Article Text

Abstract
Objective Our objective was to study the hypothalamic volume in a cohort of patients with amyotrophic lateral sclerosis (ALS) including symptomatic and presymptomatic ALS mutation carriers.
Methods High-resolution three-dimensional T1-weighted MRI datasets from 251 patients with sporadic ALS, 19 symptomatic and 32 presymptomatic ALS mutation carriers and 112 healthy controls (HC) were retrospectivally registered for manual delineation of the hypothalamus. The volume of the hypothalamus, in total or subdivided, was normalised to the intracranial volume and adjusted to age. Correlation analyses were performed with clinical and metabolic outcomes. Pathologically defined ALS stages were determined in vivo by diffusion tensor imaging (DTI).
Results We observed a severe atrophy of the hypothalamus both in patients with sporadic ALS (−21.8%, p<0.0001) and symptomatic ALS mutation carriers (−13.4%, p<0.001). The atrophy in patients with sporadic ALS was observed in both the anterior (−27.6% p<0.0001) and the posterior parts of the hypothalamus (−17.7%, p<0.0001). Notably, this atrophy was also observed in presymptomatic ALS mutation carriers (−15.5%, p<0.001) and was unrelated to whole brain volume atrophy or disease stage as assessed using DTI or functional status. Hypothalamic volume was correlated with body mass index (BMI) in patients with sporadic ALS (p=0.0434, ρ=+0.1579), and this correlation was much stronger in patients with familial ALS (fALS) (p=0.0060, ρ=+0.6053). Anterior hypothalamic volume was correlated with age at onset, but not with survival after MRI.
Conclusions Hypothalamus is atrophied in ALS, even in premorbid stages, and correlates with BMI, especially in fALS. Decreased anterior hypothalamic volume is associated with earlier onset of disease.
Statistics from Altmetric.com
Introduction
Amyotrophic lateral sclerosis (ALS) and frontotemporal dementia (FTD) are commonly considered as parts of a pathophysiological continuum. Both diseases clinically overlap, with patients with ALS developing moderate FTD-like symptoms and, conversely, patients with FTD developing motor neuron neuropathology during the time course of the disease.1 2 Moreover, patients with ALS and FTD also share mutations in identical genes and similar molecular neuropathology.1 2
Disturbed energy homeostasis is a hallmark of ALS. Patients with ALS are generally lean with normal or low body mass index (BMI) preceding onset of motor symptoms.3 4 The extent of weight loss5 6 and metabolic status evaluated by circulating lipids7or fat distribution8 are prognostic markers of ALS. The causes of weight loss in ALS are multifactorial and include dysphagia and hypermetabolism.9 10 Importantly, increasing energy content of the diet increased survival of ALS mouse models,11 and showed efficacy in a pilot clinical trial in gastrostomised patients with ALS12 as well as in a longitudinal register of PEG-implanted patients.13 Recently, patients with ALS were shown to display altered eating behaviour.14 15 Suggestive of a hypothalamic involvement in ALS, levels of AgRP, a strongly orexigenic hypothalamic neuropeptide, were increased in mouse models of ALS, while levels of its antagonist pro-opiomelanocortin were decreased,16 and two studies observed pathological abnormalities in the hypothalamus of patients with ALS.17 18 On the functional level, patients with ALS did not gain weight in response to pioglitazone, a drug known to increase food intake through hypothalamic relays.16 19
Alteration in appetite and food preference is a major symptom of the behavioural variant (Bv) of FTD, in particular a marked preference for sucrose-rich foods.20–23 In bvFTD, this is associated with marked hyperphagia, leading to weight gain24 as well as increased energy expenditure22 Similar to the situation in ALS, levels of AgRP were increased in patients with bvFTD20 and several MRI-based studies have observed up to 15% atrophy of the hypothalamus, especially of its posterior part, in patients with bvFTD.20–23 Thus, disease progression of bvFTD involves hypothalamic atrophy potentially leading to abnormal eating behaviour.10
There is currently no information available on hypothalamic volume in patients with ALS. One recent study observed pTDP43 pathology in the lateral hypothalamus of patients with ALS.18 Thus, it remains unknown whether any hypothalamic atrophy in humans might precede metabolic problems typical of ALS or even motor symptoms themselves. Importantly, weight loss itself is premorbid in patients with ALS,3 4 and therefore neurological substrates of abnormal energy metabolism should precede motor symptoms. Here, we retrospectively performed a MRI-based quantitative analysis of the hypothalamic volume in 270 patients with ALS and 32 presymptomatic ALS mutation carriers in comparison with 112 healthy controls (HC). We hypothesised that the hypothalamus volume in patients with ALS is altered in relation to disease status and metabolic indices, and we asked whether an abnormally reduced hypothalamic volume is possibly present prior to onset of ALS-defining symptoms.
Materials and methods
Study samples
A total of 414 subjects were monocentrically recruited in the Department of Neurology, University of over 4 years between 2012 and 2016. All subjects provided their written informed consent. The study had been approved by the Ethics Committee of the University of Ulm (references #19/12 and #20/12). Patients with sporadic ALS (n=251), symptomatic (n=19) and presymptomatic ALS mutations carriers (n=32) underwent MRI scans at enrolment (for details of the scanning protocols, see MRI acquisition), together with standardised clinical, neurological and laboratory examinations, distant from <3 months of the MRI session. The diagnosis of all cases was made by a motoneuron disease specialist according to the El Escorial diagnostic criteria.25 None of the patients with ALS or presymptomatic ALS mutations carriers had any history of other neurological or psychiatric disorders. The symptomatic ALS mutation carriers (n=19) were recruited from families with a positive history of ALS and had patients positive genetic testing, and the remaining 251 patients with ALS did not have any known ALS-associated gene mutation and were considered as sporadic ALS cases. All data for HC (n=112) were obtained from a normal database. Demographic and clinical features of all participants are summarised in table 1.
Demographic and clinical characteristics
MRI acquisition
The study used two different protocols for whole-brain-based morphological data and diffusion tensor imaging (DTI) acquisition.
The data for 77 patients with ALS and 41 controls were acquired at a 3.0 T MRI scanner (Allegra Siemens Medical, Erlangen, Germany). Morphological data were obtained using a high-resolution 3-D T1-weighted magnetisation-prepared gradient echo image (MPRAGE) sequence (192 sagittal slices, no gap, 1.0×1.1×1.0 mm3 voxels, 256×192×256 matrix, TE=4.7 ms, TR=2200 ms). The DTI study protocol consisted of 49 gradient directions, including one b0 gradient direction (no gap, 2.2 mm3 isovoxels, 96×128×52 matrix, TE=85 ms, TR=7600 ms, b=1000 s/mm2).
The data for 193 patients with ALS, 32 presymptomatic ALS mutation carriers and 71 controls were acquired at a 1.5 T clinical MRI scanner (Symphony, Siemens Medical, Erlangen, Germany). Morphological data were obtained using a MPRAGE sequence (144 sagittal slices, no gap, 1.0×1.2×1.0 mm3 voxels, 256×192×256 matrix, TE=4.2 ms, TR=1600 ms). The DTI study protocol consisted of 52 gradient directions, including four b0 gradient directions (no gap, voxel size 2.0×2.0×2.8 mm3, 128×128×64 matrix, TE=95 ms, TR=8000 ms, b=1000 s/mm2).
Hypothalamic volumetry
MPRAGE images were used for manual delineation of the hypothalamus in the coronal plane using a well-established landmark-based procedure (figure 1A).26 The Tensor Imaging and Fiber Tracking software package,27 recently expanded by a volumetric extension package,28 was used for volumetric analysis of the hypothalamus (for details, see Hypothalamic delineation procedure) for each of the 414 subjects in a three-step processing pipeline: (1) rigid brain normalisation, (2) spatial upsampling into a study-specific grid (in-plane resolution of 62.5×62.5 µm2, slice thickness of 0.5 mm) to improve the accuracy in identifying landmarks and hypothalamic borders (for details, see online supplementary material), and (3) manual delineation of the left and right hemispheric hypothalamus. In particular, rigid body normalisation was performed along the anterior commissure (AC)–posterior commissure (PC) axis such that the coronal cutting plane was perpendicular with respect to the AC–PC axis. The rigid body transformation approach (1) preserves the amount of hypothalamic volume, (2) corrects for individual-based tilt of the head in order to ensure coronal slicing in a common space for all subjects and (3) minimises potential partial volume effects. Prior to the analysis, all 414 datasets were randomised such that the rater was blinded to all demographic and clinical features. Grey matter and intracranial volume (ICV) were directly determined by the build-in ‘tissue volumes’ utility of the MATLAB (R2014b, The MathWorks, Natick, Massachusetts, USA) based Statistical Parametric Mapping 12 (SPM12) software (Wellcome Trust Centre for Neuroimaging, London, UK).29
Hypothalamic delineation procedure
The hypothalamus was manually delineated using an advanced, robust and highly reproducible technique that was adapted from Gabery et al 26 (figure 1A,B). The delineation procedure was based on well-defined boundaries that were visualised in coronal sections of human postmortem hypothalamic tissue30 Accordingly, the most anterior coronal slice was defined when the optic chiasm was first seen to be attached to the ventral part of the septal area (figure 1C, left panel) and the most posterior slice was determined by the coronal section where the fornix appears to be merged with the mammillary nucleus (figure 1C, right panel). The AC defines the inferior–superior boundary for the anterior hypothalamus in the telencephalic preoptic area, and the hypothalamic sulcus defines a major landmark for the superior border posterior to the AC for the posterior regions26 31 (figure 1C). The hypothalamus was medially bounded by the third ventricle, the inferior border was defined by the junction of the optical chiasm for the anterior part, and by the border of the cerebrospinal fluid for the more posterior slices (figure 1C). The hypothalamus was laterally bounded by the diagonal band of Broca in the preoptic area, the internal capsule and the cerebral peduncle for the more posterior slices together with non-hypothalamic grey matter structures such as the fields of Forel on the most posterior slices (figure 1c, right panel). The optical tract was excluded from all slices. This delineation procedure is robust and achieves a high level of reproducibility as indicated by an intrarater and inter-rater reliability analysis in a subsample of 12×3=36 randomised data sets. The coefficient of variation (CV) was CV<4% for both raters (MG and PV) and was considered as acceptable.26 The intraclass correlation coefficient (ICC) between the two raters was >0.9 (n=12, Pearson’s r=0.93, p<0.0001) in accordance with others.21 23 26 The MRI protocol (either 1.5 T or 3.0 T) did not influence the volumetric analysis.

Volumetric analysis of the hypothalamus. Example of the delineation of the hypothalamus in one representative healthy subject (female, 58 years) based on 1.5 T high-resolution magnetisation-prepared gradient echo image (MPRAGE) data (voxel size: 1.0×1.2×1.0 mm3). The delineation technique was optimised from Gabery et al 26 with respect to the lateral boundary definition.31 (A) Coronal slice (resampled slice thickness of 0.5 mm) through the most anterior part of the hypothalamus from the left hemispheric part (resampled in-plane resolution 62.5×62.5 µm2). (B) Delineation was performed on a consecutive sequence of coronal slices in anterior–posterior direction. Then, the hypothalamus was subdivided into an anterior and posterior part using the criteria reported by Piguet et al 21 (C) Consecutive sequence of each second coronal slice in anterior–posterior direction showing the boundaries (yellow line) used to delineate the hypothalamus. The hypothalamic sulcus (*) was used as a landmark to define the superior boundary, the hypothalamus was laterally bounded by the internal capsule (ic) and non-hypothalamic grey matter areas (see methods for details); the most anterior slice (left panel) was defined where the optic chiasm is first seen to be attached to the ventral part of the septal area, and the most posterior slice (right panel) was defined where the fornix (fx) appears to be merged with the mammillary body (MB). The optical tract (OT) was excluded from all slices. 3V, third ventricle; AC, anterior commissure; DB, diagonal band; FF, fields of Forel; Th, thalamus.
Volumetric analysis
Given the distinct structural connectivity and potentially ALS-related selective vulnerability of the hypothalamus,16 we performed anterior–posterior segmentation (figure 1B) using a technique that was adapted from.21 All volumes, that is, (1) the total volume, (2) the volumes for the anterior and (3) posterior hypothalamus, were corrected for gender dimorphism, ICV and age in a linear regression model according to Nordenskjöld and collaborators.32
Assessing disease status using DTI
We used the well-established fibre tract-based DTI staging procedure introduced by our group33 in order to classify in vivo the disease stage of all patients with ALS using DTI-based fibre tracking. We used our standardised and well-established procedure to control for different protocols and different scanner.34
Statistics
The statistical software package Prism (GraphPad, USA) was used for statistical data analysis. One-way analysis of variance (ANOVA) was performed in cases of three or more groups, followed in the event of significance (p<0.05) by post hoc testing using an unpaired Student’s t-test for unequal variances. Spearman’s rank order correlation coefficient was used to study possible relationships between volumetric measures and clinical scores for the patient groups. Spearman’s rank order correlation test was preferred over Pearson correlation test because multiple datasets, including BMI and age at onset failed to pass the Kolmogorov-Smirnov normality test. All statistical tests were two sided with p<0.05 indicating statistical significance.
Results
In this volumetric study, 251 sporadic ALS cases, 19 symptomatic, 32 presymptomatic mutation carriers and 112 HC were included in the data analysis. Median value of revised ALS Functional Rating Scale (ALSFRS-R) was 41, suggesting that the majority of patients included were relatively early in their disease course. Overall, our results show that ALS is associated with a severe global atrophy of the hypothalamus that is already detectable in presymptomatic ALS mutation carriers.
Hypothalamic volumes of all included individuals were manually delineated as illustrated in figure 1. MRI scans were obtained on 1.5 T (n=296) and 3 T (n=118) scanners, and the results of the volumetric analysis at the group level were controlled for different MRI protocols (1.5 T and 3 T, different slice thickness of the sagittal slices—1.1 mm for 3 T and 1.2 mm for 1.5 T) by resampling into a common 1 mm isogrid prior to preprocessing (for details, see online supplementary material)—a previously validated approach within a multicentric framework to deal with different scanners and protocols.35 No significant effect of the different protocols for volumetric results at the group level could be identified (online supplementary figure S1). Since previous evidence observed larger hypothalamus in men,36 we corrected volumes for gender, as well as ICV and age in a linear regression model (online supplementary figure S1). The hypothalamic volume of patients with sporadic ALS (mean+SD: 696±125 mm3) was significantly smaller (one-way ANOVA followed by unpaired Student’s t-test, p<0.0001) by 21.7% than those of HC (889±133 mm3, figure 2A). This atrophy was also present in the symptomatic ALS mutation carriers (750±109 mm3) included (vs controls: −15.7%, p=0.0004) (figure 2A). Most importantly, the atrophy was already present in presymptomatic ALS mutation carriers (767±132 mm3, vs controls: −13.7%, p<0.0001). The anterior hypothalamus (−27.4%, p<0.0001 figure 2B), as defined by Piguet and collaborators,21and the posterior hypothalamus (−17.3%, p<0.0001, figure 2C) were smaller in patients with sporadic ALS than in HC. Posterior hypothalamus (−15.1%, p=0.031) and anterior hypothalamus showed similar atrophy (−16.4%, p=0.008) in symptomatic ALS mutation carriers. Both subregions were smaller in presymptomatic ALS mutation carriers (−10.7%, p<0.0001 and −17.6%, p<0.0001 respectively).

Severe hypothalamic atrophy in ALS volume of the total (A), anterior (B) and posterior (C) hypothalamus in healthy controls (HC black dots, n=112), sporadic ALS cases (grey dots ALS, n=251), symptomatic (fALS, n=19) and presymptomatic ALS mutation carriers (PS-fALS, n=32). The different gene mutations are colour coded according to the legend in panel A. All volumes (shown as mean±SD) are corrected for gender, intracranial volume (ICV) and age. ****p<0.0001; ***p<0.001, Kruskal-Wallis followed by unpaired Student’s t-test. ALS, amyotrophic lateral sclerosis; fALS, familial ALS.
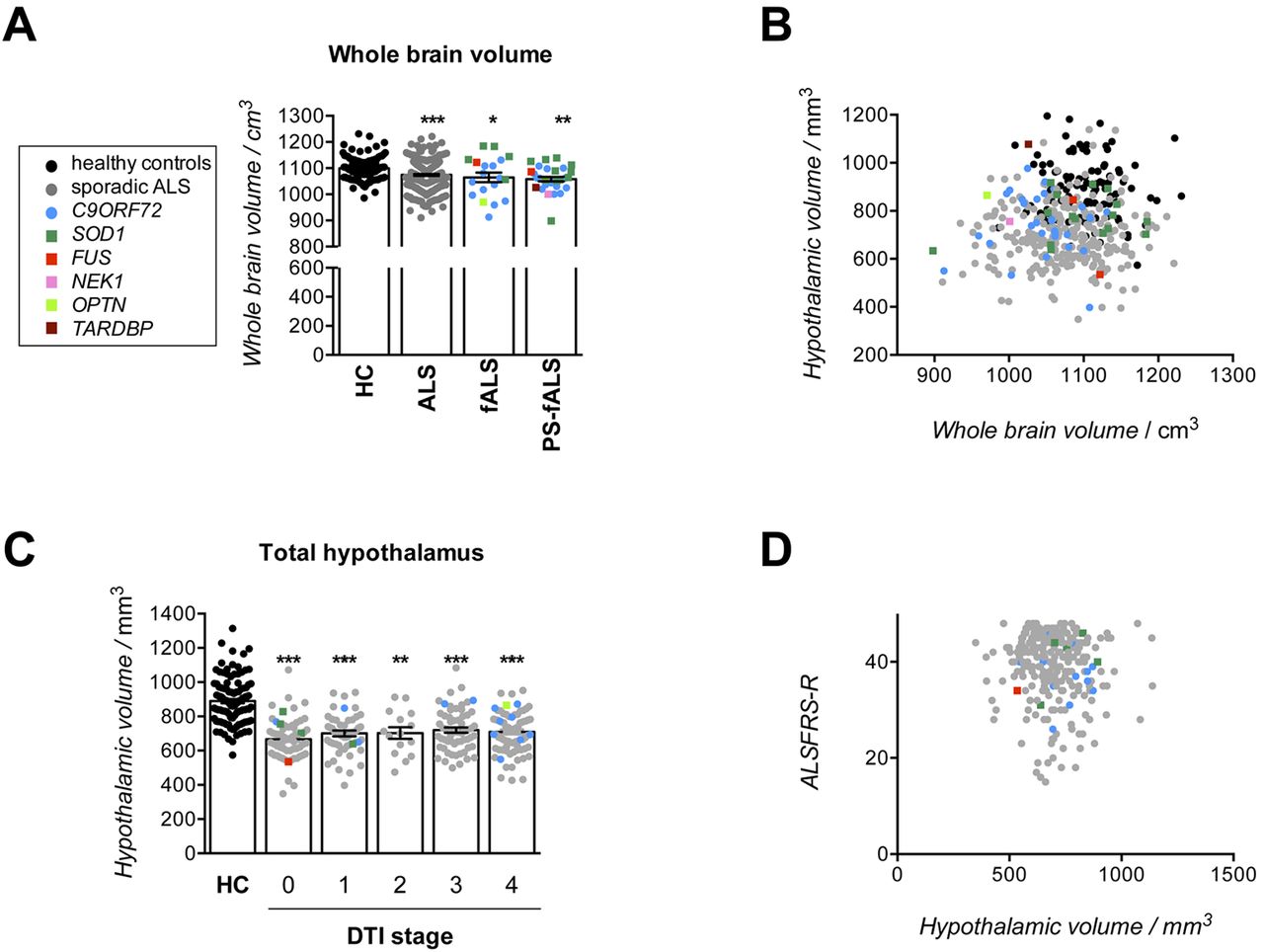
To determine whether the observed atrophy was related to global brain atrophy, we measured whole brain volume (WBV) on the same MRI scans. WBVs were slightly consistently decreased in patients with sporadic ALS (−2.3%, p<0.0001)37 and also in symptomatic ALS mutation carriers (−3.1%, p=0.0391) and presymptomatic mutation carriers (−3.7%, p<0.0001) as compared with HC (figure 3A). However, the hypothalamic volume was not correlated with WBV in either populations (figure 3B)(p>0.05). There was no relationships between DTI stages and hypothalamic volume (figure 3C), nor between ALSFRS-R and hypothalamic volume (figure 3D) (p>0.05). Thus, hypothalamic atrophy was not related with brain atrophy or clinical disease progression.

Hypothalamic atrophy is not related to disease progression in ALS, (A) whole brain volume relative in healthy controls (HC black dots, n=112), sporadic ALS cases (grey dots ALS, n=251), symptomatic (fALS, n=19) and presymptomatic ALS mutation carriers (PS-fALS, n=32). The different gene mutations are colour coded in all panels according to the legend in panel A. (B) Spearman rank order correlation of hypothalamic volume with whole brain volume, p>0.05. (C) Hypothalamic volume in HC and patients with ALS stratified by DTI stages. (D) Spearman rank order correlation of hypothalamic volume with ALSFRS-R in patients with ALS (grey and coloured dots), p>0.05. All volumes (shown as mean ± SD) are corrected for gender, intracranial volume (ICV) and age.****p<0.0001; ***p<0.001; *p<0.05. ALS, amyotrophic lateral sclerosis; ALSFRS-R, revised ALS Functional Rating Scale; DTI, diffusion tensor imaging; fALS, familial ALS.
Hypothalamic volume correlated smally but significantly with BMI at time of MRI in patients with ALS (p=0.0434, ρ=+0.1579, figure 4A), and this correlation was much more robust in patients with symptomatic fALS (p=0.0060, ρ=+0.6053, figure 4A). This robust correlation between BMI and hypothalamic volume in patients with fALS was also present when considering anterior or posterior hypothalamic volumes separately (p=0.027, ρ=+0.5064 and p=0.034, ρ=+0.4895, respectively figure 4B,C).

Hypothalamic atrophy is related to body mass index (BMI) in ALS (A–C), Spearman rank order correlation of total (A), anterior (B) and posterior hypothalamic volume with BMI. Sporadic ALS cases (grey dots ALS, n=251) and symptomatic (fALS, n=19) are shown in the left panel. For clarity, patients with fALS are shown in the right panel. The different gene mutations are colour coded in all panels according to the legend in panel A. ALS, amyotrophic lateral sclerosis; fALS, familial ALS.
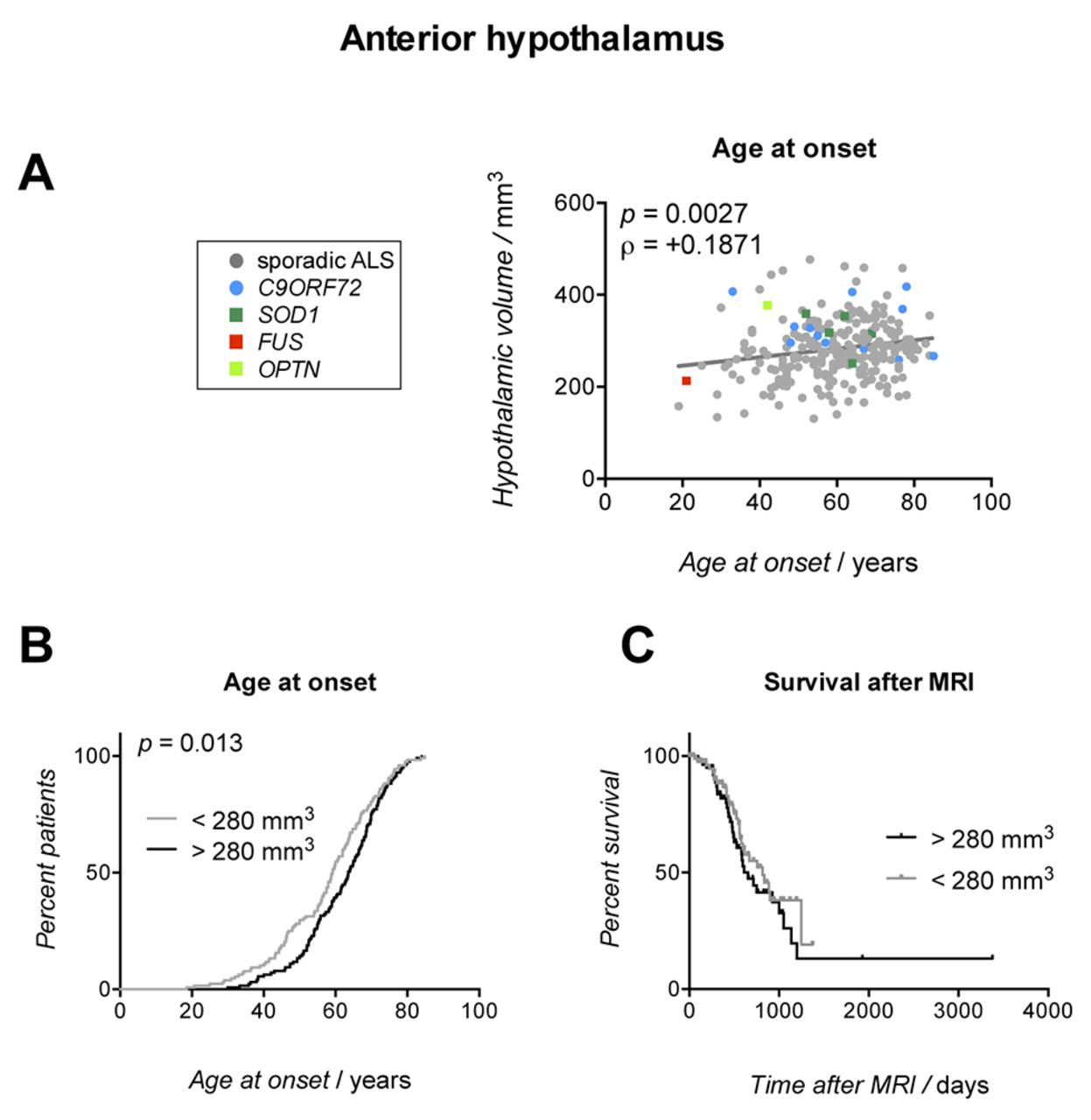
Since hypothalamus was already atrophied in presymptomatic ALS mutation carriers, we studied potential relationships between hypothalamic volumes and age at onset. Interestingly, age at onset was correlated with anterior hypothalamic volume (figure 5A), but not with total or posterior hypothalamic volumes (not shown). Consistently, patients with ALS with anterior hypothalamic volume higher than the median value of this population (ie, 280 mm3) developed ALS symptoms later than patients below the median value (p=0.013, Gehan-Breslow Wilcoxon test, figure 5B) with a relative risk of 1.23 (95% CI: 0.97 to 1.58). Median age at onset was significantly higher in patients with high anterior hypothalamic volume (63.6 years) than in patients with low anterior hypothalamic volume (59.2 years), thus providing a more than 4 years advantage of disease-free condition for these individuals. Contrastingly, anterior hypothalamic volume was not related with survival after MRI (figure 5C). Thus, anterior hypothalamic volume of patients with ALS was related to age at onset.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Atrophy of the anterior hypothalamus is related to age at onset in ALS, (A) Spearman rank order correlations of anterior hypothalamic volume with age at onset (B, C), Kaplan-Meyer curves of age at onset (B) or survival after MRI (C) of patients with ALS stratified according to their anterior hypothalamic volume. The black line represents patients with ALS having high anterior hypothalamic volume (above the median value of 280 mm3). The grey line represents patients with ALS having low anterior hypothalamic volume (below the median value of 280 mm3). In panel (C), censored patients are indicated by dots symbols on the corresponding survival curve. ALS, amyotrophic lateral sclerosis.
Discussion
In this study, we provide evidence that the total volume of the hypothalamus in patients with ALS is substantially reduced compared with controls. The volume loss occurs before motor symptoms as we observed hypothalamic atrophy in presymptomatic ALS mutation carriers. Interestingly, the atrophy of the hypothalamus appears to be related with BMI, especially in patients with fALS, and the atrophy of the anterior hypothalamus correlates with age at onset. These findings might have consequences for our understanding of energy metabolism defects in ALS.
Previous studies of hypothalamic volumetry included an order of magnitude less cases and were mostly performed in bvFTD20–23 and Huntington’s disease.26 Another original addition of the current study is the inclusion of a large group of presymptomatic ALS mutation carriers, allowing to discern whether the observed atrophy is premorbid. We specifically optimised the delineation technique previously validated by Gabery and collaborators26 to exclude white matter structures such as the internal capsule and cerebral peduncle together with laterally adjacent non-hypothalamic grey matter from the manually delineated hypothalamus. In particular, our method is very conservative in the determination of hypothalamic volume, as it excludes mammillary bodies and optical tracts, that is, regions that are sometimes included in other studies.20 21 23 This likely underlies the difference between the hypothalamic volumes in controls in our study (mean value: 889 mm3) as compared with the study by Bocchetta and collaborators who included the mammillary bodies (mean value: 944 mm3). Despite these technical differences, it is important to note that the different studies mostly converge for their conclusions. For instance, our study identified a hypothalamic volume loss of 16% in symptomatic ALS mutations carriers, mostly C9ORF72 expansion mutation carriers, and this in the same range as the hypothalamic atrophy observed in patients with bvFTD carrying a C9ORF72 expansion.23 We chose not to further subdivide the hypothalamus into subregions, mostly because the boundaries between the different nuclei are difficult to define in both MRI data (figure 1) and histological sections.30
It is the first major result of our study that hypothalamic volume was severely reduced in ALS. The atrophy of the hypothalamus was not associated with the atrophy of the whole brain suggestive of a region-selective process of degeneration in ALS. Indeed, the existence of hypothalamic atrophy even in presymptomatic ALS mutation carriers suggests that the hypothalamic atrophy pre-exists to motor symptoms. It is unclear how this hypothalamic atrophy relates to the spreading of the disease as it is present in presymptomatic ALS mutation carriers. In the neuropathological studies of Braak and collaborators, the hypothalamus was not systematically studied and it is thus difficult to relate our observation to the current knowledge on the spreading of pTDP43 proteinopathy.38 39 Recently, pTDP43 pathology was observed in the hypothalamus of a subset of patients with ALS that also had basal forebrain pathology and could therefore be classified as patients with stage 3/4 ALS according to Braak staging of ALS.18 More detailed pathological analysis of the hypothalamus in patients with ALS should be conducted and compared with Braak staging.
The observed hypothalamic atrophy in patients with ALS was quantitatively more important than in HD,26 and similar to what was previously observed in patients with bvFTD20–23 in particular in C9ORF72 mutation carriers.20–23 It is important to note, however, that the different methodologies of delineation used across studies render their comparison difficult, and measurements of hypothalamic volumes cross-validated between laboratories are critically needed. We used a similar strategy as Piguet and collaborators to identify the posterior and anterior hypothalamus,21 as these authors identified a preferential atrophy of the posterior hypothalamus in bvFTD. In this study, we observed similar atrophy of both regions in patients with ALS. While we cannot completely exclude that this difference lies into methodological differences between both studies, the hypothalamic volumes of patients with ALS were clearly consistent with a narrowing of the more lateral parts of the hypothalamus, rather than a preferential atrophy of the posterior part. This is consistent with the recent observation of pTDP43 pathology in the lateral hypothalamus of patients with ALS.18
The observation of hypothalamic atrophy as another commonality between ALS and FTD would be consistent with a major role of the hypothalamus in eating abnormalities that are pronounced in patients with bvFTD and correlated with hypothalamic volume,20–23 and milder in patients with ALS, as detected in a series of recent studies14 15 as well as in animal models.11 16 Hypothalamic atrophy could be also a common substrate in the increased energy expenditures in both patients with ALS9 and bvFTD.22 Consistent with this idea, the volume of the hypothalamus was positively correlated with BMI, and this correlation was much stronger in patients with fALS. This finding indirectly suggests that the volume of the hypothalamus could be a surrogate of body weight, in a more pronounced manner in familial cases. Interestingly, we and others have shown that weight loss is a predictor of survival in patients with ALS and models.7 8 11 Indeed, weight loss is a very early process in patients with ALS and is even premorbid,3 4 and this coincides with the hypothalamic atrophy in presymptomatic mutation carriers. The weak correlation between hypothalamic volume and BMI in patients with sporadic ALS could be the consequence of heterogeneous dietary management of patients with ALS, such as occurence of dysphagia or usage of percutaneous endoscopic gastrostomy, that constitute potential modifiers of weight loss during disease progression. Our observation of earlier onset in patients with a low anterior hypothalamic volume further indicates that the hypothalamus could be involved in weight loss and onset of disease. It is important however to stress that this association, even if significant, remains small, and thus its clinical relevance is uncertain. Furthermore, it is important to mention that eating behaviour and weight control are not merely a hypothalamic phenomenon. Indeed, alterations in orbitofrontal and other impulse control circuits are contributing to these abnormalities.40 Moreover, atrophy of other subcortical structures has been observed in ALS,41 42 and it is possible that hypothalamic atrophy is a downstream result from atrophy of other interconnected subcortical structures, such as nucleus accumbens, thalamus or caudate.41 42 Further studies are needed to characterise the cause-to-effect relationships between weight loss and atrophy of subcortical regions including hypothalamus.
Summarising, we provide here evidence that the hypothalamus of patients with ALS is atrophied, even in presymptomatic ALS mutation carriers, and that this atrophy relates to the age at onset. The large cohort with 270 patients with ALS included in the analysis as well as their in vivo DTI-based staging characterisation reinforce our conclusions. Further prospective studies should be initiated, combining dietary evaluation, longitudinal follow-up of metabolism, and MRI and CSF puncture to strengthen these results. Since counteracting weight loss could be a valuable strategy to improve the survival of patients with ALS,12 13 our study suggests that the identification of the precise hypothalamic alterations could help in designing targeted strategies to combat weight loss in these patients. Our study also calls for further investigation of hypothalamic volumes in other neurodegenerative diseases such as Alzheimer’s disease and Parkinson’s disease which are also associated with defective energy homeostasis.
Acknowledgments
We thank Sanaz Gabery, Raphael Peter and Kornelia Günther for their help in data collection.
References
Footnotes
MG and PV contributed equally.
JK and LD share senior authorship.
Contributors MG collected MRI scans, performed manual delineation of hypothalami, performed data analysis after delineation and collected clinical data; PV performed manual delineation of hypothalami and performed data analysis after delineation; H-PM provided expertise in data analysis; H-JH measured whole brain and intracranial volumes; PW organised the study of presymptomatic mutation carriers; AR and GN provided clinical expertise and patient information, AP provided expertise on manual delineation of hypothalamus; ACL, JK and LD conceived and designed the study. PV, MG, JK and LD performed statistical analysis, prepared the figures and drafted the manuscript. All authors critically reviewed the manuscript for intellectual content. MG and PV shared first authorship. JK and LD are joint senior authors of this study.
Funding This work was supported by fondation « recherche sur le cerveau » (call 2015, to LD), Fondation Thierry Latran (SpastALS, to LD) and ARSla (call 2016, to LD). Work in our laboratories is supported by Agence Nationale de la Recherche (grants ToFU and EpiFUS; to LD); ALS Association Investigator Initiated Award (grants 2235, 3209 and 8075; to LD); the Frick Foundation (award 2013 to LD); Association Française contre les Myopathies (grant #18280; to LD); Virtual Helmholtz Institute ‘RNA dysmetabolism in ALS and FTD’ (WP2, to LD and ACL); by the German Research Foundation (Deutsche Forschungsgemeinschaft, DFG Grant Number LU 336/15-1 to ACL) and the German Network for Motor Neuron Diseases (BMBF 01GM1103A to ACL); the Swedish Research Council (ÅP).
Competing interests None declared.
Patient consent Obtained.
Ethics approval Ethics Committee of the University of Ulm.
Provenance and peer review Not commissioned; externally peer reviewed.