Article Text

Abstract
Background Variation in the incidence rate in epidemiological studies on amyotrophic lateral sclerosis (ALS) may be due to a small population size and under ascertainment of patients. The previously reported incidence decline in the elderly and a decrease in the male:female ratio in postmenopausal age groups have yet to be confirmed.
Methods ALS epidemiology in a large population based register in The Netherlands was studied between 1 January 2006 and 31 December 2009, and applied capture–recapture methodology in separate age and gender groups to adjust for the number of unobserved patients.
Results 1217 incident patients were observed, and a capture–recapture incidence of 2.77 per 100 000 person-years (95% CI 2.63 to 2.91). Prevalence on 31 December 2008 was 10.32 per 100 000 individuals (95% CI 9.78 to 10.86). The incident cohort had a higher median age at onset (63.0 vs 58.1 years) and more bulbar onset patients (30.0% vs 19.1%) compared with the prevalent cohort. Incidence and prevalence peaked in the 70–74 year age group followed by a rapid decline in older age. The male:female ratio in the premenopausal age group (1.91, 95% CI 1.32 to 2.79) was not significantly higher than that in the postmenopausal age group (1.50, 95% CI 1.34 to 1.67).
Conclusion The marked difference in patient characteristics between incident and prevalent cohorts underscores the importance of including incident patients when studying susceptibility or disease modifying factors in ALS. The incidence decline in the elderly may suggest that ALS is not merely the result of ageing. Absence of a significant postmenopausal drop in the male:female ratio suggests that the protective role of female sex hormones in ALS is limited.
Statistics from Altmetric.com
Introduction
Before the 1990s, incidence rates of amyotrophic lateral sclerosis (ALS) were derived from studies lacking consensus diagnostic criteria and with a retrospective design,1–6 which has important limitations in case ascertainment.7–9 Since the 1990s, several prospective population based registers have been initiated to overcome these limitations by prospective case ascertainment, using multiple sources and diagnosis based on the El Escorial criteria.10 11 Incidence rates in these registers still show large variation, ranging from 2.3 to 6.3 per 100 000 person-years in the 45–74 year age group (table 1).12–22
Comparison of prospective population based studies on amyotrophic lateral sclerosis epidemiology
Although the methodology of epidemiological studies in ALS has improved, reported variation in incidence rates may be due to two important limitations. Firstly, catchment populations were relatively small which restricts the number of newly diagnosed patients ascertained each year and increases the uncertainty of incidence estimates. The two registers that identified more than 1000 patients needed a 10 year study period to reach this number (table 1).14 18 Secondly, only three prospective studies presented incidence rates adjusted for the number of unobserved patients.14 17 18 These studies, however, determined completeness of case ascertainment only in the total population, not in each separate age by gender group. While these limitations may partly explain the variation in incidence rates, they also cause uncertainty about whether the previously reported incidence decline in the very elderly and the decreased male to female ratio in postmenopausal age groups23 is real or a result of differential coverage of patients in different age and gender groups. By using capture–recapture methodology, the number of unobserved patients can be estimated.24 Application of this methodology in separate age and gender groups in a large population based register enables these limitations to be overcome.
In the present large prospective study, we describe the epidemiology of ALS in The Netherlands for the 4 year period 2006–2009, and explore differences between the incident and prevalent cohorts.
Methods
Study area
This population based study was performed in The Netherlands (41 528 km2). According to national census data, the mean population during the study period was 16 455 911.25
Subjects
Patients diagnosed with suspected, possible, probable or definite ALS according to the El Escorial criteria were included.10 Because previous population based studies included patients with progressive muscular atrophy, primary lateral sclerosis and progressive bulbar palsy, we also included these patients to allow comparison. Individuals <15 years of age were excluded to avoid misclassification with juvenile onset motor neuron diseases. In order to determine whether a patient fulfilled the El Escorial criteria, the correspondence of the neurologist, including results of neurophysiological examination, was scrutinised. For each of the four regions (bulbar, cervical, thoracic and lumbosacral), it was determined whether a patient had signs and symptoms of lower or upper motor neuron degeneration. Other possible causes should have been sufficiently excluded, especially in the case of clinical findings inconsistent with ALS.
Sources of case ascertainment and data collection
Incident cases were identified from 1 January 2006 to 31 December 2009. Prevalent cases were all cases diagnosed before 31 December 2008 and still alive at that date. To ensure complete case ascertainment, multiple sources were used. Firstly, all patients diagnosed with ALS at one of the university medical centres collaborating in The Netherlands ALS Centre were registered. Most patients are referred at least once during the course of the disease for diagnosis or treatment to one of these tertiary referral centres. All university medical centres not participating in The Netherlands ALS Centre and the 30 largest of the 83 general hospitals were visited each year to screen their registers for ALS patients. In addition, all neurologists in The Netherlands were contacted at least once per year by mail.
Once a diagnosis has been reached, patients in The Netherlands are referred to one of the 46 rehabilitation centres specialised in the care of ALS. All centres were visited every year during the study period to scrutinise their registers for ALS patients. Furthermore, all consultants in rehabilitation medicine were informed about the study by mail once per year. Patients were also recruited by the Dutch Association for Neuromuscular Diseases (VSN). Every year their members were invited to participate in the study, and more regularly they were informed about the study in a newsletter. Finally, patients were able to register themselves via our website.
Demographic and clinical data were collected, including gender, date of birth, date of onset, site of onset, date of diagnosis and classification according to the 1994 El Escorial criteria.
Statistical analysis
Differences in baseline characteristics between incident and prevalent patients were determined using the Mann–Whitney U and χ2 tests.
Age and gender specific crude incidence rates were calculated by dividing the number of observed cases by the person-years of observation. Crude prevalence rates were calculated from the number of patients alive on 31 December 2008, divided by the total population. Poisson approximation was used to calculate 95% CIs (95% CI). Population data for the analysis of incidence and prevalence rates came from national census data.25 The population at risk was defined as the entire population older than 15 years.
To estimate the number of unobserved cases, we applied the two source capture–recapture method in each separate age by gender group. This is a method to correct for under ascertainment of cases in epidemiological surveillance when two sources are used. Patients ascertained by neurologists, consultants in rehabilitation medicine and by our website were considered as one source because there is a high positive dependence between these sources. Neurologists are used to refer ALS patients to a consultant in rehabilitation medicine and patients who had registered themselves via our website were often encouraged by their neurologist to do so. The second source we used was the membership register of the patient organisation, the Dutch Association for Neuromuscular Diseases. A formula developed by Chapman26 was applied to calculate the estimated number of patients N in the population:
The coverage rate is defined as the percentage of the estimated total number of patients N in the population identified by the two sources.
To allow comparison with other studies, incidence and prevalence rates were adjusted to the 1990 US population using the direct method.27 The Kaplan–Meier method was used to estimate survival rate. Differences in survival rate for each prognostic factor were compared using the log rank test. Prognostic factors were gender, site of onset and age of onset. In addition, multivariate survival analysis was performed using Cox's regression model.
Results
During the 4 year study period, 1217 incident patients were observed by the two sources (source 1: neurologists, consultants in rehabilitation medicine, website registrations; source 2: Dutch Association for Neuromuscular Diseases). A total of 847 patients were unique to source 1, 89 were unique to source 2 and 281 patients were identified by both sources, resulting in a total of 1217 patients. Clinical data were available for the 1128 incident patients identified by the first source (table 2). Due to privacy regulations, clinical data were not available for the 89 patients unique to source 2.
Patient characteristics
The number of unobserved incident patients was estimated to be 278 by the capture–recapture method, which results in an estimated total of 1495 incident patients in the 4 year period and an average annual incidence rate of 2.77 per 100 000 person-years (95% CI 2.63 to 2.91). There was a preponderance of men among the incident cases. Male and female incidence rates were 3.26 (95% CI 3.04 to 3.47) and 2.22 (2.05 to 2.40), respectively. Age specific incidence rates according to gender are reported in figure 1A and in supplementary table 1 (available online only). An increase in incidence with increasing age was evident in males and females until the 70–74 year age group in men and the 65–74 year age group in women. After peak incidence has been reached, there was a rapid decline in incidence in the elderly.
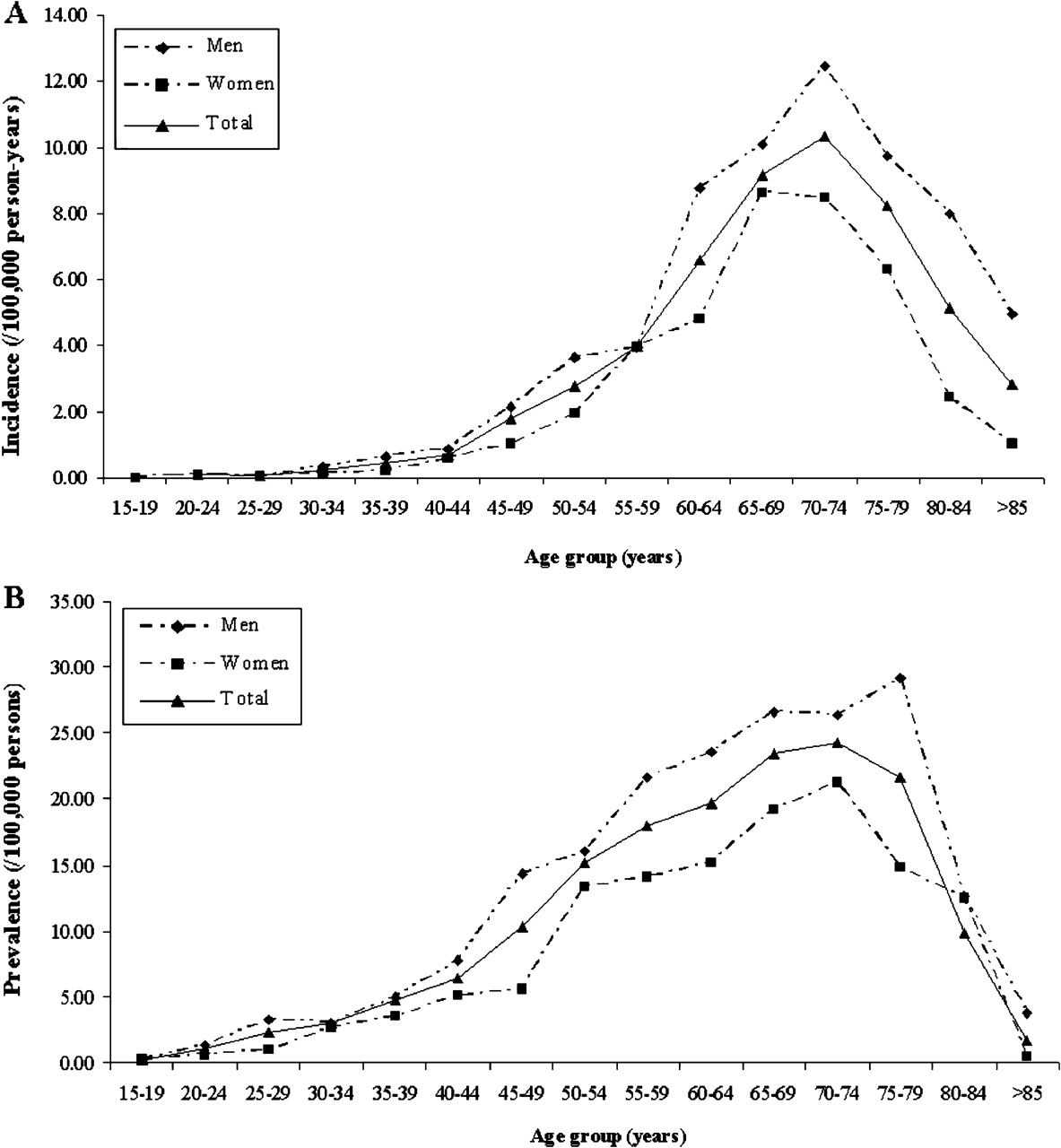
Age and gender specific incidence (A) and prevalence (B) rates.
On prevalence day, 31 December 2008, 1080 patients had been observed. A total of 490 patients were unique to source 1, 247 were unique to source 2 and 343 patients were identified by both sources. In table 2, clinical data are presented for the 833 prevalent patients identified by a neurologist, a consultant in rehabilitation medicine or by registration at our website. The total number of prevalent cases was estimated at 1400 by the capture–recapture method, which results in a prevalence rate of 10.32 per 100 000 persons (95% CI 9.78 to 10.86). The male and female prevalence rates were 12.05 (95% CI 11.22 to 12.89) and 8.20 (7.52 to 8.87), respectively. Prevalence rate peaked in the 75–79 year age group in men and in the 70–74 year age group in women (figure 1B and supplementary online table 2).
The incidence rate, age and gender adjusted to the 1990 US population,27 for the 45–74 year age group was 5.27 (95% CI 4.98 to 5.56) per 100 000 person-years for the overall population, 6.13 (95% CI 5.67 to 6.60) for men and 4.51 (95% CI 4.10 to 4.91) for women. Previous prospective population based studies on ALS have reported comparable 1990 US population standardised rates in the 45–74 year age group, with the exception of the registers in South East England and Uruguay which found a lower rate (table 1).17 20
Median survival from onset was 2.9 years (95% CI 2.8 to 3.1) in incident patients. Female patients had a significantly shorter median survival compared with male patients (male 3.3, female 2.6; p=0.003). Bulbar onset (bulbar 2.3, spinal 3.4; p=4.51e−16) and old age (<60 years 4.4, >60 years 2.5; p=3.71e−18) were also associated with a shorter median survival. Multivariate analysis showed that a higher age at onset and a bulbar onset were independent predictors of a shorter survival. Gender was not independently associated with survival (p=0.46).
The highest male:female incidence rate ratios were found in the premenopausal age groups as well as in the >75 year age group (figure 2A). The prevalence rate ratios did not show a clear pattern with age (figure 2B). Although the male:female incidence rate ratio in the premenopausal age group was higher than in the postmenopausal age group (1.91 and 1.50, respectively), this difference was not significant (table 3).

{kind=link}
{kind=link}
Relationship between age group and gender ratio: (A) incidence rate ratio, (B) prevalence rate ratio.
Age and gender adjusted incidence according to menopause status
Discussion
This study reports on the epidemiology of ALS in a large prospective population based register, the first ALS register to use the capture–recapture methodology for each separate age and gender group, instead of only for the total population. The reliable age and gender specific incidence rates offered by this study method provide evidence that the rapid decrease in ALS incidence after 74 years of age is real, and may not be caused solely by under ascertainment in the elderly. This implies that the ALS incidence peak in the 70–74 year age group reflects a time period with maximal susceptibility, and that ALS is not merely the result of ageing. Furthermore, no clear evidence was found for a postmenopausal drop in the male:female ratio, suggesting that the protective role of female sex hormones in ALS is not as important as previously thought. Marked differences between an incident and prevalent ALS cohort were identified, which demonstrates the influence of including either incident or prevalent ALS patients when studying susceptibility or disease modifying factors.
Compared with population based studies with a large population size, the 81% coverage rate in our study was comparable or higher.28–30 This high coverage rate may be due to certain factors characteristic of The Netherlands. Firstly, although population size is large, the area is relatively small. With a population density of 491/km2, it is one of the most densely populated countries.25 Secondly, the Dutch healthcare system is of relatively high quality and there is no financial hurdle to obtaining access to healthcare. The physical distance to healthcare institutions is also small: mean distance to the nearest general practitioner is 1.1 km and to the nearest hospital only 7 km.31 It is therefore very likely that all patients with ALS will visit a doctor at least once during the course of their disease, so that every ALS patient in The Netherlands could potentially be ascertained by one of our sources. A last explanation for the high coverage rate is that the various medical institutions in The Netherlands are used to collaborating in neuromuscular medical research.
The incidence of ALS in The Netherlands is similar to incidence rates reported by other prospective population based registers, with the exception of a lower ALS frequency in South East England and Uruguay (table 1).17 20 As these registers did not use capture–recapture analysis, it is not clear to what extent these differences may have been due to under ascertainment. Application of capture–recapture methodology by future studies may provide more precise estimates of ALS risk, allowing for a better comparison between studies. Knowing whether the risk of developing ALS actually varies between different populations may result in a better understanding of its aetiology.
Susceptibility to ALS decreases rapidly after a peak has been reached in the 70–74 year age group (figure 1A). The incidence in this age group is almost four times that observed in the >85 year age group, which is in sharp contrast with the figures in a typical age related disease such as Alzheimer's dementia.32 Previous studies on ALS epidemiology also observed an incidence decrease in old age, and suggested that the decline could be attributed to difficulties in case ascertainment in the elderly.20 33 Because we applied the capture–recapture method in each separate age class, we were able to test this hypothesis. With a coverage rate of 52% in the >85 year age group, catchment in the very elderly is indeed lower (see supplementary table 1, available online only). However, the rapid decline was also observed in the present study, in which incidence rates were adjusted for differential coverage in different age and gender groups. It is therefore unlikely that the decrease is caused by under ascertainment in the elderly. Another reason for low incidence in the oldest age groups could be under diagnosis of the illness in these age groups. It might be more difficult to recognise ALS in older age groups, particularly as they may have other disorders.20 34 Furthermore, the decreased likelihood of referral or being seen by a neurologist may contribute towards under diagnosis.20 35 However, the Dutch healthcare system provides access to everybody without financial or geographical hurdles, so it is unlikely that under diagnosis of a devastating and disabling disease such as ALS in the elderly completely explains the substantial decrease in incidence. A third explanation might be that older ALS patients evade healthcare and all sources used in the current study. Nevertheless, based on our results, it is plausible that susceptibility to ALS decreases after 74 years of age. The peak may reflect a time period of maximal susceptibility determined by exposure to an environmental risk factor or its interaction with a genetic susceptibility.20 Another explanation is that ALS is exclusive to a small susceptible subpopulation, and that this population is substantially depleted beyond the age of 74 years by mortality from ALS or from other unrelated causes.36
Our study provides no clear evidence that the male:female ratio declines after menopause. This is not congruent with prior studies that showed a postmenopausal drop in the male:female ratio, suggesting a role for sex hormones in the aetiology of ALS.23 37 A relatively small study population and retrospective case ascertainment may have caused inaccuracy of male and female incidence rates in previous studies. To make accurate hypotheses on risk factors for ALS, unbiased epidemiological data are needed, which may be provided by large prospective population based registers applying the capture–recapture methodology. The present study, therefore, casts doubt on the hypothesis that physiological levels of sex hormones have an important role in motor neuron diseases, which is corroborated by the observations that oestrogen replacement therapy is not associated with the risk of ALS38 and that only high supraphysiological levels of oestrogens are able to protect motor neurons in vitro.39
Patient characteristics, which were comparable with other population based studies,12–21 showed large differences between the incident and prevalent cohort of ALS patients, confirming previous observations.33 The incident ALS cohort had a higher median age at onset (63.0 vs 58.1 years) and at diagnosis (64.7 vs 60.4 years), a shorter median time to diagnosis (343 vs 477 days) and more bulbar onset patients (30.0% vs 19.1%). Differences are probably caused by the shorter survival associated with bulbar onset disease and disease onset at old age, which makes patients with bulbar onset disease and higher age at onset less likely to be entered into a study including only prevalent cases. These observations underscore the importance of including incident rather than prevalent cohorts when studying susceptibility or disease modifying factors in ALS. An example is the reported effect of kinesin associated protein 3 (KIFAP3) on ALS survival in a prevalent cohort, which could not be replicated in an incident cohort.40 41
Exact confirmation of diagnosis of the small subset of patients unique to the Dutch Association for Neuromuscular Diseases was impossible due to privacy regulations. Patient organisations cannot acquire personalised medical information, which will be true for many other alternative sources that register ALS patients outside hospitals. Although this slightly impacts on the accuracy of diagnosis, using only one source (ie, neurologists and consultants in rehabilitation medicine) would have resulted in a less precise estimation of ALS epidemiology.
In capture–recapture methodology, the intersection of the two sources relative to the cases that are unique to each source are crucial to the estimate of the unknown total population. It is widely accepted that one important assumption for this methodology—that is, independence of sources—is practically impossible.24 42 Positive dependence between sources implies that the number of cases is being underestimated, and negative dependence leads to an overestimate. In the current study, it is plausible that some positive dependence exists between the two sources used, as patients who visit hospitals and rehabilitation centres also get information regarding the national patient organisation. Even with positive dependence, however, it was previously shown that an accurate prevalence estimate could be made in Huntington's disease by using the capture–recapture methodology.42 An analysis based only on the actual total number of observed patients will result in a greater underestimation of incidence and prevalence rates. Application of the capture–recapture methodology, therefore, provides more useful information about ALS epidemiology.
Acknowledgments
The authors thank Petra Berk, PhD, Hermieneke Vergunst and Dorien Standaar for providing assistance in collecting data and performing data entry.
References
Supplementary materials
Web Only Data
Files in this Data Supplement:
Footnotes
See Editorial commentary, p 1066
JHV and LHvdB contributed equally to the manuscript.
Linked article 246876.
Funding This project was funded by the Prinses Beatrix Fonds, VSB fonds, H Kersten and M Kersten (Kersten Foundation), The Netherlands ALS Foundation and J R van Dijk and the Adessium Foundation. The research leading to these results has received funding from the European Community's Health Seventh Framework Program (FP7/2007–2013) under grant agreement No 259867.
Competing interests LHvdB received travel grants and consultancy fees from Baxter.
Ethics approval This study was conducted with the approval of the institutional review board of the University Medical Centre Utrecht.
Provenance and peer review Not commissioned; externally peer reviewed.