Article Text

Abstract
Background: Cognitive impairment plays a role in Parkinson’s disease (PD) and has important consequences for patient management. However, many aspects of cognitive impairment in PD remain unclear because of the use of different and often invalid measurement instruments. In this study, a reliable and valid instrument, the SCales for Outcomes in PArkinson’s disease-COGnition (SCOPA-COG), was used.
Aim: To evaluate cognitive functioning in a large cohort of patients with Parkinson’s disease and to assess the relations with demographic, disease related and clinical variables.
Methods: A cohort of 400 patients with PD was evaluated for cognition, motor and non-motor domains, as well as for demographic and disease related characteristics. Results were compared with 150 controls matched for overall age, sex and education distribution.
Results: Patients with PD scored significantly lower on all cognitive subdomains compared with controls, with the largest differences for executive functioning and memory. After correction for age and years of education, 22% of patients had impaired cognition, as measured by the total SCOPA-COG score, compared with controls. Across all patients, more severe cognitive impairment was associated with significantly more impairment in motor, autonomic, depressive and psychotic domains. Patients with the postural instability gait difficulty (PIGD) dominant phenotype showed more cognitive impairment compared with patients with the tremor dominant phenotype. Contrary to tremor scores, PIGD scores significantly worsened with increasing disease severity.
Conclusions: Cognition is an important domain of the clinical spectrum of PD and poorer cognitive performance is associated with greater impairment in motor and non-motor domains in PD. The difference in cognitive scores between PIGD dominant patients and tremor dominant patients likely reflects more advanced disease.
Statistics from Altmetric.com
Parkinson’s disease (PD) is predominantly characterised as a movement disorder, but over the past years there has been an increasing awareness that the clinical spectrum of PD is much broader, also encompassing many non-motor domains, including cognition.1 Cognitive decline is a predictor of dementia in PD (PDD),2 3 which has important consequences for patient management.2 4 5 The reported prevalence of dementia in PD varies greatly (2–81%) between studies.3 Consistency in the relation between cognitive impairment/PDD and demographic or clinical characteristics has only been found for age and motor impairment. Factors that have contributed to the variability between studies are sample characteristics (selection procedure, source population, sample size), applied criteria of dementia and cognitive impairment and the use of different methods for the evaluation of cognition in PD. Most studies to date have been performed on small populations and samples selected from tertiary care clinics. Additionally, several studies in PD have relied on the use of measurement instruments that have been developed for screening of dementia (Mini-Mental State Examination (MMSE)) or Alzheimer’s disease. These instruments generally lack discriminative ability to capture the specific aspects of cognitive impairment in PD. Moreover, many of these instruments include items that are sensitive to motor symptoms and may thus affect the results of cognitive assessment in PD.
Based on compelling evidence that memory, attention and executive and visuospatial functioning are important aspects of cognitive impairment in PD, a reliable and valid quantitative PD specific instrument (SCales for Outcomes in PArkinson’s disease-COGnition (SCOPA-COG)) was developed in 2003.6 In the current study, we used this instrument to evaluate the characteristics of cognitive impairment in patients with PD and its associations with demographic and clinical characteristics.
METHODS
Study design
The study is part of the PROfiling PARKinson’s disease (PROPARK) study, a longitudinal cohort study of patients with PD, who are extensively profiled on phenotype, disability and global outcomes of health, with assessment instruments that have been found to be valid and reliable in PD. Findings obtained from the first annual evaluation of 408 patients who were assessed between May 2003 and September 2005 were used in this analysis.
Study participants
Patients with idiopathic PD were recruited from neurology clinics from both university and regional hospitals in the western region of the Netherlands. All patients were diagnosed by neurologists with a special interest in PD according to the clinical diagnostic criteria of the United Kingdom Parkinson’s Disease Society Brain Bank for idiopathic PD.7 Patients were stratified according to age at onset (based on age at onset of the first symptoms as perceived by the patient ⩽/>50 years) and disease duration (⩽/>10 years), because these characteristics are important determinants of disease course in PD.8 9 Inclusion of patients stopped when approximately 100 patients were included in each stratum. No other selection criteria were applied. No attempt was made to separate demented from non-demented patients according to the DSM-IV-criteria.10 The majority of the patients were assessed at the Leiden University Medical Centre. To avoid a bias towards recruiting less severely affected patients, those who were unable to come to the hospital for the assessment were assessed at home.
Controls were selected to match the overall age, sex and education distribution of the patients and were included if they had no documented diseases of the central nervous system and were able to read and understand Dutch. Half of the controls (n = 75) were acquaintances from participating patients and the other controls were recruited from volunteers working in our hospital. The study was approved by the local medical ethics committee of the Leiden University Medical Centre and all participants gave informed consent.
Assessments
In the PROPARK study, all patients had a standardised assessment, including evaluation of demographic and clinical characteristics, family history of PD and medication. Measurement instruments for the different clinical domains of PD were derived from a prior project (SCales for Outcomes in PArkinson’s disease (SCOPA)).11 For the current study, data obtained for cognition (SCOPA-COG,6 MMSE12), depressive symptoms (Beck Depression Inventory13), autonomic function (SCOPA-AUT14), motor function (SPES-SCOPA-motor15), disease severity (Hoehn and Yahr (H&Y)16) and psychotic symptoms (modified Parkinson Psychosis Rating Scale17) were used. All patients who used levodopa or dopamine agonists and experienced motor fluctuations were assessed during the “on” state. Data collected from controls included demographic characteristics and cognition scores.
All instruments were either self-administered or administered by one of three trained research associates. The SCOPA-COG has 10 items, including memory (four items: replicating the order in which cubes were pointed out, digit span backward, immediate and delayed word recall), attention (two items: counting down by threes and months backward), executive functioning (three items: successive repetitions of fist-edge-palm movements, set shifting with dices and fluency animals) and visuospatial functioning (one item: mental reconstruction of figures). The maximum score is 43. Values of all rating scales are expressed as percentages of the maximum obtainable score (100%) for reasons of comparability. Except for the SCOPA-COG and the MMSE, higher scores indicate more severe impairment.
The association between motor phenotype (tremor or postural instability gait difficulty (PIGD)) and cognition was also evaluated. A mean score for tremor was calculated as the mean of the following items from the SPES-SCOPA-motor: rest tremor (right and left) and postural tremor (right and left) and a mean score for PIGD was calculated as the mean of postural instability, freezing during “on”, gait and walking. Patients with a ratio of mean tremor score/mean PIGD score ⩾1.5 were classified as tremor dominant whereas patients with a ratio of ⩽1.0 were classified as PIGD dominant. Patients with ratios between >1.0 and <1.5 were classified as indeterminate.
Statistical analysis
If 25% or more of the data from a particular scale were missing, this scale was excluded from statistical analyses for that patient. Linear regression and correlation coefficients were used to assess relations between SCOPA-COG scores and demographic, disease related and clinical characteristics. In the linear regression analysis, the forward method was used. For patients, three separate blocks were used in the model: block 1 (age, sex and years of education), block 2 (age at onset, levodopa dose and motor function) and block 3 (depressive symptoms and psychotic symptoms). Linear regression for blocks 1 and 2 was used to determine the separate contribution of demographic and disease related variables. In block 3, the additional contribution of depressive and psychotic symptoms to the variance of the SCOPA-COG total score was explored.
A Student’s t test for independent samples was used to assess differences in age and years of education between patients and controls, and a χ2 test was used to assess differences in sex distribution between patients and controls. Subsequently, SCOPA-COG scores of patients and controls were compared with the Student’s t test for independent samples, whereas differences between groups based on disease severity were compared by analysis of covariance.
To compare differences in subdomain scores between patients and controls, standardised z score values were calculated to account for differences in variance between the subdomains. Z scores were also used to account for differences in difficulty levels between subdomains.
Subgroups of patients with normal or impaired cognition were constructed with the following approach:
Because age and education are known to have an influence on cognition,18 the regression equation of the SCOPA-COG score of controls with the variables age and years of education was used to calculate an estimated value for every subject (controls and patients).
The difference (Δ) between the actual value and the estimated value was calculated for every subject (controls and patients).
Patient subgroups were formed on the basis of the distribution of the Δ value of the controls. This resulted in two subgroups:
normal cognition; Δ value of −/+2 SD of the data of controls;
impaired cognition; Δ value ⩽−2 SD of the data of the controls.
To analyse differences between patients with normal and impaired cognition, the Student’s t test for independent samples and the χ2 tests were used without adjusting for other variables.
To evaluate how different impairment domains relate to each other, patients were classified into subgroups, based on the quartiles of the SCOPA-COG scores, with the first quartile representing the highest and the fourth quartile the lowest scores. Ordinal regression19 was subsequently used to analyse the relation between SCOPA-COG scores and scores of the other PD domains. A p value <0.05 was considered significant. All analyses were performed using the Statistical Package for the Social Sciences 12.0.1 Software (SPSS 12.0.1).
RESULTS
Characteristics of the participants
Eight patients with PD were excluded because of too many missing values on the SCOPA-COG. Consequently, 400 patients (63% men) and 150 controls (55% men) were included in the study. No significant demographic differences existed between patients and controls (table 1).
Influence of demographic, disease related and clinical characteristics
The following regression equation best fitted the SCOPA-COG scores of controls:
SCOPA-COG score = 74.6–0.3× [age] +0.9× [years of education]
where 74.6 is a constant and age and years of education of each control are entered in the equation, thus resulting in a predicted score for each subject.
Age and years of education accounted for 22% of the variance in controls (p<0.001).
In patients, the total variance of the SCOPA-COG accounted for by the regression model was 41%. Age and years of education explained 29% of the variance whereas levodopa dose and motor function explained an additional 6%. Psychotic symptoms accounted for another 6% of the total SCOPA-COG score (p<0.001). Sex, age at onset and depressive symptoms did not contribute significantly to the explained variance of the SCOPA-COG. Correlations between the total SCOPA-COG score and other impairment domain scores were all moderate (motor function −0.35, psychotic symptoms −0.33, autonomic function −0.28, depressive symptoms −0.24).
Characteristics of the cognitive profile
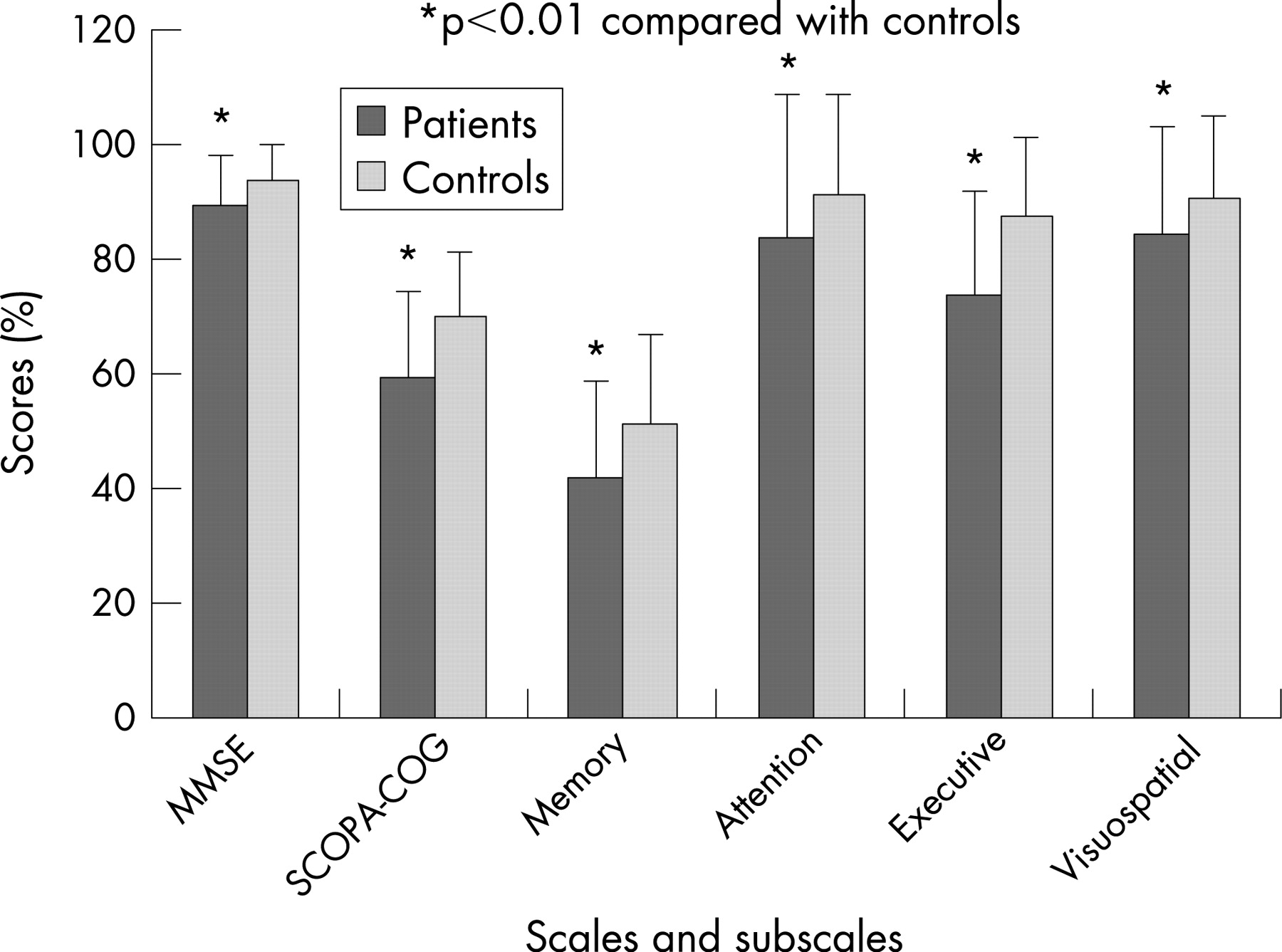
Both patients and controls had their lowest scores on the executive functioning and memory subdomains of the SCOPA-COG, with the poorest performance in the latter subdomain (fig 1). Controls performed significantly better than patients on the SCOPA-COG, each of its subdomains and the MMSE. The differences between patients and controls were largest for executive functioning (mean score patients 74% vs mean score controls 87% (mean z score difference 0.8, 95% CI 0.6 to 0.9)) and memory (mean score patients 42% vs mean score controls 52% (mean z score difference 0.6, 95% CI 0.4 to 0.7)). The differences for attention (mean score patients 84% vs mean score controls 92% (mean z score difference 0.3, 95% CI 0.2 to 0.5)) and for visuospatial functioning (mean score patients 85% vs mean score controls 91% (mean z score difference 0.3, 95% CI 0.2 to 0.5)) were smaller (all p values <0.001).
Influence of disease severity
To explore the influence of disease severity, four groups based on the H&Y stages were compared with respect to cognition scores corrected for age and sex (controls were classified as “none” (H&Y-stage 0) (n = 150), patients in H&Y-stages 1 and 2 were classified as “mild” (n = 208), patients in stage 3 as “moderate” (n = 114) and patients in stages 4 and 5 as “severe” (n = 74)). Controls performed significantly better compared with all three patient groups on the SCOPA-COG. Severely affected patients performed significantly worse compared with mildly and moderately affected patients (fig 2).

Subgroup analysis of patients grouped by cognitive performance
Using the distribution of the Δ value (difference between SCOPA-COG actual and estimated value) of the controls, 88 (22%) of the patients had impaired cognition. These patients were significantly older, had an older age at onset, longer disease duration and used a higher dose of levodopa per day. Additionally, these patients were more severely affected, as measured by H&Y, motor, autonomic, depressive and psychotic scores (fig 2, table 2).
A total of 50 patients (58%) with impaired cognition, as measured by the SCOPA-COG, had normal MMSE scores based on age and education corrected normative data. These MMSE cutoff points were the lower quartile scores of different age and education groups (total 18 056 subjects).20 Fourteen per cent of the patients with impaired cognition had a disease duration of less than 5 years.
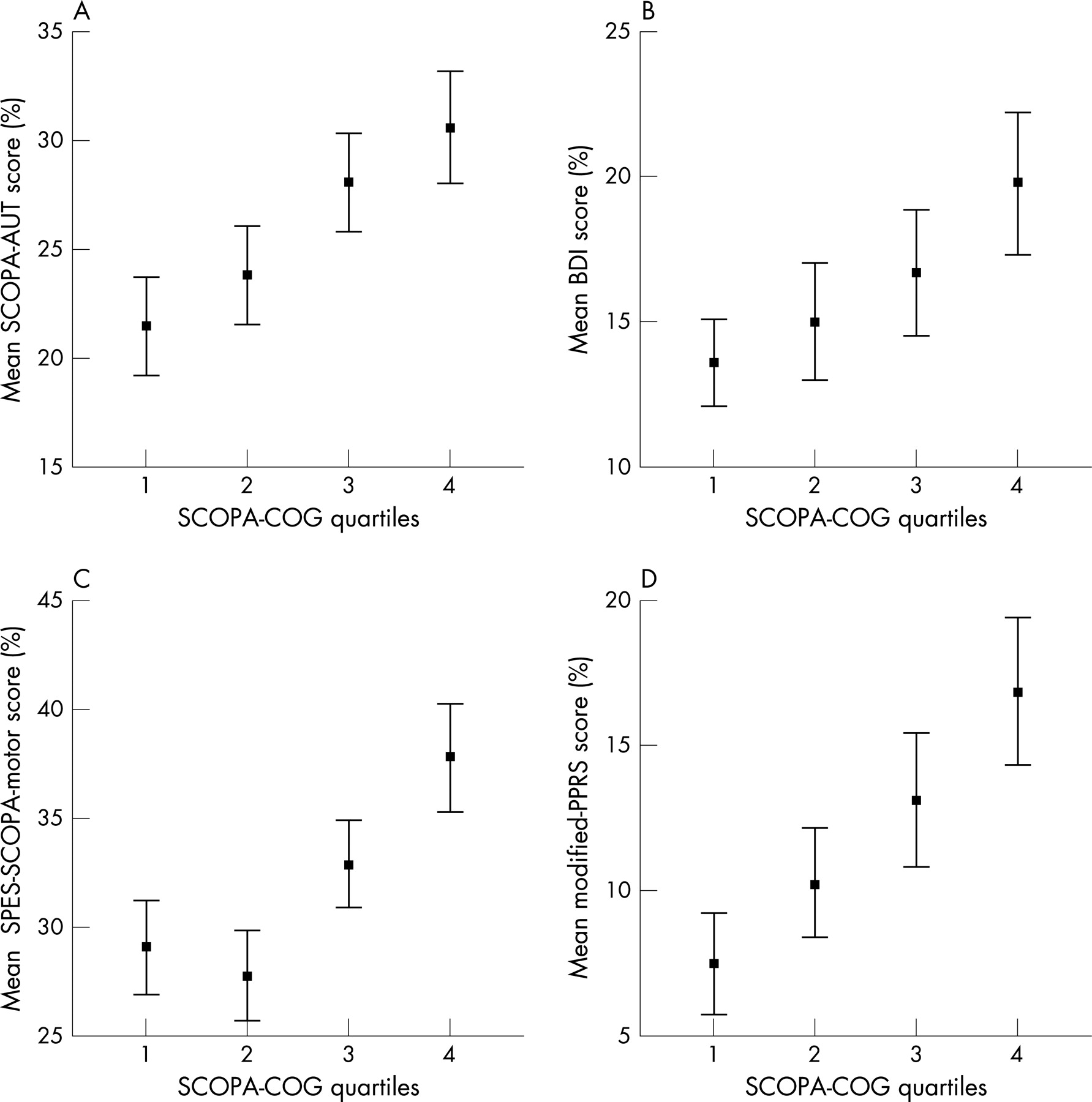
Across the four quartiles of the SCOPA-COG, increasing cognitive impairment was associated with significantly higher impairment scores of motor and non-motor domains (motor, autonomic and psychotic scores (all p values <0.001); depressive scores (p = 0.006)) (fig 3). Across groups with increasing cognitive impairment, the number of PIGD dominant patients significantly increased whereas the number of tremor dominant patients significantly decreased (p<0.001). As the assignment of the phenotype was based on the ratio, we also considered the nominator and denominator individually. We found that the mean tremor scores did not differ between the quartiles whereas the mean PIGD scores significantly increased across the quartiles (from 6% in the first quartile to 11% in the fourth quartile) (trend p<0.001). Contrary to tremor scores (r = 0.1, p = 0.070), PIGD scores (r = 0.7, p<0.001) correlated with disease severity, as measured by H&Y.
{kind=link}
{kind=link}
{kind=link}
DISCUSSION
In this study, a large sample of patients with PD was assessed with an instrument that evaluates relevant aspects of cognitive impairment in PD without being sensitive to motor symptoms.6 The findings of this study, however, should be viewed against the following background. Firstly, this is a clinic based study with a selection procedure based on age at onset and disease duration. Therefore, the results in this study cannot be generalised to the PD population in general. The percentage of patients with impaired cognition in this study cannot be interpreted as a prevalence estimate, which limits the possibility to compare our findings with prevalence rates of other studies. Secondly, the cross sectional design makes it impossible to draw conclusions about the direction of the reported relations.
In many studies on cognitive functioning in PD, the MMSE is applied as a gross measure of cognitive impairment.21 The MMSE includes items from domains which generally are less severely affected in PD (temporal orientation and language),3 22 whereas the SCOPA-COG focuses on domains which are frequently affected in PD (memory, attention and executive and visuospatial functioning).6 Therefore, the SCOPA-COG is expected to be more sensitive to the cognitive deficits of PD. This is demonstrated by the fact that in our study 58% of the patients with abnormal SCOPA-COG scores had normal MMSE scores. In this comparison, both scores were corrected for age and years of education, indicating that the MMSE may substantially underestimate the degree of cognitive impairment in PD.
In comparison with controls, all four cognitive subdomains were impaired in patients. In accordance with other studies, executive functioning was most prominently affected, followed by memory.3 23 Both controls and patients had relatively low scores on the memory subdomain, indicating that items of this subdomain are more difficult compared with items of the other subdomains. As with other measures of cognition, we found that age3 5 23–27 and (years of) education25 28 were related to the SCOPA-COG scores in both controls and patients. In line with other studies, more advanced disease (higher H&Y stage, higher SPES-SCOPA motor score) was associated with poorer cognitive performance,2 3 5 6 24 28–30 indicating an additional influence of the disease process on cognitive performance. Additionally, in agreement with others,3 24 26 we found that the psychotic domain score was weakly associated with the total SCOPA-COG score.
In daily practice, differences in levels of cognitive impairment suggest that there are subgroups of particular PD phenotypes.31 Therefore, an attempt was made to identify patients with impaired cognition by taking into account the influence of age and education. Using this approach, 22% of the patients had impaired cognition. Because of the cross sectional design of this study, we cannot exclude the fact that some patients had a decline over time in cognitive performance but still remained within the 95% confidence interval. Longitudinal research is needed to elucidate whether subgroups of PD patients exist where cognition is spared, or whether inter-patient variability is mainly explained through differences in the rate of progression of the disease.
In this study, 14% of patients with impaired cognition had a disease duration less than 5 years. Generally it is assumed that cognitive impairment may develop early in the disease process,32 33 but clinical symptoms of dementia, as detailed in the DSM-IV criteria, appear only late in the disease course.4 28 30 However, in PD, the term “dementia” is problematic because there is no disease specific definition3 21 and the DSM-IV-criteria10 require experienced disability in daily life, which poses a problem for any disease where motor impairment per se may cause such disability.3 To determine if patients with impaired cognition truly suffer dementia, a PD specific definition of dementia is required. In view of the fact that no adequate definition of dementia in PD was available, we made no attempt to distinguish demented from non-demented patients.
Our results show that poorer cognitive performance is associated with more severe impairments in other domains of PD. In line with the findings of others, we found that patients with a tremor dominant phenotype showed higher cognition scores compared with patients with the PIGD dominant phenotype.34 35 However, since the assignment of this particular phenotype is based on a ratio, we evaluated the differential influences of the nominator and denominator. We found that this ratio is only driven by the denominator (PIGD score), and hence reflects increasing disease progression. According to Braak and colleagues,36 the symptoms of PD parallel the formation of Lewy bodies and Lewy neurites, and advance in a topographically predictable sequence beginning in the medulla oblongata/pontine tegmentum and olfactory bulb/anterior olfactory nucleus with a subsequent spread to the substantia nigra and other midbrain nuclei, forebrain and neocortex. However, the clinical findings may also be explained by a differential individual vulnerability of neuronal circuits for the underlying disease process.37 As such, neuronal circuits underlying all impairment domains in PD may be affected simultaneously, but because of different cell type vulnerability, become clinically manifest at different stages.
REFERENCES
Footnotes
Funding/support: This work was supported by grants from the Prinses Beatrix Fonds (PBF, project No WAR05-0120), the Netherlands Organisation of Scientific Research (NWO, project No 0940-33-021), the van Alkemade-Keuls Foundation and the Dutch Parkinson’s Disease Society.
Competing interests: None.
- Abbreviations:
- H&Y
- Hoehn and Yahr
- MMSE
- Mini-Mental State Examination
- PD
- Parkinson’s disease
- PDD
- dementia in PD
- PIGD
- postural instability gait difficulty
- PROPARK study
- PROfiling PARKinson’s disease study
- SCOPA-COG
- SCales for Outcomes in PArkinson’s disease-COGnition