Article Text

Abstract
Background Increased rates of brain atrophy on serial MRI are frequently used as a surrogate marker of disease progression in Alzheimer’s disease and other dementias. However, the extent to which they are associated with future risk of dementia in asymptomatic subjects is not clear. In this study, we investigated the relationship between the Cardiovascular Risk Factors, Aging, and Dementia (CAIDE) risk score and longitudinal atrophy in middle-aged subjects.
Materials and methods A sample of 167 subjects (aged 40–59 at baseline) from the PREVENT-Dementia programme underwent MRI scans on two separate occasions (mean interval 735 days; SD 44 days). We measured longitudinal rates of brain atrophy using the FSL Siena toolbox.
Results Annual percentage rates of brain volume and ventricular volume change were greater in those with a high (>6) vs low CAIDE score—absolute brain volume percentage loss 0.17% (CI 0.07 to 0.27) and absolute ventricular enlargement 1.78% (CI 1.14 to 2.92) higher in the at risk group. Atrophy rates did not differ between subjects with and without a parental history of dementia, but were significantly correlated with age. Using linear regression, with covariates of age, sex and education, CAIDE score >6 was the only significant predictor of whole brain atrophy rates (p=0.025) while age (p=0.009), sex (p=0.002) and CAIDE>6 (p=0.017) all predicted ventricular expansion rate.
Conclusion Our results show that progressive brain atrophy is associated with increased risk of future dementia in asymptomatic middle-aged subjects, two decades before dementia onset.
Statistics from Altmetric.com
Introduction
It is now clear that pathological changes related to Alzheimer’s disease start decades before cognitive symptoms are evident.1 2 Dementia prevention or postponement strategies, such as lifestyle changes, should therefore begin as early as possible and there is a need to identify at risk individuals in whom such interventions are likely to have the greatest effect. Alzheimer’s disease shares risk factors with vascular disease such as hypertension and obesity, and these can be used both to identify individuals at risk and act as modifiable intervention targets.
A number of dementia risk scores have been suggested3 including the Cardiovascular Risk Factors, Aging, and Incidence of Dementia (CAIDE)4 score, which was developed in middle-aged community dwelling subjects.
Cross-sectional studies have found associations between raised midlife dementia risk scores and reduced brain volume.5–8 There has, however, been little reported research on the relationship between dementia risk score and subsequent brain atrophy. The aim of this study was to investigate to what extent an increased CAIDE score in midlife was linked to greater rate of brain atrophy over subsequent years. This is important to determine, since brain volume change is a frequently used objective biomarker of disease progression used in dementia studies, especially for Alzheimer’s disease. It is therefore important to know whether it may also be useful as a putative outcome marker for disease progression in midlife subjects.
Methods
Subjects
The protocol has been described in detail elsewhere.9 A total of 193 participants aged 40–59, of whom 168 had repeat MRI were recruited through multiple sources. Initially, they were identified from the dementia register database held at a London National Health Service (NHS) Trust, part of the UK NHS. This registry holds information on patients with dementia and cognitive impairment who have consented to be approached for clinical research and their carers (often offspring). Other participants were recruited via the Join Dementia Research website (https://www.joindementiaresearch.nihr.ac.uk/), through information about the study on the internet and public presentations. The study aimed to recruit approximately half of the subjects with a parental family history of dementia and half without. For those with a family history, the estimated time to dementia onset was on average 20 years, based on age of parental dementia onset.9
Dementia risk score
Dementia risk scores were calculated for each participant at baseline using the CAIDE score.4 This is a dementia risk score (DRS) composed of weightings by reference to the following variables: age, sex, education, systolic blood pressure, body mass index (BMI), total cholesterol, physical activity and apolipoprotein E (APOE) status. Scores vary from 0 to 18. We treated this as a binary variable, split according to the group median (DRS≤6). Family history of dementia was defined as positive if at least one parent had clinically diagnosed dementia and APOE4 status was regarded as positive for ≥1 ε4 allele.
Imaging
Participants underwent multimodal 3 T structural MRI on a single scanner (Siemens Verio) including volumetric T1-weighted scans (176 slices, 1.0×1.0 mm, 1.0 mm slice thickness, repetition time=2300 ms, echo time=2.98 ms, flip angle 9°). Scans were repeated after approximately 2 years on the same scanner using the same protocol.
Percentage brain volume change and ventricular enlargement between the two scans were determined using the FSL siena programme (https://fsl.fmrib.ox.ac.uk/fsl/fslwiki).10 Values were then divided by the time between scans to give rates per year. Total intracranial volume was calculated from the sum of grey matter, white matter and cerebrospinal fluid (CSF) segmentation done with SPM12 (http://www.fil.ion.ucl.ac.uk/spm). All output was manually checked to ensure correct brain segmentation and alignment of baseline/repeat scans.
Statistical analysis
Brain volume data and clinical variables were analysed with the Statistical Package for Social Sciences (SPSS V.19). Independent t-tests were used to compare groups for continuous variables and χ² test for categorical data. Pearson’s correlation coefficient was used to compare continuous variables. Linear regression was used to investigate predictors of brain atrophy rates. Residuals were checked by eye to verify normality, heteroscedasticity and absence of non-linear associations.
Consent and organisation of examinations
Participants were seen at the West London Cognitive Disorders Treatment and Research Unit. Blood was taken for APOE genotyping, with all members of the research and clinical teams remaining blind to the result. All participants provided informed written consent.
Role of the funding source
The sponsor had no role in study design, collection, analysis or interpretation of data, nor in the writing of the report or decision to submit the paper for publication.
Results
Of the 193 participants with T1 MR scans at baseline, 168 had a repeat scan. There were no significant differences between those with versus without a repeat scan in age (52.0 SD 5.4 vs 51.3 SD 5.4; t191=0.6, p=0.5), years of education (16.1 SD 3.4 vs 14.7 SD 3.1; t191=1.9, p=0.06), CAIDE score (5.9 SD 2.9 vs 5.7 SD 2.9; t189=0.4, p=0.7), sex (118/168 vs 17/25 female; χ2=0.1, p=0.8) or APOE genotype (64/166 vs 6/25 with ε4; χ2=2.0, p=0.16). However, those with repeat imaging were more likely to have a parent with dementia (89/168 (53%) vs 6/25 (24%); χ2=7.3; p=0.007).
One participant had marked ventricular shrinkage (−26%) between baseline and repeat scan. There were no obvious technical problems with this participant’s images. As this ventricular change was more than 3 SD below the mean (+3.6% SD 5.8), this subject was excluded from further analysis. Demographic details of the 167 participants included in the longitudinal analysis are shown in table 1.
Subject demographics
In univariate analyses, there were no significant differences in either ventricular enlargement or brain volume change rates between those with versus without a parent with dementia (table 2) or between those with versus without presence of the APOE ε4 allele. Age (table 3) was significantly associated with both ventricular enlargement and brain volume change, as was having CAIDE score >6. Males had greater rate of ventricular enlargement, but no difference in overall brain volume change.
Univariate comparison of annual percentage change in brain volume and percentage change of ventricle volume with demographic variables
Univariate correlations of annual percentage change in brain volume and percentage change of ventricle volume with demographic variables
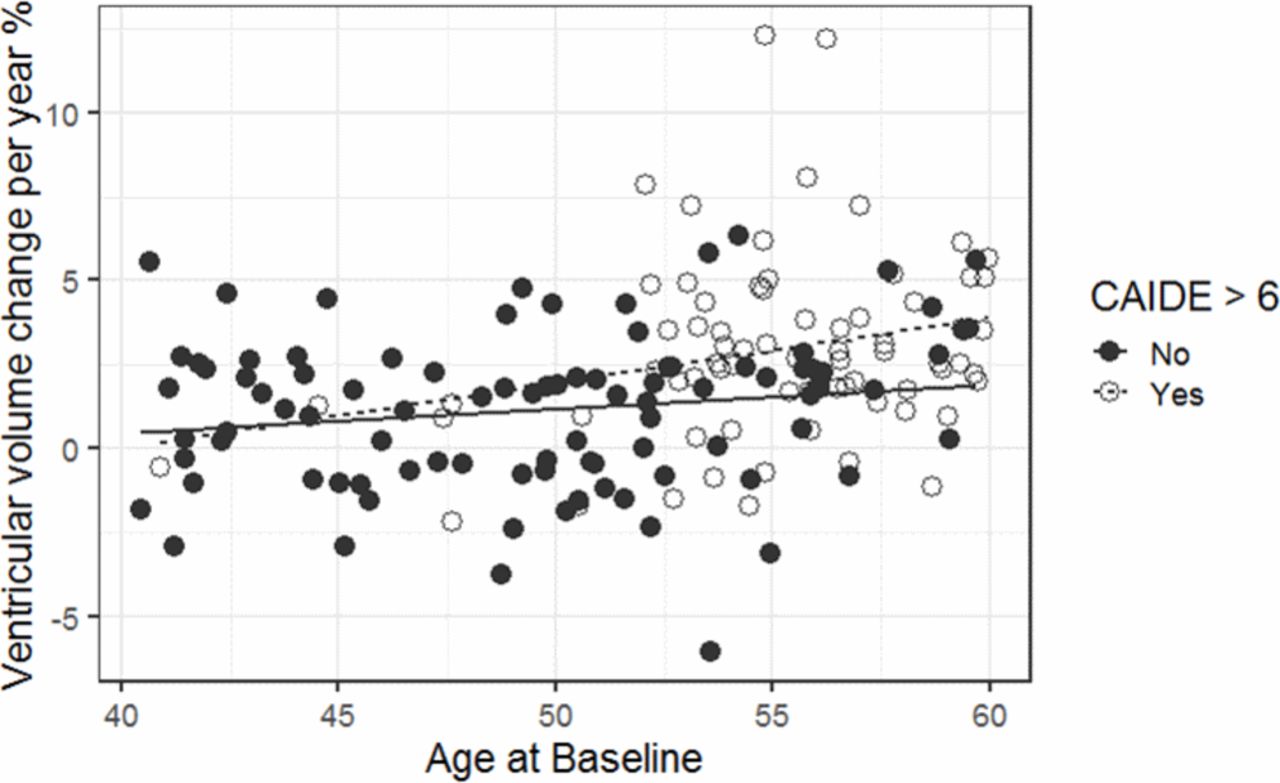
In a linear regression, including covariates of age, sex and number of years of education, ventricular enlargement was greater in those with CAIDE score >6, older age at baseline and male sex (table 4, figure 1).
{kind=link}
Ventricular expansion as a function of age. Regression lines show linear fit for CAIDE split by >6. CAIDE, Cardiovascular Risk Factors, Aging, and Dementia risk score.
Results of linear regression of annual ventricular enlargement rate and percentage brain volume change with age, years of education, sex and CAIDE score >6 as predictors
In the linear regression for brain volume change, CAIDE score >6 was the only significant predictor (table 4), although age was borderline significant.
Discussion
We found, in this group of middle-aged subjects, that having a CAIDE dementia risk score over 6 was significantly associated with brain atrophy over a 2-year period, after controlling for age, sex and years of education. The presence of the APOE ε4 allele or a parent with dementia was not related to ongoing brain atrophy.
Previous studies, using this and other cohorts, have demonstrated significant associations between CAIDE and brain volume.5 6 Data from the Framingham study11 investigated the effect of individual risk factors and found midlife diabetes associated with faster hippocampal atrophy, rated visually. A study with MRI taken up to 30 years apart found midlife CAIDE score associated with longitudinal medial temporal lobe atrophy.12 Neither of these showed strong associations with total brain volume; however, the brain boundary shift technique we used is more sensitive to longitudinal change than individual volume measurement.13
We found relatively greater ventricular expansion in male versus female participants. We could not find any previous analysis of the effect of sex on ventricular expansion using the siena technique; however, one paper using ventricular thickness found greater longitudinal expansion in male subjects14 and there have been reports of differential trajectories of brain volume changes between the sexes in a number of structures.15 Men generally have larger ventricles16 and it could be that either the ventricular enlargement is easier to detect in bigger ventricles (due to fewer partial volume effects) or that enlargement is not a linear process and is greater in bigger ventricles. Further research is suggested to verify this finding and determine the causal factors.
We did not find an association between APOE ε4 and brain atrophy. A recent large study of amyloid deposition and cortical thinning,17 found that middle-aged APOE e4 carriers had markedly increased rates of amyloid deposition, but that the effect on cortical thinning was minimal. A separate cross-sectional study also found that the effect of the APOE ε4 on brain volume was only evident in those aged over 60. Our findings are in keeping with these studies, suggesting that APOE ε4 predisposes individuals to the Alzheimer amyloid cascade, in which brain volume changes appear at a relatively late stage.2
In our analysis, there was a strong univariate association between age and brain atrophy; however, CAIDE score >6 was significantly associated with brain atrophy even after controlling for the linear effect of age. A recent paper18 compared the utility of different dementia risk scores in predicting dementia in the large community dwelling Rotterdam study. They concluded that age was the component which contributed most to the predictive ability of the scores. However, they were unable to assess the effect of age on the CAIDE score, since all of their participants were in the oldest age category of the scoring system. They comment that since the CAIDE score was developed in middle-aged subjects, it may not be appropriate for use in the over 60 age group, since some factors such as BMI may be associated with risk in middle age, but protective in later life.19
A limitation of this study is that due to the relatively young age of the participants, the actual future incidence of dementia remains unknown. However, planned longitudinal follow-up should reveal to what extent the CAIDE score and brain atrophy relate to ongoing cognitive decline.
In summary, in order to investigate preventative strategies for dementia, it is necessary to identify at risk subjects years before the onset of clinical symptoms. Our results here, showing an association between raised CAIDE score in mid-life and longitudinal brain atrophy, support the use of the CAIDE score in studies such as the FINGER trial20 for this purpose. They also indicate that serial MRI may be a putative outcome measure in future trials aimed at disease prevention, even in this relatively young and symptom-free group.
Acknowledgments
We thank all the PREVENT-Dementia participants for their enthusiastic participation in this study.
References
Footnotes
Twitter @Craig_ritchie68
Contributors JTO’B helped obtain funding, led the design of the imaging protocol and supervised this study. MJF performed the image analysis, statistical analysis and wrote the paper. KR helped obtain funding and was involved with study design. KW was involved with study design and oversaw data collection. GBW assisted with the detailed design and implementation of the imaging protocol. CWR helped obtain funding, was involved with study design and is Chief Investigator of the PREVENT-Dementia programme. LS assisted with the detailed design and implementation of the imaging protocol and supervised all aspects of the MR data design and collection.
Funding Research grants from the UK Alzheimer's Society, the US Alzheimer’s Association and philanthropic donations. This work was funded by a grant for the PREVENT-Dementia programme from the UK Alzheimer’s Society (grant numbers 178 and 264), and the PREVENT-Dementia study is also supported by the US Alzheimer’s Association (grant number TriBEKa-17–519007) and philanthropic donations. JTO'B and LS are supported by the Cambridge NIHR Biomedical Research Centre. MJF is supported by the NIHR Newcastle Biomedical Research Centre awarded to the Newcastle Hospitals NHS Foundation Trust and Newcastle University. LS is also supported by Alzheimer’s Research UK (ARUK-SRF2017B-1). Participants were recruited at West London Mental Health National Health Service (NHS) Trust (now known as West London NHS Trust) and scanning was carried out at the Clinical Imaging Facility, Imperial College London.
Competing interests JTO’B has no conflicts related to this study. Unrelated to this work, he has received honoraria for work as DSMB chair or member for TauRx, Axon, Eisai, has acted as a consultant for Lilly and has received honorarium for talks from GE Healthcare and research support from Alliance Medical.
Patient consent for publication Not required.
Ethics approval NHS Research Ethics Committee London Camberwell St-Giles (REC reference: 12/LO/1023).
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available on reasonable request.