Article Text

Abstract
Objective To determine whether neuropsychological measures differ between patients with idiopathic Parkinson's disease (PD) who acquire dementia within 10 years of disease onset versus those who acquire dementia later in the disease course, using data from the longitudinal Sydney Multicentre Study of PD.
Methods The Sydney Multicentre Study of PD is a cohort of 149 community-living de novo patients with idiopathic PD studied over a 20-year period. Detailed clinical and neuropsychological tests were administered at baseline and at 3, 5, 10, 15 and 20 years, and the dementia status was assessed at each time point. For the present study, the pattern of longitudinal neuropsychological measures was compared between PD patients with the onset of dementia in the middle (5–10 years, mid-stage PD dementia, N=20) or late (>10 years, late-stage PD dementia, N=10) disease stages using analysis of variance and multiple linear regression modelling, and the relationship between age and dementia onset assessed using survival statistics.
Results Mid-stage PD dementia patients were differentiated from late-stage PD dementia patients by having greater deficits in vocabulary skills prior to and at dementia onset. The pattern of cognitive deficits following dementia onset are similar, and there is no difference in the age of dementia onset between the different PD groups.
Conclusions These data suggest that the evolution of dementia within PD occurs at around 70 years of age, regardless of the time of PD onset, and affects cognitive domains in a similar way, although patients with earlier-onset PD have a preserved linguistic ability prior to dementia onset.
- Dementia
- linguistics
- longitudinal study
- Parkinson's disease
- cognitive neuropsychology
- cognitive neuropsychology
- dementia
- parkinson's disease
Statistics from Altmetric.com
- Dementia
- linguistics
- longitudinal study
- Parkinson's disease
- cognitive neuropsychology
- cognitive neuropsychology
- dementia
- parkinson's disease
Introduction
Dementia and cognitive impairment are common problems in advanced idiopathic Parkinson's disease (PD),1 2 causing higher death rates and increased frailty,3 4 and making it more difficult for patients to attend neurological clinics or visit their community neurologist. Dementia and the neuropsychiatric problems associated with cognitive impairment are leading causes of nursing-home placement for PD patients,4 5 and recent retrospective data show a consistent relationship between dementia onset, advanced age and increasing Lewy-body scores.6 Evidence to assist with predicting when dementia may intervene in PD is likely to be of assistance in developing effective preventive treatments.
The Sydney Multicentre Study is one of a few studies that has assessed the changes in cognition occurring with disease duration by neuropsychologically examining PD patients first when they were newly diagnosed and treatment-naïve and later at 3, 5, 10, 15 and 20 years after diagnosis, when they were on treatment.4 7–9 This dataset allows for the assessment of predictive indicators differentiating PD patients who will acquire dementia earlier versus later during the disease course. In our recent report on cognitive screening performed by a neurologist,9 we showed that 83% of the survivors acquired dementia at 20 years. Here, we assess demographics and neuropsychological data performed by a neuropsychologist in order to determine cognitive differences that will assist with identifying an earlier onset of dementia during the course of PD.
Methods
Cohort
The study patients were participants in the Sydney Multicentre Study of PD, a long-term study that was initially designed to compare the efficacy and safety of low-dose bromocriptine with low-dose levodopa over a 5-year period in community-living subjects who were newly diagnosed as having PD.7 Patients with newly diagnosed PD were recruited from 1984 to 1987 from the Sydney metropolitan region. Community volunteers, spouses and friends of the PD patients were recruited as controls and screened for exclusion criteria using a general health questionnaire. Detailed clinical and neuropsychological assessments were performed at study entry before treatment initiation (baseline) and at follow-up examinations at 3, 5, 10, 15 and 20 years. Fifty individuals were selected as age- and education-matched control subjects, and followed for the first 5 years. For the first 10 years of the study, participants were examined in hospital outpatient clinics; in subsequent years, frail patients who were unable to travel to the clinic were examined in their home or nursing home. All assessments were conducted by the same neurologist (MAH) and neuropsychologist (WGJR). The initial research protocols were approved by the Sydney Metropolitan Area Health Services Human Research Ethics Committees, with approval for long-term follow-up from the Sydney West Area Health Service Human Research Ethics Committee. Informed consent was obtained from all participants. The study design and the baseline, 5-year and 10-year follow-up neuropsychology have previously been reported.10–12
Clinical and neuropsychological assessments
Examinations always took place on the same day of the week at the same time of day over a 20-year period for PD patients and over a 5-year period for control subjects. Clinical signs were recorded using a modified Columbia scale,13 while disability was assessed using a modified North Western Disability Scale.14
The neuropsychological assessment battery was designed to sample a range of cognitive domains including vocabulary store and premorbid ability (Vocabulary WAIS-R),15 memory (Rey Auditory Verbal Learning Test or RAVLT16 and Benton Visual Retention Test17), executive/adaptive frontal-lobe function (Block Design Test WAIS-R,15 Ravens Coloured Progressive Matrices Test18 and Controlled Oral Word Association Test19), visuospatial skill (Block Design Test WAIS-R) and information processing (Choice and Simple Reaction Time). Verbal Fluency (the letters FAS and Animal Category Fluency)20 differed from other Executive tests and was treated as a separate domain. Deterioration in motor function associated with disease progression made it difficult to distinguish visuospatial deficit from motor impairment; therefore, we did not include additional tests of visuospatial ability using graphomotor skill in tasks requiring copying. Details of the tests and administration procedures were reported previously.11
Assessment of cognitive status and definition of dementia
Cognitive scores were constructed for each of the six domains by summing the scores of individual tests within that domain: Memory (RAVLT Trial 5, RAVLT Recall list A and Benton Visual Retention Test correct score), Vocabulary (vocabulary raw score of WAIS-R), Verbal Fluency (FAS and animal fluency), Executive Function (Ravens Colored Progressive Matrices total score and WAIS-R Block Design age-scale score), Visuospatial Skills (Block Design) and Reaction Time (Simple Reaction Time). Although choice reaction time was tested as a measure of information processing, choice reaction time was excluded in calculating the Reaction Time cognitive score due to the extremely high variability of this measure. The Reaction Time score (in seconds) was multiplied by −1 in order to maintain consistency with the other five domain scores, in which lower values imply deficits.
Cognitive status was quantified using domain-specific z-scores. Cognitive impairment was defined as a test score that fell two standard deviations away from the mean cognitive score of the control group. Using Diagnostic and Statistical Manual of Mental Disorders-IV American Psychiatric Association and Alzheimer's Disease and Related Disorders Association criteria,21 dementia was defined as clearly and unambiguously present if the patient showed cognitive impairment in memory and in two other areas of cognitive functioning.
Subjects were classified into two groups based on time to dementia. Patients with classic idiopathic PD clinically but also with dementia on neuropsychological testing at baseline or within the first 3 years were not included in the analysis (as they may satisfy criteria for dementia with Lewy bodies, N=33).22 Patients who acquired dementia at 5–10 years after diagnosis of PD were classified as having mid-stage PD dementia (MPDD), and those with dementia appearing 10 years after PD diagnosis were classified as having late-stage PD dementia (LPDD).
Statistical analysis
The time to dementia was assessed using Kaplan–Meier survival statistics. The effect of age of dementia onset was modelled using the Cox proportional hazards model. Data are presented as HRs and their 95% CI. Analysis of variance with posthoc protected t tests was used to assess differences between groups in cognitive domain scores at the time of diagnosis of dementia. To compare differences in cognitive test scores between groups, we used multivariate linear regression modelling covarying for age, sex and education with posthoc pairwise Mann–Whitney U test comparisons. Correlations between clinical and cognitive domain scores were assessed using Spearman rank tests. Analyses were performed using SPSS software, version 15. Statistical significance was defined as a p value of <0.05.
Results
Prevalence of dementia and distinguishing demographics
The study initially enrolled 149 community-living individuals with newly diagnosed classic idiopathic PD.7 Forty-one subjects did not receive a full neuropsychological assessment at baseline for one of the following reasons: native language other than English (N=22), additional atypical disease symptom (N=13) and withdrew consent (N=6). Thus, the cohort for neuropsychological study consisted of 108 subjects.
Table 1 presents the mean age and dementia status of the study cohort at baseline and at follow-up at 3, 5, 10, 15 and 20 years. The size of the cohort decreased over time due to increasing mortality. Notably, the prevalence of dementia remained relatively stable for the first 10 years, then dramatically increased.
Demographic data of surviviors at each assessment
Clinical features for groups acquiring dementia at different stages of PD are given in table 2. In 20 patients, a diagnosis of dementia was made 5–10 years after PD onset (MPDD), and in 10 patients dementia appeared late (LPDD). There were no significant differences between groups in the age at onset of dementia (70±5.5 years) or the age at death (77±5.5 year). As illustrated in figure 1, a younger age of PD onset was associated with a significantly longer dementia-free survival by Cox proportional hazards modelling (HR=1.08, 95% CI 1.03 to 1.13, p<0.001, proportionality assumption upheld upon testing with time-dependent covariate). A subject with a PD onset age of 75 years is 4.8 times as likely as a subject with a PD onset age of 55 years to develop dementia.
Demographic features of dementia groups

Survival-to-dementia curves plotted for Parkinson's disease groups defined by onset age divided into quartiles excluding those with dementia at presentation. The earlier the onset of Parkinson's disease, the longer the survival prior to dementia onset.
Cross-sectional assessments of neuropsychological functioning in MPDD compared with LPDD
At baseline, MPDD and LPDD did not differ from control subjects in any of the cognitive domains.
At 10 years, linear regression modelling showed that the MPDD group differed from baseline in all cognitive domains covarying for age, sex and education (simple reaction time worse than memory, then executive functioning, visuospatial skills, vocabulary and least affected verbal fluency; figure 2A). LPDD only differed from MPDD in simple reaction time (p<0.03) and memory (p<0.04, figure 2A).

Z score graphs of the cognitive domains distinguishing the three dementia phenotypes in Parkinson's disease, where 0 represents the control group. Asterisk, different from all groups; Exec, executive function; Mem, memory; SRT, reaction time; star, different from controls; VF, verbal fluency; VisS, visuospatial; Voc, vocabulary. (A) Ten-year follow-up. The mid-stage Parkinson's disease dementia (MPDD) group was worse across all domains with the greatest impairment evident in reaction time and memory. The MPDD group had significantly poorer reaction times and memory than the late-stage Parkinson's disease dementia (LPDD) group, with these tests clearly distinguishing between these groups at this time. The LPDD group had a similar performance to that of the controls. (B) Twenty-year follow-up. The LPDD group was worse across all domains with the greatest impairment evident in reaction time and memory. (C) Comparison between groups at the time of dementia onset revealing that MPDD cases had greater linguistic deficits compared with LPDD cases.
At 20 years, a small group of PD patients (N=15) survived to be neuropsychologically assessed at 20 years (LPDD). Their performance at 20 years was compared with their baseline scores, and these comparisons show a marked decline from baseline across all cognitive domains (figure 2B). The greatest decline was seen in information-processing ability, with a dramatic increase in simple reaction time, followed by declines in the cognitive domains of memory, visuospatial skill and executive functions. Significant declines in vocabulary and verbal fluency also began to emerge in the LPDD patients at 20 years.
At the time of dementia onset, linear regression modelling showed a greater impairment in vocabulary (p<0.045) in the MPDD compared with the LPDD group (figure 2C).
Longitudinal analysis of neuropsychological functioning in PD
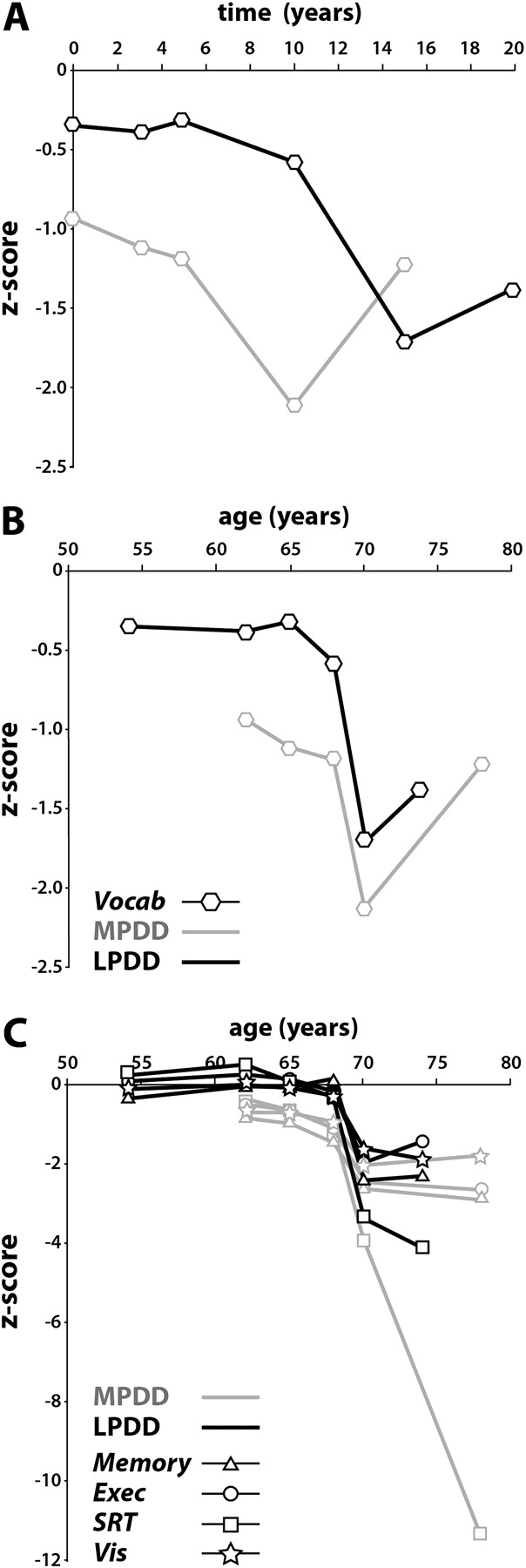
Analysis of the individual groups based on the cognitive domains that differentiated MPDD from LPDD (vocabulary score) revealed limited deficits in LPDD patients until 10 years after baseline, but a poorer performance in vocabulary in MPDD patients from PD onset (figure 3A). A significant decline in vocabulary occurred at 5 years for the MPDD group and at 10 years for the LPDD group (figure 3A). Assessment of this deficit by age of PD onset revealed this more significant decline to be related to chronological age rather than disease duration (figure 3B), with all deficits significantly increasing around the age of 70 (figure 3C).

{kind=link}
{kind=link}
{kind=link}
Graphs of the longitudinal change in z scores in vocabulary (Vocab), memory, executive function (Exec), reaction times (SRT) and visuospatial function (Vis) over the 20 years, where 0 represents the control group. LPDD, late-stage Parkinson's disease (PD) dementia; MPDD, mid-stage Parkinson's disease dementia. (A) Z scores plotted from study onset showing the greater linguistic deficits prior to dementia onset in MPDD compared with LPDD. (B) Z scores for linguistic deficits plotted from age of Parkinson's disease onset showing similar deficits once dementia occurs, but greater predementia deficits in MPDD cases. (C) Z scores plotted from age of PD onset showing general cognitive decline related to chronological age with deficits significantly increasing around the age of 70.
Discussion
The Sydney Multicentre Study is the first extended neuropsychological study to assess differences in cognitive profiles in patients with PD over a 20-year time frame. In a meta-analysis of 25 longitudinal studies assessing cognitive decline in 901 initially non-demented PD patients over 29 months, consistent decline occurred in global cognitive ability, visuoconstructive skills and memory, but cognitive changes in non-demented PD patients over the 29-month period appeared to be modest.23 The present study corroborates this finding over the short term; however, assessments using the same test battery over an extended 20-year follow-up period showed that even by 10 years, the concept of modest decline in cognition is no longer valid in a PD cohort. Our results indicate that there are different cognitive profiles and severities depending on when dementia onset occurs within the disease. As recently shown, the diagnosis of dementia occurred around a similar chronological age rather than at a similar stage of PD,6 consistent with evidence that the age of PD onset significantly affects clinical phenotype.24 25 In the present study, a later chronological age of PD onset was associated with more rapid cognitive decline and poorer prognosis, while an earlier chronological age of PD onset was associated with longer survival and very late-onset dementia that particularly affected simple reaction time and memory.
In addition to age of PD onset, the severity of vocabulary impairment differed between MPDD and LPDD patients. No previous study that we are aware of has reported a specific impairment in vocabulary in PD patients, although the vocabulary test used is not routinely included in neuropsychological batteries exploring cognitive functioning in PD. Our findings are consistent with reports of a higher level cognitive and communication deficit in non-demented patients with PD.26–29 Communication impairment in PD has been associated with dysexecutive disorder arising from reductions in processing speed, vigilance, cognitive flexibility and working memory. These deficits have generally been acknowledged to be associated with prefrontal cortical dysfunction in PD affecting verbal fluency, sentence comprehension and narrative production.27 28 30 By contrast, other authors have reported that semantic, but not phonemic, fluency is a useful predictor of cognitive decline and dementia in PD, and argue that semantic fluency and ability to copy an intersecting-pentagons figure imply a posterior cortical rather than a frontostriatal basis for dementia in PD.31
Our unique 20-year study of PD has provided us with the opportunity to prospectively define a previously undescribed group of patients with a relatively benign form of PD. LPDD patients are younger at PD onset and have minimal cognitive impairment over a decade. Clinicopathological studies of these patients32 show a slow infiltration of Lewy bodies in the limbic system that underlie their neurocognitive deficits. A more rapid disease course is indicated in MPDD with an earlier dementia onset in the course of the disease compared with LPDD patients. A lower linguistic ability in early life33 and lower educational attainment34 are risk factors for Alzheimer's disease, and in longitudinal studies a decline in vocabulary is associated with frontal Aβ deposition.35 In MPDD, we hypothesise that the predementia decline in linguistic abilities relates to frontal Aβ deposition, as demented PD patients with cortical Aβ deposition show similar characteristics to patients with Alzheimer's disease.36 Our clinicopathological studies of MPDD patients32 show that cortical Aβ deposition is additionally associated with their neurocognitive deficits.
Several methodological problems of the Sydney Multicentre Study should be noted. The disadvantage of the 20-year study duration is that relatively few subjects survived for the 15- and 20-year follow-up assessments, making interpretation of the neurocognitive data from those groups more speculative. Furthermore, the study initially was only planned for 5 years starting in 1984, and at that time the choice of cognitive tests to be included in the study was influenced by the specific questions relevant to the study of cognition in PD at that time. The decision of which cognitive domain was the best fit for a given cognitive test was difficult and still a subject of debate, as many cognitive tests are multifactorial, and a given test may fall into more than one cognitive domain. For example, the block design test, a test traditionally associated with visuo-spatial and constructional skill, is also considered to require elements of executive functioning. A further difficulty with this particular study, as with any study of cognitive functioning in PD, comes from the marked decline in motor functioning and the development of dementia over time. Both factors have a significant effect on a patient's ability to physically perform many of the standard tests of cognitive functioning, particularly drawing tasks, pointing tasks and, as in the case of block design, the manipulation of objects where time is an important factor. In our study, observation and clinical assessment of motor function indicated that this did not appear to affect the patients' performance on the block design and drawing tests such as the Benton Visual Retention test until dementia and more severe motor impairment became very apparent.
In summary, this study found that untreated PD patients who do not acquire dementia in the very early years have cognitive functioning that can be separated into two further phenotypes (MPDD and LPDD) based on age of PD onset and linguistic abilities. Unique to our prospective study was the more cognitively benign LPDD group, consisting of younger patients with a better long-term prognosis. In contrast, PD patients with lower linguistic abilities are likely to have cognitive impairment earlier in their disease. These differences have some utility for treatment planning. Across the groups, the evolution of dementia within PD occurred at around 70 years of age regardless of the time of PD onset.
Acknowledgments
We wish to thank the participants and their carers, the clinical nurse consultants, D Grayson, for statistical analysis, and H Cartwright, for the figures.
References
Footnotes
Funding Funding from the Australian Brain Foundation has allowed the long-term follow-up of this cohort. GMH is funded as a Senior Principal Research Fellow of the National Health and Medical Research Council of Australia.
Competing interests GMH received personal compensation as a speaker (Elan Pharmaceuticals San Francisco, learned societies and government agencies) and writer (Elsevier), and received financial support for research activities from Parkinson's NSW and the Australian government.
Ethics approval Ethics approval was provided by the Westmead Hospital, Sydney, Australia.
Provenance and peer review Not commissioned; externally peer reviewed.