Article Text

Abstract
Background Primary progressive aphasia (PPA) is a clinical syndrome characterised by progressive decline in components of the language system. Recent evidence suggests that the logopenic/phonological (LPA) variant is a reliable in vivo marker of Alzheimer related pathology. The aim of this study was to determine if patients with clinically typical early stage Alzheimer's disease (AD) display a characteristic language disorder that resembles LPA, or if LPA is a clinical manifestation of an atypical form of AD.
Methods Spoken language samples were obtained using the Cookie Theft picture description task from 18 post mortem confirmed cases of AD, where speech samples were taken at the first point of clinical diagnosis, and 18 post mortem confirmed healthy controls. Spoken samples were transcribed from tape recordings and analysed using the scoring system described by Wilson et al.
Results Group comparisons between normal controls and AD patients showed no significant overall differences. Individual review of the linguistic variables compared with the PPA variants showed that a third of patients had normal language (n=6). The remainder showed varied patterns of linguistic impairment. In the majority of the affected group, the most salient feature was a reduction in one or more measures of syntactic complexity. One patient's deficit was comparable to that found in LPA.
Conclusions The impairment found in clinically typical early stage AD did not correspond consistently to the linguistic profiles described in any of the sub-syndromes of PPA. The only reliably distinguishing feature was a reduction across a range of syntactic complexity measures. The findings suggest that LPA represents an atypical clinical presentation of AD rather than a common clinical feature of typical AD.
Statistics from Altmetric.com
Introduction
Primary progressive aphasia (PPA) is a clinical syndrome seen in patients with neurodegenerative disorders in whom cognitive decline is limited to one or more components of the language system.1 ,2 Since Mesulam's first description of the phenomenon,3 clinical, neuropsychological and imaging studies have converged on the existence of three distinct clinical subtypes: one, characterised by fluent but empty speech, impaired single word comprehension and a high incidence of surface dyslexic errors on single word reading, in association with selective atrophy in one or both anterior temporal regions, corresponds to the syndrome of semantic dementia (also known as semantic variant PPA or as PPA semantic). A second major subgroup meets criteria for progressive non-fluent aphasia (PNFA; also known as non-fluent/agrammatic variant PPA or as PPA agrammatic), with phonologically and/or grammatically distorted speech output, preserved single word comprehension, and atrophy focused on the left inferior frontal and insular regions. Speech output in the third group of patients is characterised by a slow production rate, long word finding pauses, sparse phonological paraphasias and difficulty with sentence (but not single word) repetition. This group is now referred to as logopenic/phonological progressive aphasia (LPA; also known as logopenic variant PPA or as logopenic PPA). Structural and/or functional imaging reveals abnormalities in more posterior brain regions.4–8
Wilson et al9 analysed samples of connected discourse that had been obtained from patients with these three variants and found that each showed a distinctive profile of performance. Patients with semantic dementia used more closed class words, more verbs and high frequency nouns while speech rate was normal and there were few phonological or syntactic errors. By contrast, those with PNFA produced fewer words per minute, and committed phonological and syntactic errors. The speech of patients with LPA was associated with features of both PNFA (phonological and syntactic errors) and semantic dementia (impaired lexical access), although to lesser degrees.
Studies of the pathological correlates of PPA suggest that the majority of cases with semantic dementia and PNFA are associated with non-Alzheimer (tau or TDP43 based) neurodegenerative pathology,6 ,10 ,11 although a small number reflect atypical presentations of Alzheimer's disease (AD).12–14 In contrast, biochemical, amyloid imaging and post mortem findings in LPA support the idea first advanced by Gorno-Tempini et al that the syndrome is a clinical marker of AD pathology.5 ,15 ,16
In light of the association between the syndrome of LPA and AD pathology, it is reasonable to ask whether the inverse association also holds, such that patients with clinically typical AD display a characteristic language disorder that resembles LPA but is overshadowed by a more prominent deficit in new learning. This association would mirror that between the posterior cortical atrophy variant of AD (in which early and disproportionate pathological involvement of parieto-occipital cortical regions gives rise to a prominent visuospatial disorder)17 and the more subtle posterior cortical dysfunction that is often detectable in the early stages of clinically typical AD.18 The absence of such an overlap would support the suggestion that LPA should be regarded as one of the atypical presentations of AD.19
To obtain a definitive answer to this question, the present study drew on data from patients with early stage clinically typical AD, in whom language and general cognition had been systematically studied during life, and AD pathology confirmed after death. These antemortem language samples obtained from patients prior to postmortem pathological confirmation of AD, form part of an extensive behavioural and biological data archive assembled in the course of a longitudinal investigation of the clinical and histopathological correlates of normal and late life cognitive ageing.
The analytical method was based on the techniques used by Wilson et al in their PPA study.9 By applying the same set of methods to speech samples obtained from patients at a uniform stage of clinically typical AD, the aim of this study was to determine whether a common or dominant pattern of abnormalities would emerge and, if so, whether or not this pattern was similar to the profile described in LPA.
Methods
Study population
Data were obtained from the Oxford Project to Investigate Memory and Ageing (OPTIMA), a longitudinal cohort study involving subjects with possible and probable AD, other dementia syndromes, and cognitively normal elderly volunteers.
On entry to the study, all participants are evaluated using the Cambridge Mental Disorders of the Elderly Examination interview (CAMDEX),20 undergo structural brain imaging, blood and CSF sampling, and are invited to enrol in a brain donation programme. Assessment procedures are repeated at 6–12 month intervals. Selected parts of the CAMDEX are tape recorded for offline analysis, scoring and archiving. After each episode an updated diagnosis is agreed by an expert clinical panel, using standard diagnostic criteria: the National Institute of Neurological Communicative Disorders and Stroke and the Alzheimer's Disease and Related Disorders Association (NINCDS-ADRDA)21 criteria are used for AD, and the Petersen criteria for mild cognitive impairment (MCI).22 Follow-up and diagnostic review continues until death, allowing clinical and neuropsychological findings to be correlated with those of postmortem brain examination if consent was granted.
The data for the present study were the scores and audio recordings of two sets of CAMDEX assessments: (1) AD converter samples were those obtained from subjects classified at entry as either cognitively normal or MCI, at the point when the clinical classification was changed to probable AD (corresponding to early stage AD) and in whom definite AD was later confirmed at postmortem. All available audio recordings of this assessment in subjects meeting these criteria were used for the study. Two subjects had entered the cohort while cognitively normal, and the remainder with MCI. (2) Control samples were obtained from a similar number of participants, matched as closely as possible to the AD group for age, sex, education and number of prior CAMDEX assessments, who were judged to be cognitively intact at every visit and in whom postmortem examination was later found to be compatible with normal brain ageing. Subjects in both groups were native speakers of British English, without a prior history of major medical or psychiatric illness, stroke, alcoholism or major head injury.
Since its inception in 1988, more than 1000 people have enrolled in OPTIMA. Of the 543 who have so far been followed-up until death, postmortem examination was carried out on 394 (72.6%). The sample size available for this study was restricted by the selection criteria detailed above and by the degraded quality of some of the audio tapes (see figure 1 for detailed illustration of subject attrition).
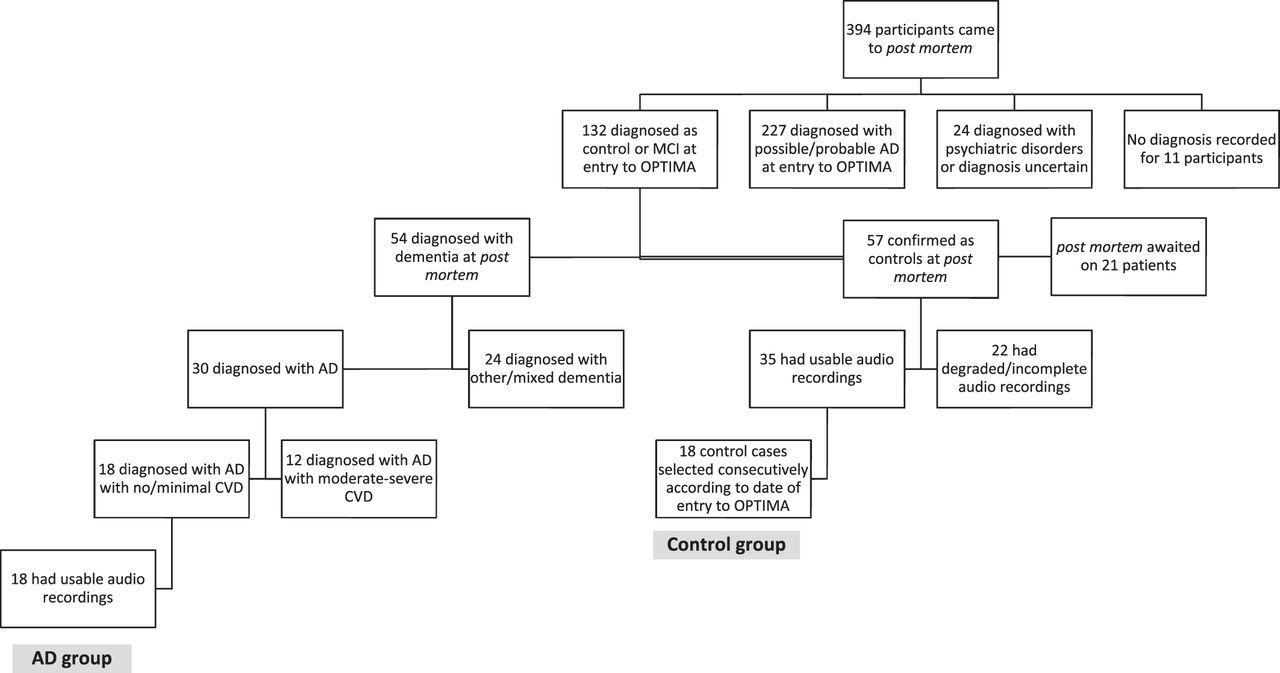
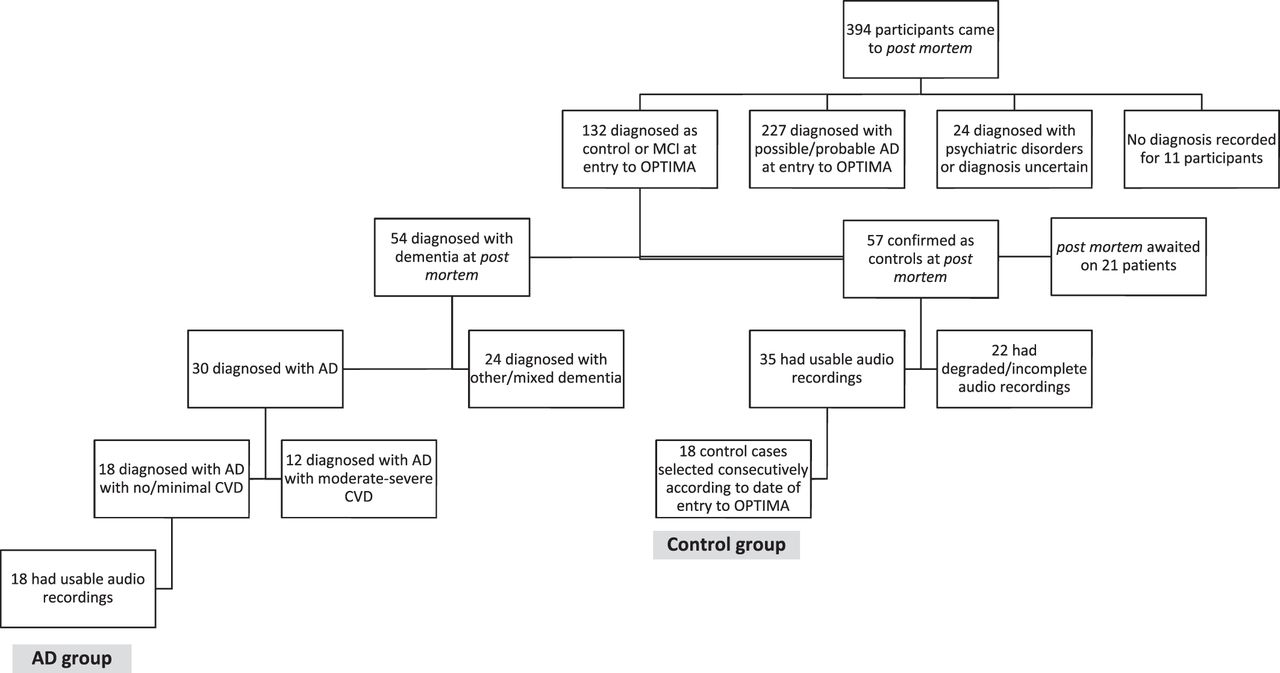{kind=link}
Flowchart to illustrate subject attrition due to selection criteria. AD, Alzheimer's disease; CVD, cardiovascular disease. MCI, mild cognitive impairment; OPTIMA, Oxford Project to Investigate Memory and Ageing.
Study approval
Ethics approval for the study was granted by the Central Oxford Research Ethics Committee and the Frenchay Research Ethics Committee (study reference 09/H0107/9). Written informed consent was obtained from all participants.
Spoken language samples
The cognitive subsection of the CAMDEX (CAMCOG) consists of eight subscales (relating to domains of orientation, language, memory, attention, praxis, calculation, abstract thinking and perception) and incorporates the Mini-Mental State Examination.23 The language subtest includes elicitation of a sample of connected speech using the Cookie Theft picture from the Boston Diagnostic Aphasia Examination.24 This widely used task requires the participant to ‘describe what is going on’ in a black and white line drawing of a domestic scene depicting a daydreaming woman standing at an overflowing sink with her back to a boy, who is falling off a stool as he reaches up to steal cookies from a tin, encouraged by his sister.
The subjects' picture descriptions were transcribed from tape following the conventions set out by Garrard et al.25 The picture description task should ideally elicit a monologue by the subject, but in practice the subject is often heard asking questions about the task (such as ‘is that all right?’) and the examiner supplying comments, prompts or ‘back channel signals’ (such as ‘mmhmm’ or ‘yes’).26 Although all recorded speech was transcribed, the analysis was carried out on the participants' narrative utterances only.
Language analysis
Analysis of transcribed language samples followed the methods used by Wilson et al9 to characterise connected speech in patients with variants of PPA. These methods are based on the phenomenological classification of normal and abnormal discourse proposed by Saffran et al,27 and employ the quantitative production analysis (QPA) approach described by Berndt et al.28
Transcripts were independently analysed by two raters, who showed high inter-rater agreement. Disagreements between raters were resolved after discussion by all of the authors. On one measure (semantic errors), however, consensus proved difficult to achieve: the operational definition of ‘sentences that were syntactically well formed, but were either nonsensical or semantically inappropriate for the context’ was found difficult to apply consistently. This measure was therefore omitted from the analysis.
The variables that were assessed can be considered under four headings: (1) speech production (speech rate, distortions and phonological paraphasias); (2) syntactic complexity (mean length of utterance, proportion of words in sentences, number of embedded clauses, syntactic errors, nouns preceded by determiners and verbs with inflections); (3) lexical content (proportional frequencies of open class (nouns, verbs and descriptive terms) and closed class (grammatical function) words); and (4) fluency errors (false starts, repaired sequences, filled pauses and incomplete sentences).
Statistical analysis
Individual variables were checked for normality and homogeneity of variance assumptions for parametric statistics. Independent sample t tests or non-parametric Mann–Whitney U tests with Bonferroni corrected p values were used accordingly to compare neuropsychological and linguistic measures between controls and AD patients. Individuals' performances on each of the linguistic variables were converted to z scores using the control means and SDs. Impairment was categorised as mild (1.5 SDs below the control mean), moderate (2.0 SDs below the control mean) or severe (2.5 SDs below the control mean).
Results
Background characteristics of the two subject samples
There were no significant differences between the subjects in the control and AD groups in terms of age, education, gender ratio or number of Cookie Theft descriptions completed before the index assessment. The Mini-Mental State Examination scores, and performance on 10 out of the 11 CAMCOG subtests obtained from subjects with AD were significantly lower than those of controls. Group means for all of these measures are presented in table 1. Multiple linear regression analyses were performed to identify the impact of demographic variables on QPA measures. Non-linear variables were corrected by log10 transforming the data and adding a constant of 0.5 to values of zero. Where data were skewed at zero, scores were categorised in a binary manner (error, no error) and binary logistic regression applied. The results of these analyses showed that age significantly predicted the proportion of verbs, verbs with inflections, pronouns and phonological paraphasias but neither age nor education significantly predicted performance on any other QPA variable. Subsequent group comparisons of these variables were adjusted for age using univariate analysis of variance.
Demographic characteristics and CAMCOG scores, subdivided by cognitive domain, for normal controls and Alzheimer's disease cases at first episode of diagnosis
QPA variables: group and individual case analysis
Group analyses revealed no significant differences between AD patients and controls on any of the QPA measures, after correction. It is likely, however, that language abnormalities in AD may not only be milder but more heterogeneous than those seen in PPA, masking differences between the AD and control groups. Data from the 18 AD cases were therefore analysed individually in order to identify common profiles of linguistic impairment (table 2). To address the question of whether the profiles obtained from the present group of clinically typical AD patients were similar to those described in the three variants of PPA, group z scores for semantic dementia, PNFA and LPA were calculated using the patient and control means and SDs reported by Wilson et al.9
Individual case analysis of linguistic profiles in AD with primary progressive aphasia variants
For descriptive purposes, mild impairment (denoted as ‘+’ in table 2 and representing 1.5 SDs below the control mean), was judged to be within the normal range, and therefore was not included in the descriptions of the profiles of connected speech. In table 2, therefore, cells containing ‘+’ or ‘+++' denote moderate to severely impaired features of language. Inspection of table 2 reveals that the AD patients fall into a number of distinct subgroups.
No aphasia
Six AD patients (33% of the total group) showed no impairment on any of the linguistic indices measured.
Logopenic aphasia
A single patient (AD2) revealed a profile of linguistic impairment similar to that of LPA, as described by Wilson et al.9 Patient AD2 showed reduced speech rate, without speech errors, fluency errors, changes in lexical content or reduced syntactic complexity.
Impaired fluency
Two AD patients made isolated fluency errors. The discourse of patient AD4 contained an increased number of filled pauses whereas patient AD18 made successive numbers of false starts.
Reduced syntactic complexity
Six AD patients (33% of the total group) showed isolated, moderate to severe, reduction in at least one aspect of syntactic complexity. All six patients showed either a reduction in the proportion of words in sentences, or syntactic errors, or both, similar to errors seen in PNFA and LPA. These AD cases also showed an additional varied decrease in the proportion of nouns with determiners and/or verbs with inflections, a characteristic not seen in any of the PPA variants.
Reduced syntactic complexity with additional features
Three AD patients showed a reduction in syntactic impairment, as described in the previous group, with additional impairment. Patient AD11 showed an additional reduction in speech rate, patient AD13 showed additional fluency errors and patient AD15 displayed additional severe changes in lexical content.
Discussion
By applying a well validated assessment protocol to connected speech samples obtained from patients with newly diagnosed AD (which was later pathologically confirmed), this study identified the abnormalities of connected speech characterising the early stages of clinically typical AD. The neuropsychological profile of all patients in the AD group at the time of the assessment revealed impairments in learning and recent memory, confirming a typical clinical profile, rather than any of the atypical presentations that have been described.12
A straightforward group comparison revealed no overall differences between AD and control discourse. Unlike the language deficits associated with variants of PPA, those associated with the AD patient population are more likely to be sparse and heterogeneous and, accordingly, there was no single prototypical pattern of impairment. Individual case analyses showed that, at initial examination, a third of patients were found to have no linguistic deficits, suggesting that features of aphasia are not a universal finding in the early stages of typical AD. Linguistic abnormalities were detected in the remainder of the AD patients, similar to a previously reported prevalence of language deficits at this early stage in clinically typical AD.29 Deficits were characterised by features of LPA, PNFA and semantic dementia, but to varying degrees and with no single homogeneous profile. This could be explained partly by the variability in pathological load and distribution, and partly by the fact that the samples were obtained early in the course of AD when there are fewer deficits overall.
The most frequently occurring feature of the AD patients' language was a reduction in one or more measures of syntactic complexity, identified in 10 of the 12 affected patients. AD patients showed a reduction in the proportion of words in sentences and increased syntactic errors (as described in PNFA and LPA), but in contrast with all three PPA variants, they also showed a reduction in the proportion of nouns with determiners and verbs with inflections.
The finding of a syntactic irregularity in these samples is in agreement with previous studies of discourse in AD that have examined this measure of linguistic performance. Croisile et al30 found ‘simplified but relatively correct syntax’ in Cookie Theft descriptions in probable AD, although the effect was more pronounced in written than oral descriptions. Hier et al31 also described reduced syntactic complexity in oral descriptions and found that the mean clause length was shorter in AD than in vascular dementia. Garrard et al32 found some evidence for syntactic change in an analysis of Iris Murdoch's final novel, written shortly before clinical evidence of AD emerged. Kempler et al33 documented the absence of syntactic errors in the early stages of AD although formal analysis of syntactic complexity was not performed and the data considered were single written sentences rather than transcripts of connected speech.
Two AD patients deviated from the syntactic profile and made isolated fluency errors. Errors were largely restricted to false starts and filled pauses, which may reflect difficulties in generating grammatical structures or word finding difficulties.9
The absence of speech sound errors together with consistent and pervasive fluency or lexical content related differences indicated that the profile of language in early stage AD was distinct from any of the three variants of PPA, and most particularly from the LPA variant, with a single exception. Patient AD2 presented with a profile of reduced speech rate, severe fluency errors and changes in lexical content and syntactic complexity, as were noted by Wilson et al9 in a group of LPA patients. The linguistic changes shown by patient AD2 were less severe in the affected domains but the deficits were nonetheless comparable with LPA. To clarify, the aim of the study was to determine whether an LPA-like language phenotype (not LPA per se) can be identified in the context of typical AD, and therefore we did not expect to find significant numbers of atypical clinical presentations in this sample of clinically typical AD patients.
The present study has unique and important strengths: the availability of postmortem confirmation in members of the AD group; the opportunity to select a language sample from a longitudinal dataset such that all patients were examined at the point at which they first met the clinical criteria for AD; and the availability of a matched group of histologically confirmed controls.
The advantages of diagnostic certainty and uniformity of clinical stage are, to some degree, tempered by the relatively small number of samples available for analysis, and the absence of lexical data relevant to semantic memory impairment—a clinical feature of early AD that is well documented in studies using methods based both on single word stimuli34–36 and connected speech analysis.37
In response to these observations we would point out that for studies aiming to characterise clinical correlates, diagnostic uniformity is a sine qua non and sample size is always limited by strict adherence to diagnostic criteria. For exactly these reasons, the numbers per group included in the studies of Wilson et al9 and others5 ,6 ,38 ,39 were of similar magnitude. Second, if an excess of semantic errors had been documented, then the profile obtained for the patients in our sample would have remained distinct from any of the PPA profiles. Current work is, however, being undertaken to assess semantic content in this patient cohort, and will help to rectify this omission.
In conclusion, therefore, and in answer to the question posed by the title of this paper, the data support the classification of LPA as an atypical clinical presentation of AD rather than an invariant clinical feature of the typical form of the disease.
Acknowledgments
We thank Clare Bateman and Samuel Hinton for assistance with transcriptions and Lucy Hiscox with the coding. We thank all study participants and their families, without whose long term commitment this study could not have occurred. Similarly, we wish to thank Professor A David Smith, founder and former director of OPTIMA, who set up this longitudinal cohort study, and Professor Gordon Wilcock, Project Director, who kindly agreed to share the data with the authors, and the OPTIMA nurses and staff who contributed to the data collection and neuropsychological assessment of the participants.
References
Footnotes
Funding This work was supported by UK Medical Research Council research grant No G0801370, awarded to PG and CAdJ.
Competing interests None.
Ethics approval The study was approved by the Southampton and West Hampshire research ethics committee.
Provenance and peer review Not commissioned; externally peer reviewed.