Article Text

Abstract
Background: Excitotoxicity is one pathogenic mechanism proposed in amyotrophic lateral sclerosis (ALS), and loss of cortical inhibitory influence may be contributory. Patients with ALS who are homozygous for the D90A superoxide dismutase-1 (SOD1) gene mutation (homD90A) have a unique phenotype, associated with prolonged survival compared with patients with sporadic ALS (sALS). In this study, transcranial magnetic stimulation (TMS) was used to explore cortical excitation and inhibition. Flumazenil binds to the benzodiazepine subunit of the GABAA receptor, and 11C-flumazenil positron emission tomography (PET) was used as a marker of cortical neuronal loss and/or dysfunction, which might in turn reflect changes in cortical inhibitory GABAergic mechanisms.
Methods: Cortical responses to single and paired stimulus TMS were compared in 28 patients with sALS and 11 homD90A patients versus 24 controls. TMS measures included resting motor threshold, central motor conduction time, silent period, intracortical inhibition (ICI), and facilitation. 11C-flumazenil PET of the brain was performed on 20 patients with sALS and nine with homD90A. Statistical parametric mapping was used to directly compare PET images from the two patient groups to identify those areas of relatively reduced cortical 11C-flumazenil binding that might explain differences in cortical excitability seen using TMS.
Results: Increased cortical excitability, demonstrated by reduction in ICI, was seen in the patients with sALS but not the homD90A patients. A relative reduction in cortical 11C-flumazenil binding was found in the motor and motor association regions of the superior parietal cortices of the patients with sALS.
Conclusions: A cortical inhibitory deficit in sALS was not demonstrable in a homogeneous genetic ALS population of similar disability, suggesting a distinct cortical vulnerability. 11C-flumazenil PET demonstrated that neuronal loss/dysfunction in motor and motor association areas may underlie this difference. The corollary, that there may be relative preservation of neuronal function in these areas in the homD90A group, has implications for understanding the slower progression of disease in these patients.
- ALS, amyotrophic lateral sclerosis
- ALSFRS-R, ALS functional rating scale
- CMAP, compound muscle action potential
- CMCT, central motor conduction time
- FDI, first dorsal interosseous
- GABA, gamma aminobutyric acid
- ICF, intracortical facilitation
- ICI, intracortical inhibition
- ISI, interstimulus intervals
- MEP, motor evoked potentials
- PET, positron emission tomography
- PSTH, peristimulus time histogram
- RMT, resting motor threshold
- sALS, sporadic amyotrophic lateral sclerosis
- SOD1, superoxide dismutase-1
- SP, silent period
- S-R, stimulus response
- TMS, transcranial magnetic stimulation
- UMN, upper motor neurone
- VD, volume of distribution
- amyotrophic lateral sclerosis
- transcranial magnetic stimulation
- D90A
Statistics from Altmetric.com
- ALS, amyotrophic lateral sclerosis
- ALSFRS-R, ALS functional rating scale
- CMAP, compound muscle action potential
- CMCT, central motor conduction time
- FDI, first dorsal interosseous
- GABA, gamma aminobutyric acid
- ICF, intracortical facilitation
- ICI, intracortical inhibition
- ISI, interstimulus intervals
- MEP, motor evoked potentials
- PET, positron emission tomography
- PSTH, peristimulus time histogram
- RMT, resting motor threshold
- sALS, sporadic amyotrophic lateral sclerosis
- SOD1, superoxide dismutase-1
- SP, silent period
- S-R, stimulus response
- TMS, transcranial magnetic stimulation
- UMN, upper motor neurone
- VD, volume of distribution
Amyotrophic lateral sclerosis (ALS) is characterised by degeneration of corticospinal, brain stem, and spinal cord motor neurones1 The cause of ALS remains uncertain. It is established that the cortical lesion is widespread, and is not confined to motor regions.2–4
Transcranial magnetic stimulation (TMS) allows cortical and corticospinal pathway function and integrity to be probed non-invasively,5 and when used with the triple stimulation technique,6 has proved useful in characterising the degree of upper motor neurone (UMN) involvement in ALS, which is variable. Hyperexcitability of the motor cortex as revealed by TMS could reflect raised intrinsic excitability of cortical cells, or a diminished inhibition of these cells. Paired TMS, using a subthreshold conditioning stimulus followed 1–5 milliseconds later by a suprathreshold test stimulus, provides unique insight into the function of intracortical inhibitory circuits,7 mediated through γ-amino butyric acid (GABA)ergic transmission. At longer (7–50 ms) interstimulus intervals (ISIs), the test response is facilitated. Such studies in ALS have provided evidence of increased cortical excitability,8,9,10 and support a role for excitotoxic pathogenic mechanisms.11 Increased cortical excitability may be caused either by increased excitability, or decreased inhibition, of neuronal pathways.
Flumazenil binds to the benzodiazepine subunit of the GABAA receptor present on neurones throughout the cerebral cortex. 11C-flumazenil positron emission tomography (PET) therefore provides a marker for cortical neuronal loss and/or dysfunction that might also reflect altered GABA-ergic inhibitory function. A pilot study with this PET radioligand confirmed significant cortical binding decreases in patients with ALS compared with controls, and not confined to motor regions.12
About 5–10% of ALS cases are associated with mutations of the superoxide dismutase-1 (SOD1) gene on chromosome 21.13–15 Most of the 109 known SOD1 gene mutations are associated with variable phenotypes, a survival period typically in the order of 1–4 years, and are inherited as a dominant trait.14 The exception is the most prevalent SOD1 mutation worldwide, an aspartate→alanine substitution at codon 90 (D90A). The D90A SOD1 gene mutation is usually inherited as a recessive trait. There is an invariable phenotype (beginning with lower limb spasticity and weakness, prior to upper limb and bulbar involvement), and prolonged survival (mean 14 years).16 Worldwide, patients with D90A have been shown to share a common founder some 18 000 years ago. To explain this paradox, the existence of a linked protective factor has been postulated, but the neuroprotective mechanism of this factor is not understood.16–18 A TMS study in patients with ALS homozygous for D90A, also aimed at exploring inhibitory mechanisms, employed peristimulus time histograms (PSTHs) rather than paired pulse stimuli. The authors were able to demonstrate delayed peak responses and a “suppression phase” in the patients with D90A compared with those with sporadic ALS, which they concluded was evidence of preserved cortical inhibitory influence.19
Using TMS, the resting motor threshold (RMT), central motor conduction time (CMCT), stimulus response (S-R) curves, silent period (SP) duration, and intracortical inhibition (ICI) and facilitation (ICF) were evaluated in a group of patients with sporadic ALS (sALS), and a group of affected patients homozygous for D90A (homD90A). The results were compared with findings in a group of healthy controls. In addition, 11C-flumazenil PET was performed on subjects from both patient groups, comparing them with each other to look for relative regional reductions in cortical 11C-flumazenil binding that might reflect reduced GABAA receptor function.
METHODS
Participants
All patients were diagnosed with ALS according to revised El Escorial criteria.20 Affected patients were rated functionally using the revised ALS functional rating scale (ALSFRS-R; 0–48, lower scores correlate with increasing disability).21 Patients were also graded in terms of UMN “burden”, by totaling the number of UMN signs on examination. These were taken as pathologically brisk biceps, supinator, triceps, finger, knee, and ankle reflexes, and extensor plantar responses assessed bilaterally, and brisk facial and jaw jerks (maximum possible score 16) (see also Turner et al4). Disease duration at the time of investigation was calculated in months from date of first symptom onset to date of investigation.
All subjects were asked to omit all medication for at least 48 hours prior to testing. None was taking any regular medication known to interact with the benzodiazepine receptor. All patients gave informed written consent, and the study was approved by the ethics committees of the Institute of Psychiatry, Hammersmith Hospitals NHS Trust, Umeå University, and King’s College Hospitals.
TMS studies
Surface electromyographic activity was recorded from the right first dorsal interosseous (FDI) muscle. The compound muscle action potential (CMAP) was determined by supramaximal electrical stimulation of the ulnar nerve at the wrist. Magnetic cortical stimulation was delivered from a Magstim 200 device (Magstim Co. Ltd, Dyfed, UK) driving a circular coil centred at the vertex and held tangentially to excite preferentially the left hemisphere. F wave minimal latency was determined from 10 consecutive supramaximal stimuli of the ulnar nerve at the right wrist at 1 Hz.
The mean RMT was determined using previously described methods.22 The S-R curves were evaluated by stimulating the motor cortex at 0.9, 1.0, 1.1, 1.2, and 1.3 times threshold, initially with the muscle at rest (auditory feedback was provided) and then with a modest isometric contraction of the FDI muscle.
ICI and ICF were evaluated using paired pulse stimulation. The intensity of the conditioning stimulus was set at 0.9 times threshold and the test stimulus set at 1.3 times threshold. Paired pulse stimulation was then performed, in the resting state, using a BiStim device (Magstim Co.) capable of delivering the two stimuli at varying ISIs (1, 2, 3, 4, 5, 7, 10, 20, and 50 ms).
Ten trials were collected for each paradigm, whose order was also randomised. The area of the averaged rectified motor evoked potentials (MEPs) obtained under each experimental condition was the measure of interest. For analysis of the S-R curves, the area of the averaged MEP obtained at each stimulus intensity was expressed as a percentage of the area of the peripherally evoked CMAP.
The SP duration was measured in each trial from the stimulus artefact to the onset of the return of sustained voluntary EMG activity, by visual inspection, using a gain of 100 μV/division. The average of 10 trials was calculated for each stimulus intensity.
To analyse ICI and ICF, the mean area of the conditioned MEP obtained at each ISI was expressed as a percentage of the mean area of 30 unconditioned (test) MEPs. (inhibition <100, facilitation >100). Central motor conduction time (CMCT) was determined using the F wave method.23
Statistical analysis
All statistical analyses were performed using SPSS software (version 11.0; SPSS Inc., Chicago, IL, USA). One way analysis of variance was performed for all TMS variables with post hoc analysis comparing patient groups with controls (two sided Dunnett test to correct for multiple comparisons). Results with p<0.05 were considered significant.
In order to explore various combinations of three or more consecutive ISIs from the paired data (for example, 1–3, 1–4, 5–10 ms), a repeated measures analysis of variance was used, with identical post hoc group analysis, comparing affected patient groups with controls (and with adjustment for multiple comparisons), with significance again set at p<0.05.
Two tailed bivariate correlations, with a Pearson coefficient, were examined between clinical variables (ALSFRS-R, duration of disease, and UMN score) and TMS measures for both affected patient groups separately. One way analysis of variance was performed for both patient groups using sex and site of onset (the latter only used for the sALS group, as the homD90A group were all lower limb onset), against all TMS measures. For the control group, similar analyses were carried out for age and sx against all TMS measures.
To reduce the potential for a type I error, only those correlations with a very high correlation coefficient (greater than +/−0.7) and p<0.05 were considered potentially relevant. However any firm conclusions drawn from these correlational results must still remain cautious, as they were not subject to any correction for potential error due to multiple comparisons.
PET studies
11C-flumazenil PET images were acquired in three dimensional mode using an ECAT 953B PET scanner (CTI/Siemens, Knoxville, TN, USA), in 20 frames over 90 minutes. Scanning started 30 seconds before a bolus injection of approximately 10 mCi (370 MBq) 11C-flumazenil intravenously over 30 seconds into an antecubital fossa vein. A metabolite corrected arterial plasma input function and spectral analysis24 were used to derive parametric images of volume of distribution (VD) for the ligand.
Statistical parametric mapping (SPM’99; Wellcome Department of Cognitive Neurology) was used to make group comparisons of the normalised and smoothed VD images.25 Individual VD images were normalised into standard Montreal Neurological Institute space using a normal 11C-flumazenil template created in house and a t test applied at voxel level to mean VD images from controls and from patients with ALS. A proportional voxel threshold of 0.8 (default setting) was used. Proportional scaling of the global VD was used (calculated using the default setting). An overall image threshold of p = 0.05 was applied to the SPMs, and only those clusters identified with a corrected p<0.05 were displayed.
RESULTS
Missing data
Clinical variables were incomplete in two of the patients with sALS. Four of the sALS and two of the homD90A patients had thresholds greater than the maximum output of the stimulator. There was no obvious phenotypic difference between these and other patients in the respective groups, and their threshold was designated 100% for the subsequent analyses. The CMCT result was missing from a total of five subjects with sALS and two homD90A subjects, owing to failure to complete the protocol or recording artefacts preventing reliable measure.
Participants
The group characteristics in the TMS studies are summarised in table 1. 11C-flumazenil PET was performed on 20 of the 28 patients with sALS (mean age 57 years, ALSFRS-R 38, UMN score 8) and nine of the 11 homD90A patients (mean age 53 years, ALSFRS-R 33, UMN score 8).
Group characteristics in TMS studies
TMS studies, RMT and CMCT, S-R curves, and SP
The mean and SD for each measure in the TMS studies are shown in table 2.
TMS measures in controls and patient groups
RMT and CMCT were both significantly higher than controls in both the sALS and homD90A groups (p<0.05) (fig 1).
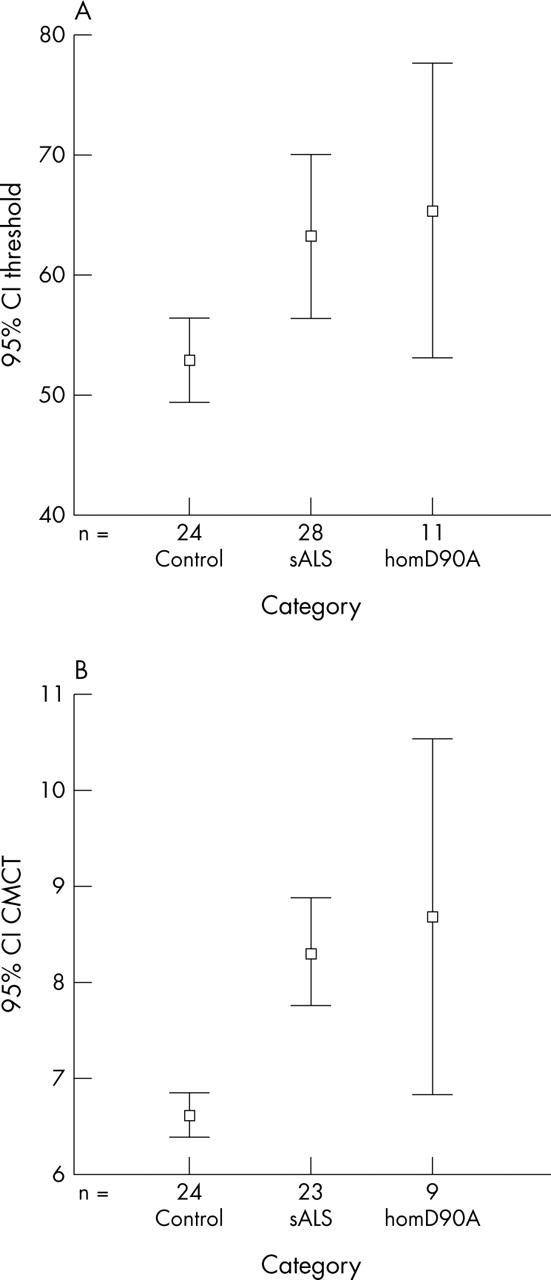
Error bar plots with 95% confidence intervals (CIs) of RMT (A) and CMCT (B) for each subject group. Both measures are significantly higher in the patient groups compared with controls (p<0.05). RMT, resting motor threshold; CMCT, central motor conduction time; sALS, sporadic ALS; homD90A, homozygous D90A SOD1 ALS.
There were no significant group differences in the S-R curves, obtained with the target muscle relaxed. When the target muscle was contracted, the homD90A patients showed significantly reduced MEP size when the stimulus intensity was 1.3 times threshold, compared with controls (p<0.05) (fig 2).
There was no significant difference in the duration of the SP for any group (fig 3).
Inhibitory measures
In the paired stimulus paradigm, the sALS patient group showed significantly reduced inhibition at ISI 1 and 2 ms and reduced facilitation at 10 and 50 ms (p<0.05). The mean inhibition ratio across the range of ISI 1–3 ms was also significantly reduced in the sALS group compared with controls (p<0.05), but not using any other combination of multiple ISIs. In contrast, the pattern of inhibitory and facilitatory responses across the full range of inidividual ISIs in the homD90A group was not significantly different from controls (fig 4).

Responses to TMS across a range of stimulus strengths with the target muscle relaxed (A) and activated (B). The homD90A group showed significantly less response at maximum stimulation in the activated state compared with controls (p<0.05) (result circled). sALS, sporadic ALS; homD90A, homozygous D90A SOD1 ALS; MEP, motor evoked potential; CMAP, compound motor action potential; t, threshold.

Silent period measured during stimulation with the target muscle in the activated state. There was a lengthening of SP with increasing stimulus strength, but no significant difference between patient groups and controls. sALS, sporadic ALS; homD90A, homozygous D90A SOD1 ALS; ms, milliseconds; t, threshold.

Inhibition of response to paired TMS stimuli over a range of interstimulus intervals, expressed as a percentage of the unconditioned response (lower percentage = more inhibition/less facilitation; 100% line drawn horizontally). The sALS group shows significantly reduced inhibition compared with controls at 1 and 3 ms, and significantly reduced facilitation compared with controls at 10 and 50 ms (p<0.05) (results circled). The homD90A group responses were not significantly different to those of the controls however, suggesting relative preservation of inhibitory cortical mechanisms. ICI, intracortical inhibition. ICF, intracortical facilitation; ISI, interstimulus interval; sALS, sporadic ALS; homD90A, homozygous D90A SOD1 ALS; ms, milliseconds.
Intragroup correlations
In the control population there was no significant correlation between age at investigation and any TMS measure, and no significant effect of sex.
Within the sALS group paired study at ISI 1 ms, men showed significantly greater inhibition than women (37% v 84% of unconditioned response, p<0.02). There was no significant effect of sex, site of onset, or clinical variables such as UMN score, for any other TMS measures.
Within the homD90A group, duration of disease correlated positively with motor stimulation threshold (r = 0.8, p<0.004) and size of the conditioned response at ISI 3 ms (r = 1, p<0.001), and negatively with duration of the silent period when the stimulus intensity was threshold and 1.1 and 1.2 times threshold (r>−0.7, p<0.02). The ALSFRS-R score correlated negatively with the size of the inhibitory response at ISI 1 ms (r = −0.9, p = 0.003) and 3 ms (r = −0.8, p<0.01). The UMN score correlated negatively with size of the MEP obtained when the stimulus intensity was 1.1 times threshold with the target muscle relaxed (r = −0.7, p<0.03). There was no significant effect of sex.
PET studies
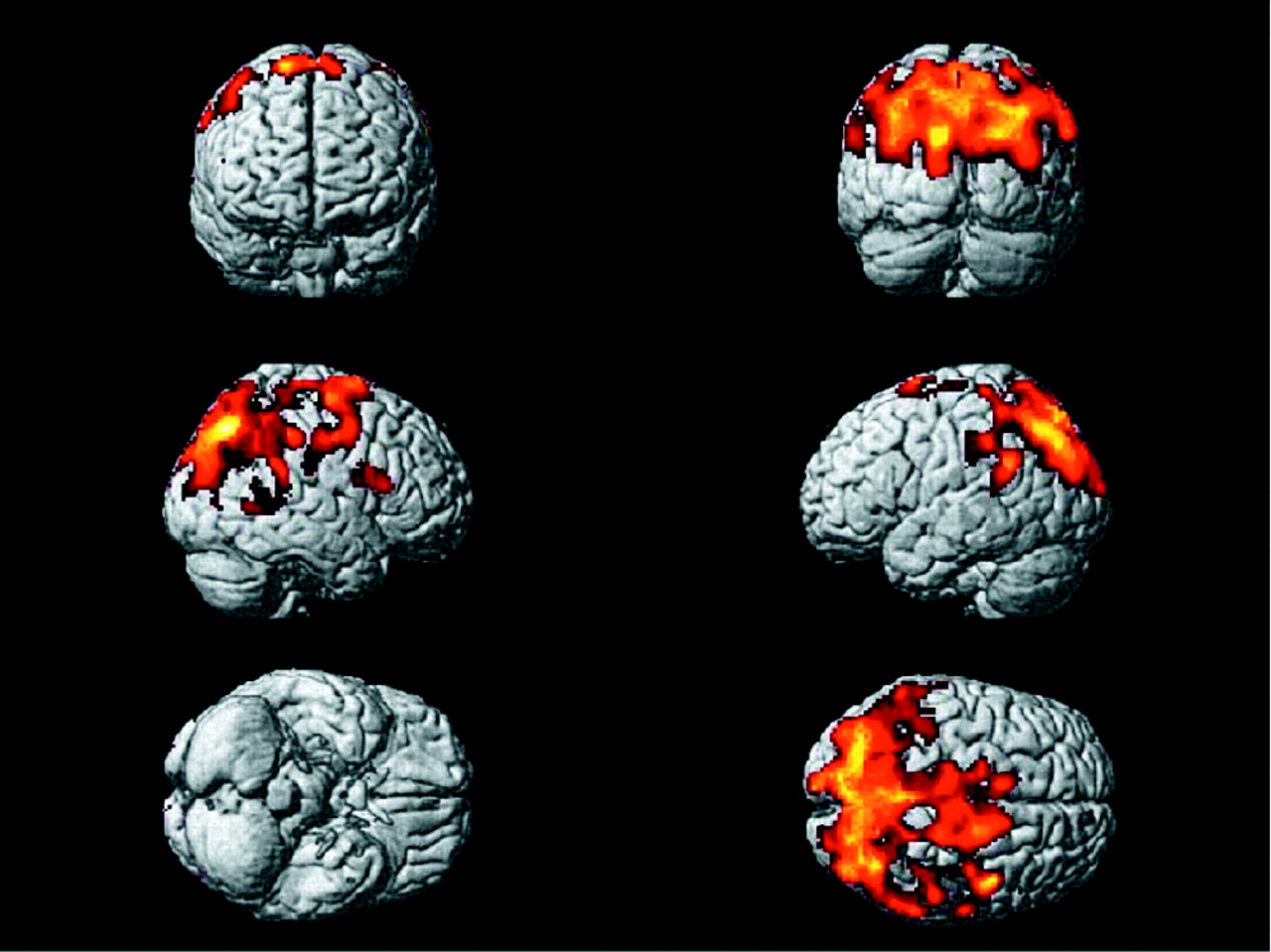
Bilateral significant areas of relatively decreased cortical binding of 11C-flumazenil to GABAA receptors were seen in the sALS patients compared with the homD90A subjects (p<0.05). These were concentrated over the motor cortex (precentral gyri) and posteriorly in the motor association areas, particularly over the superior parietal cortices (fig 5).
{kind=link}
{kind=link}
SPM rendered to generic 3D brain (shown from six angles) demonstrating areas of relative decrease of 11C-flumazenil binding in patients with sALS versus those with homD90A (cluster corrected p<0.05). The areas of relatively decreased binding in the sALS patients were concentrated in the motor (precentral gyri) and motor association areas, particularly those of the superior parietal lobes bilaterally. This relative reduction may reflect the increased cortical excitability seen during TMS, in contrast to the relatively preserved inhibition in the homD90A patients. sALS, sporadic ALS; homD90A, homozygous D90A SOD1 ALS.
DISCUSSION
This TMS study has provided evidence of differential cortical excitability in patients with sALS and those with SLS and homD90A SOD1 with similar functional disability. A unique parallel visualisation of the GABAA receptor through 11C-flumazenil PET localised the relative deficit in the sALS patients to motor and motor association areas. Although we cannot be certain whether the reductions in binding of 11C-flumazenil are due to neuronal loss or purely functional GABA-ergic decreases, the two are not mutually exclusive.
Patients with sALS showed evidence of reduced intracortical inhibition in paired pulse studies at short ISIs, but also a significant lack of facilitation at higher ISIs, compared with controls. In contrast, paired pulse studies in patients with homD90A demonstrated preserved inhibition. The pattern of relatively reduced cortical 11C-flumazenil binding in patients with sALS compared with the homD90A patients supports the concept of reduced inhibitory influence, via GABAA receptor transmission, in sALS. The relative preservation of such circuitry in homD90A patients with ALS may be one mechanism accounting for prolonged survival in this group.
Cortical excitability in ALS and previous TMS studies
The concept of excitotoxic neuronal damage in ALS (and other neurodegenerative disorders) is established.11,26 A contributory mechanism may be loss of inhibitory GABAergic function, and pathological studies support loss of cerebral inhibitory interneuronal cells in ALS3 and an alteration in the expression of GABAA receptor unit subtypes in the motor cortex.27 A previous 11C-flumazenil PET study supported loss of cortical GABAergic influence in ALS, possibly through loss of neurones bearing the receptor, and this was not confined to motor regions.12 PET activation studies support the concept of increased cortical excitability through a “boundary shift” effect during motor activity.28 In keeping with our findings, several other studies in patients with sporadic ALS have demonstrated a deficit of intracortical inhibition at short ISIs, suggestive of increased cortical excitability.8,9,10
In contrast to a previous study,9 we demonstrated significantly reduced facilitation at 10 and 50 ms ISIs in the patients with sALS compared with controls. Although facilitation was not statistically significantly reduced in the homD90A patients, this may simply reflect the greater variance in the data for this group. Riluzole has been reported to alter TMS measures both in patients with ALS and in controls. It does not appear to alter motor threshold,29 but may increase the duration of the SP30 and enhance ICI in patients.30,31 Although it was found to suppress ICF in controls,32,33 this was not demonstrated in patients.31 It was not clearly stated whether riluzole was being taken by the patients tested in previous paired stimulus TMS studies in ALS8,9,10; however, it is unlikely, as the licensing of this drug occurred near to the time that these studies were performed. Although in the present study patients did not take riluzole for at least 48 hours prior to study (at least four drug half lives34), it is possible that some effect of this drug persisted, and theoretically this could account for the relatively reduced facilitatory responses in our results. However, another pre-riluzole study also noted reduced ICF in some ALS patients.35 We are confident that the differences in ICI are not merely a drug effect; indeed, given that riluzole might be expected to have enhanced ICI, the size of the differences in this study would then be an underestimate. In a study of the effects of carbemazepine on TMS measures, no effect on ICI or ICF was found.36
The most striking finding is the lack of significant difference in response to paired stimulation in the homD90A patients with ALS compared with controls. This strongly suggests that inhibitory pathways responsible for the effect at short ISIs are intact in this patient group, in contrast to the patients with sALS. It is noteworthy that this was in spite of the fact that the homD90A patients were functionally slightly more disabled than the patients with sALS (mean ALSFRS-R score 34 v 37).
Such inhibitory pathways may conceivably also have a role in the significantly reduced response to high intensity stimulation in the activated paradigm that we noted in the homD90A group compared with controls, but this remains speculative. We noted a correlation at short ISIs between reduced inhibitory responses and both increased disease duration and decreased ALSFRS-R score, suggesting that the relative preservation of cortical inhibitory function in the homD90A patients may wane over the course of the disease in this group.
The striking relative reduction in sALS compared with the homD90A group for the binding of 11C-flumazenil to GABAA receptors in motor and motor association areas is compatible with reduced GABAergic influence, either through loss of neurones bearing the receptor or functional receptor changes, or indeed both. It is established that patients with sporadic ALS have significant cortical reduction in the binding of 11C-flumazenil compared with healthy controls.12 The involvement of parietal regions might seem surprising, but neuronal changes in this area have been previously noted in neuropathological2,37 and neuroimaging38 studies in ALS. The relative preservation of inhibitory influences in such areas in the homD90A patients may be linked to the preserved inhibition seen neurophysiologically,19 and suggests an altered cortical vulnerability in this group.
Central motor conduction time and RMT
Our study demonstrated significantly prolonged CMCT and RMT in both the sALS and homD90A patient groups compared with controls. Prolongation of the CMCT in sALS has been previously reported to occur in only about 20% of sALS patients,39–42 but was more consistently seen in a study of homD90A patients.16 In this latter group, however, it has been shown that cortex to muscle latency may only be prolonged when the muscle is activated.43 CMCT is not thought to change with disease progression,39 and there was no correlation between this measure and disease duration in this study.
Some studies have noted a reduced corticomotor threshold in ALS, frequently soon after onset of symptoms.22,44 We chose to include those patients with a threshold above maximum possible stimulation in the analysis (designated 100%), and although their exclusion rendered the differences in mean RMT non-significant, it was still not lower than controls in either group. It has been previously reported that there is no change in RMT with disease progression in sALS,39,45 although we noted a positive correlation in the homD90A group.
Silent period
The SP is, in part, a measure of cortical inhibition,7 and has been reported to be shortened in patients with ALS,41 and to decrease with disease progression.46,47 In a more detailed study it was suggested that any reduction is only seen shortly after clinical presentation, and is less obvious as the disease evolves.39 Although there was a steady increase in SP with increasing stimulus intensity in our study, this occurred in all groups. The disease duration in this study ranged from 9 to 80 months in the sALS and 9 to 162 months in the homD90A group, and so was probably beyond the “early stages” where changes in SP might have been seen. There were, however, negative correlations noted between disease duration and SP length in the homD90A group at two stimulus strengths, but not the patients with sALS.
UMN involvement
In order to qualify for one of the defined categories within the revised El Escorial criteria for ALS,20 it is necessary to have demonstrable UMN signs. This study incorporated a 16 point scale of pathological UMN signs, which lends itself easily to parametric analysis. In a study of microglial activation in vivo, the UMN score correlated closely with microglial activation in the motor cortex.4 Previous studies have noted higher motor stimulation thresholds in those with UMN signs in the hands,39,48 and lower than normal thresholds in those with no signs in the hands.22,44
The mean UMN score was similar for both patient groups in this study, and no meaningful correlations between UMN score and threshold, CMCT, or any other TMS measures were noted; neither was there a significant effect of site of onset within the sALS group. In contrast to imaging studies, where the UMN score has correlated with increased burden of cortical disease,4,49 overall the influence of UMN involvement on the cortical lesion as demonstrated by TMS remains unclear.
Sex
In keeping with another study,50 no clear effect of sex on TMS measures in controls was demonstrated.
CONCLUSION
This study supports the notion that cortical excitability is abnormally increased in sALS, and also demonstrates that patients with similar functional disability but homozygous for the D90A SOD1 gene mutation appear to have relatively preserved cortical inhibitory mechanisms. The relatively reduced binding of the PET GABAA receptor ligand 11C-flumazenil in motor and motor association cortical regions of the patients with sALS supports the concept of relatively reduced inhibitory GABAergic influence as a potential mechanism accounting for, or exacerbating, increased cortical excitability. We propose that the homozygous D90A patients have a distinct cortical vulnerability, one in which intrinsic cortical inhibitory neurones are relatively preserved,19 and which may have a bearing on the latter group’s characteristic and slowly progressive disease phenotype.
Acknowledgments
M R Turner is supported by a Wellcome Trust Clinical Research Fellowship, who also provide funding to A D Osei-Lah and K R Mills. The King’s MND Care & Research Centre (M R Turner, A Al-Chalabi, C E Shaw, P N Leigh) receives support from the Motor Neurone Disease Association (UK). A Hammers receives support from the Medical Research Council (MRC). A Al-Chalabi is an MRC Clinician Scientist. P M Andersen is supported by the Swedish Brain Research Foundation, the Hållstens Brain Research Foundation, and the Swedish Medical Society and the Björklund Foundation for ALS Research. D J Brooks receives support from the MRC.
We are indebted to the patients for their participation in this project, particularly those who travelled to the UK from Sweden. Thanks also to the radiographers A Blyth, H McDevitt and S Ahier, and PET technician L Scnorr.
REFERENCES
Footnotes
-
Competing interests: none declared