14), the mean JCV index was 3.08±0.94 (median 3.1 (1.52–5.27)). At PML diagnosis, 43 out of 54 patients (79.62%) met the AAN criteria for definite PML, 2/54 (3.71%) for possible PML and 7/54 (12.96%) for probable PML. Two patients out of 54 (3.71%) were asymptomatic with no JCV copies in the CSF at PML diagnosis, but they met the most recently proposed criteria26; thus, their data were included in accordance with recent advances in PML knowledge.26 34

Flow diagram reporting the number of patients at each stage. Asterisk (*) denotes that at the prediagnostic MRI all the patients were asymptomatic. MRI+, lesion present in the prediagnostic MRI; MRI−, lesion absent in the prediagnostic MRI.
Patients whose prediagnostic scans were available (n=41, 75.9%) differed from patients whose prediagnostic scans were not available (n=13, 24%) in gender and age at PML diagnosis (table 1). Out of 41 patients with the prediagnostic MRI scans available, 32 (78.1%) were symptomatic and 9 (21.9%) were asymptomatic at PML diagnosis.
Demographic and clinical variables in patients with and without the prediagnostic image available. Number denotes row number (percentage) (A) and median (range) (B) Statistical significance was evaluated using χ2 (A) and the Mann–Whitney U test (B)
Prediagnostic lesions
Prediagnostic PML lesions were present in 26 of the 32 (81.2%) patients who were symptomatic at PML diagnosis and in 6 of the 9 (66.6%) patients who were asymptomatic at PML diagnosis. In total, PML lesions were detectable in the prediagnostic MRIs of 32 of the 41 (78.1%) patients. The information was extracted from a retrospective neuroradiological report in four cases, as the images were not shared with the authors. In all four cases, the neuroradiologists declared that they misinterpreted the emerging PML lesion as a new MS lesion. Figure 2 shows the prediagnostic and diagnostic lesions in two patients with NTZ-PML for exemplification purposes. Patients with a positive prediagnostic MRI did not differ from patients with a negative prediagnostic MRI (n=9, 21.9%) in any demographic or clinical variable at PML diagnosis (table 2). Of note, three deaths occurred in the positive prediagnostic MRI group, while no deaths occurred in the negative prediagnostic MRI group.

Lesion evolution from prediagnostic to diagnostic phase. The figure represents the prediagnostic and diagnostic lesions of two patients included in the Italian PML cohort. Every box in the upper line shows axial T2-weighted in the inferior line axial FLAIR. Upper line: prediagnostic MRI: smooth hyperintensity in left frontotemporal cortical region (red circle); diagnostic MRI: evolution of the left frontotemporal lesion with swallowing of the cortex; evidence of other focal lesions in left thalamic region in left cortical frontomesial region, another small lesion in right occipital pole, still with cortical location. Minimal oedema is present. Lower line: prediagnostic MRI: smooth cortical signal alteration in left temporoccipital and parietal region; diagnostic MRI: evolution with extension of both lesions in corticosubcortical regions. Sulcal effacement is present.
Presymptomatic phase length
The difference between the current approach and the approach used in previous literature is presented in figure 3. In the group of patients with a positive prediagnostic MRI, the mean time elapsed between prediagnostic and diagnostic MRIs was 150.8±74.8 days (5.2±2.5 months, range 1–11). In symptomatic patients, the length of the presymptomatic phase was 142.1±80.1 days (4.8±2.6 months, range 1–11). In asymptomatic patients, the length of the presymptomatic phase was 188.5±23.6 days (6.5±0.8 months, range 6–8), of which 122.5±28.2 days (4.3±1 months) were spent in the prediagnostic phase and 66±39 days (2.1±1.3 months) were spent in the postdiagnostic phase.
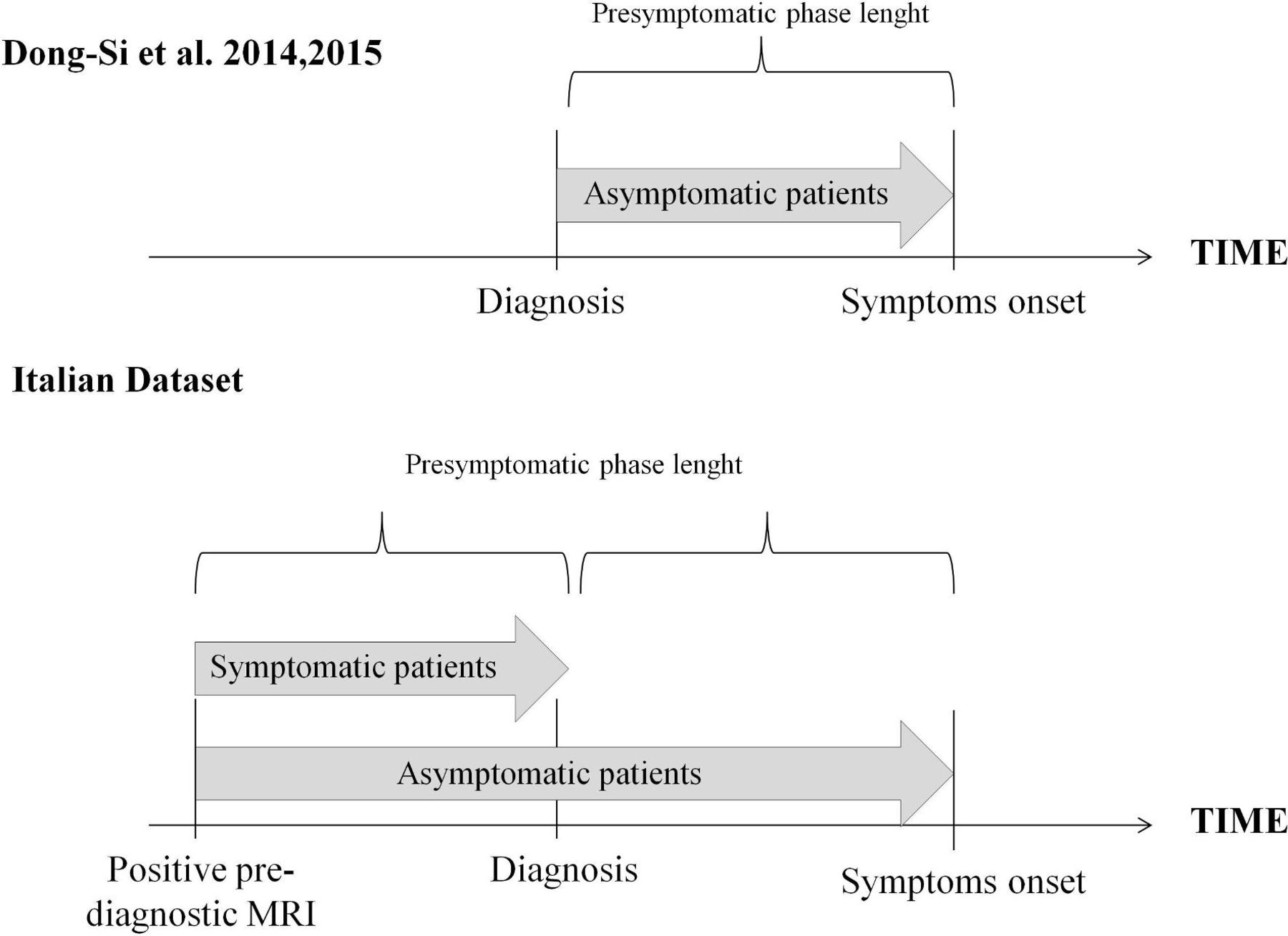
Presymptomatic phase length. The figure represents the presymptomatic phase length as previously calculated in literature17 (upper panel) and as it was calculated in the current paper (lower panel).
Demographic and clinical variables in patients with and without PML lesion in the prediagnostic MRI. Number denotes row number (percentage) (A) and median (range) (B)
NTZ therapy length recalculation
Of the 41 patients with a prediagnostic MRI available, the mean dTL was 43.9 months, and the median was 44 (12-89) months. The dTL did not reflect the therapy length at PML onset (oTL), which corresponded to a mean of 39.5 months and a median of 40 (5-86) months. Analysis of the dTL showed that eight of the 41 patients (19.5%) were diagnosed with PML before the 24th NTZ infusion. Furthermore, oTL showed that PML emerged before the 24th infusion in 14 of the 41 patients (34.1%). Finally, the dTL showed that 2 of the 41 patients (4.8%) were diagnosed with PML before the 12th month of therapy and the oTL identified PML emerging before the 12th month of therapy in 5 of the 41 patients (12.1%).
Lesion volume change kinetics
Four patients had only a neuroradiological report; thus, both their lesion dissemination and lesion volume could not be evaluated.
Unilobar lesions were more frequently present in prediagnostic MRIs (21/28, 75%) than in the diagnostic MRIs (5/28, 17.8%) (χ2=18.98, p<0.001).
The lesions in the 28 patients had a mean prediagnosis volume of 1527 mm3 (SD: 1564 mm3) with a median of 888 mm3 (IQR: 397–2634 mm3). At diagnosis, the same lesions in the 28 patients had a mean volume of 16 954 mm3 (SD: 22 427 mm3) and a median of 9000 mm3 (IQR: 2455–19925 mm3). The PML lesion volume was estimated to increase by 62.8% (95% CI 46% to 81%; p<0.001) per month between prediagnostic and diagnostic MRIs (figure 4). This percentage was adjusted for previous use of immunosuppressive drugs (p=0.04), gender (p=0.062) and age (p=0.33). Previous immunosuppressant use had no impact on volume change (interaction p=0.77). A model with random intercept and random slope was preferred (LR test p=0.05).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Lesion volume evolution from prediagnosis up to diagnosis. The figure represents the lesion volume evolution for each patient (blue line) and the overall evolution (red line).
Impact of PML diagnosis lesion volume on clinical outcome
The lesion volume at PML diagnosis was correlated with the outcome in all 41 patients in the cohort. The partial correlation between lesion volume at PML diagnosis and ΔEDSS was highly significant (r=0.515, p=0.001), suggesting that larger volume is related to a more severe increase in longitudinal disability.
Discussion
Through a retrospective reanalysis of MRI data from a sample of 41 patients with NTZ-PML, this study aimed to calculate the proportion of patients with PML lesions detectable in the presymptomatic phase and to estimate the longitudinal change in PML lesion volume.
The results are noteworthy. First, PML lesions were detectable in the prediagnostic MRIs of at least 78% of patients. Second, lesions were identifiable 5 months (on average) prior to the onset of symptoms (up to 11 months). Third, the results suggest that therapy length at PML diagnosis is not a precise risk parameter. Fourth, the longitudinal data revealed a lesion volume increase of 62.8% per month between the prediagnostic and diagnostic MRIs. Fifth, lesion volume at PML diagnosis strongly correlates with the clinical outcome at the 12-month follow-up.
As the majority of patients included in the Italian cohort were diagnosed with PML when manifesting a new symptom, the current finding of PML already being present in the prediagnostic MRI of 78% of cases suggests that the correct identification of PML is still very difficult, despite the available criteria to differentiate MS from PML lesions.27 However, the results also suggest that PML could have potentially been identified when most patients were still asymptomatic. This should be the aim of future research. Interestingly, as the percentage of asymptomatic patients in our cohort (21.9%) is higher than previously described (8.1%17 or 17.85%26), it is likely to suppose that our results may be generalised to prior PML cases. We were also able to estimate that PML onset may predate the onset of clinical symptoms by 5 months on average. This result is significant, as it provides experimental justification for the usefulness of MRI surveillance every 3–4 months in patients at high risk for PML.6 19 35 36 In asymptomatic patients only, previous research16 17 estimated the postdiagnostic/presymptomatic phase length by following the patients who discontinued NTZ therapy on PML suspicion until they developed PML symptoms. Our data enrich the literature due to a substantially different approach. Through the analysis of prediagnostic MRIs, we were able to determine the prediagnostic and presymptomatic phase length in the whole cohort (symptomatic and asymptomatic patients). To the best of our knowledge, this is the first study empirically demonstrating that PML symptoms might develop months after JCV replicates in the brain and forms a visible lesion.
Another noteworthy finding comes from the focus on six patients in our cohort who had a positive prediagnostic MRI in their third year of treatment. Through the reassessment of therapy length, we observed that PML onset could be traced back to the first 2 years of treatment in these patients. Since therapy length at PML diagnosis is one of the three key risk stratification elements for PML, this result may impact future PML research, as it shows that the stratification of risk algorithms5 6 8 might be biased. Indeed, therapy duration as a risk parameter might need to be reassessed, as the algorithm is based on NTZ therapy length at PML diagnosis, which differs from therapy length at actual PML onset. The actual interval of interest is the time to JCV infection, as recently suggested.19 Although it is not possible to know precisely when JCV spreads in the brain, the time of PML lesion appearance can be considered a proxy, as it is now known that PML lesion volume is associated with viral load.26 This knowledge should not lead to over-reliance on MRIs, which might compromise clinical vigilance.37 MRI is a powerful instrument for pharmacovigilance and could assist early diagnosis and timely withdrawal of NTZ when PML is suspected. However, clinical vigilance, meticulous observations of clinical progression and detection of JCV are of utmost importance for PML diagnosis and management. While a previous study26 provided evidence of a link between lesion size and viral load at PML diagnosis, the current paper provides evidence of the longitudinal evolution of the PML lesion(s) up to the time of diagnosis. Our data prove that lesions are smaller in the initial stage of viral infection, before spreading throughout the brain, supporting the idea that the lesions begin as small groups of infected regions that enlarge as viral infection proceeds.26 38 Whether this takes weeks or months has recently been identified as an area requiring further investigation.38 The longitudinal nature of the data analysed in the current study allowed us to provide a preliminary answer to this important question. Our data suggest that PML lesion volume increases by 62.8% per month between the prediagnostic and diagnostic MRIs, taking 5 months to become clinically symptomatic. Despite the lesion evolution rate differing between patients, our analysis did not identify any individual factor impacting lesion evolution, as the rate of volume increase was not influenced by the previous immunosuppressant use.
These data are of great relevance for patient prognosis. The ability to anticipate PML diagnosis by at least 5 months would critically affect both lesion volume and CSF viral load26 at withdrawal of NTZ. In addition, the likelihood of withdrawing NTZ while patients are still asymptomatic would also increase. As asymptomaticity and low viral load at PML diagnosis are known predictors of a good functional outcome,16–18 the current data suggest that the insightful use of MRI for pharmacovigilance coupled with meticulous training of neuroradiologists and efficient communication between neurologists and neuroradiologists has the potential to become the most effective way to positively influence patient prognosis. Indeed, our data revealed that all three deaths in Italy occurred in patients whose PML was not initially recognised. Critically, the data also showed a strong correlation between PML lesion volume at diagnosis and functional outcomes, thus clearly supporting the usefulness of early diagnosis. If the diagnosis had been made 5 months in advance, the lesion volume would have been smaller and the clinical outcome would have been better.
Limitations
In addition to the number of patients with PML included and the retrospective nature of this study, which are the main drawbacks of the current paper, an important limitation is that we did not analyse the impact of the JCV index. Unfortunately, as the JCV index has only been available since 2013, these data are missing for most patients (n=27 out of 41). An additional limitation is our inclusion of four patients who never had JCV copies detectable in the CSF. Two of these patients were also asymptomatic at PML diagnosis, hampering the classical diagnosis of PML. However, all four patients had lesion characteristics and a longitudinal evolution typical for PML. In addition, they developed the typical immune reconstitution around 2–3 months after withdrawal of NTZ.22 39 Asymptomatic and CSF-negative patients have also been included in recent papers,26 34 and a revision of the AAN diagnostic criteria24 has been proposed.19 25 26 Finally, this retrospective study included patients from different Italian sites. Thus, as in previous research,26 MRI acquisition protocols were not standardised, reflecting real-world pharmacovigilance clinical practice. However, we are confident that the identification of the lesions by consensus mitigated the bias introduced by the different scanning protocols. Furthermore, the manual lesion tracing method applied was specifically selected to reduce the effect of different acquisition parameters on lesion volume.
Conclusions
This study found that 78% of PML patients pass through a prediagnostic, presymptomatic phase. Viral infection could be identified by MRI 5.2 months prior to symptom onset. Furthermore, therapy duration should be reconsidered as a risk stratification element, due to risk stratification algorithms being based on therapy duration at PML diagnosis rather than on therapy duration at PML onset. Finally, lesion volume increases by 62.5% per month of diagnostic delay.
Despite the preliminary nature of this work, it justifies the usefulness of MRI surveillance every 3–4 months for high-risk patients. Neuroradiologists should be aware of the relevance of very small PML lesions and how to differentiate PML from MS lesions27 in asymptomatic patients.
Knowledge concerning PML treatment after onset,22 39–41 coupled with insights gained from this paper, provides critical elements to deal with patients who cannot be withdrawn NTZ.
This work was made possible by a remarkable collaboration between Italian neurologists and neuroradiologists who were proactively disposed to critically reassess the prediagnostic images of their own patients.
References
Footnotes
RC and SG contributed equally.
Collaborators Marta Altieri; Maria Pia Amato; Carlo Alberto Artusi; Fabio Bandini; Valeria Barcella; Antonio Bertolotto; Vincenzo Brescia Morra; Marco Capobianco; Guido Cavaletti; Paola Cavalla; Diego Centonze; Maurizia Chiusole; Marinella Clerico; Cinzia Cordioli; Giangaetano D’Aleo; Giovanna De Luca; Milena De Riz; Nicola De Rossi; Luciano Deotto; Luca Durelli; Mario Falcini; Claudio Ferrante; Ernesta Ferrari; Maria Luisa Fusco; Claudio Gasperini; Angelo Ghezzi; Luigi Grimaldi; Mario Guidotti; Alice Laroni; Alessandra Lugaresi; Lucia Moiola; Paola Naldi; Chiara Pane; Barbara Palmeri; Patrizia Perrone; Matteo Pizzorno; Carlo Pozzilli; Monica Rezzonico; Maria Rosa Rottoli; Marco Rovaris; Giuseppe Salemi; Marco Salvetti; Giuseppe Santuccio; Elio Scarpini; Edoardo Sessa; Claudio Solaro; Gianola Stenta; Giulietta Tabiadon; Carla Tortorella; Maria Trojano; Paola Valentino; Maira Rosa Rottoli.
Contributors CS, SG and RC had full access to all the data in the study and take responsibility for the integrity of the data and the accuracy of the data analysis. Study concept and design: CS, SG and RC. Acquisition, analysis or interpretation of data: all authors. Drafting of the manuscript: CS, LP and AS. Critical revision of the manuscript for important intellectual content: SG, MC, MPS and RC. Statistical analysis: AS, MPS and CS. Final approval of the version to be published: all authors.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests SC and AS have nothing to disclose. LP declares received consulting fees from Biogen and Novartis; speaker honoraria from Biogen, Genzyme, Novartis and Teva; travel grants from Biogen, Genzyme, Novartis and Teva; research grants from the Italian MS Society (Associazione Italiana Sclerosi Multipla) and Genzyme. LP also acts as member of steering committee Agenzia Italiana del Farmaco on natalizumab. RC received consulting fees from TEVA, Biogen, Merck Serono, Genzyme, Roche, GeNeuro, Novartis and Medday. MPC received speaker honoraria from Biogen. SG received speaker honoraria from Biogen and Novartis. RC received consulting fees from Novartis, Biogen and lecture fees and/or travel grants from Novartis, Biogen, Celgene, Genzyme and Sanofi-Aventis. These relationships are not related to the content in the manuscript. No other disclosures were reported.
Patient consent Not required.
Provenance and peer review Not commissioned; externally peer reviewed.