Article Text

Abstract
Objectives In neuromyelitis optica spectrum disorders (NMOSD) thalamic damage is controversial, but thalamic nuclei were never studied separately. We aimed at assessing volume loss of thalamic nuclei in NMOSD. We hypothesised that only specific nuclei are damaged, by attacks affecting structures from which they receive afferences: the lateral geniculate nucleus (LGN), due to optic neuritis (ON) and the ventral posterior nucleus (VPN), due to myelitis.
Methods Thirty-nine patients with aquaporin 4-IgG seropositive NMOSD (age: 50.1±14.1 years, 36 women, 25 with prior ON, 36 with prior myelitis) and 37 healthy controls (age: 47.8 ± 12.5 years, 32 women) were included in this cross-sectional study. Thalamic nuclei were assessed in magnetic resonance images, using a multi-atlas-based approach of automated segmentation. Retinal optical coherence tomography was also performed.
Results Patients with ON showed smaller LGN volumes (181.6±44.2 mm3) compared with controls (198.3±49.4 mm3; B=−16.97, p=0.004) and to patients without ON (206.1±50 mm3 ; B=−23.74, p=0.001). LGN volume was associated with number of ON episodes (Rho=−0.536, p<0.001), peripapillary retinal nerve fibre layer thickness (B=0.70, p<0.001) and visual function (B=−0.01, p=0.002). Although VPN was not smaller in patients with myelitis (674.3±67.5 mm3) than controls (679.7±68.33; B=−7.36, p=0.594), we found reduced volumes in five patients with combined myelitis and brainstem attacks (B=−76.18, p=0.017). Volumes of entire thalamus and other nuclei were not smaller in patients than controls.
Conclusion These findings suggest attack-related anterograde degeneration rather than diffuse thalamic damage in NMOSD. They also support a potential role of LGN volume as an imaging marker of structural brain damage in these patients.
- thalamus
- neurodegeneration
- optic neuritis
- lateral geniculate nucleus
- transsynaptic degeneration
Statistics from Altmetric.com
Introduction
Neuromyelitis optica spectrum disorders (NMOSD) are chronic, relapsing inflammatory disorders of the central nervous system, defined by pathogenic IgG antibodies against astrocytic aquaporin-4 (AQP4-IgG) in the majority of cases.1 The most typical clinical manifestations are optic neuritis (ON) and acute myelitis, usually occurring as longitudinally extensive transverse myelitis.1 2 Other clinical core characteristics include area postrema and acute brainstem syndromes.1
Patients with NMOSD very rarely show a secondary progressive phase,3 and the mechanisms leading to neurological disability are thought to be mainly attack-related.3–5 However, recent findings suggested retinal neuronal loss independent of ON attacks in NMOSD.6 Moreover, some imaging7 8 and histopathological studies in NMOSD9 10 showed abnormalities and neuronal loss in non-lesional cortical grey matter. Less is known regarding deep grey matter changes in NMOSD, particularly the affection of the thalamus is controversial.11–16
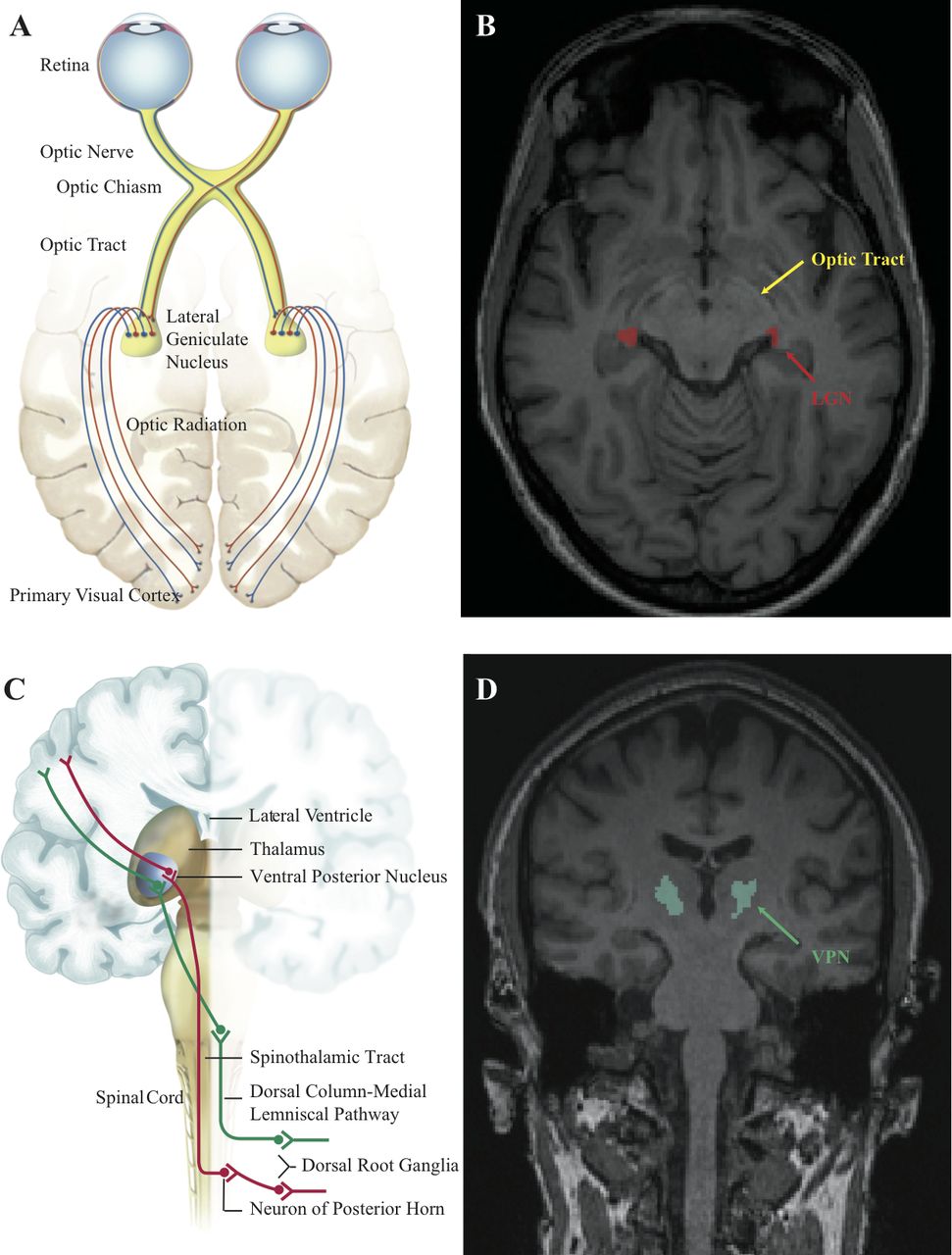
Our aim was to assess volume loss in thalamic nuclei in NMOSD. Our hypothesis was that lesions in (1) the optic nerves due to ON and (2) the spinal cord due to myelitis may cause anterograde degeneration only to specific nuclei, with which these structures are connected. We hypothesised that the lateral geniculate nucleus (LGN), which receives afferences from the optic nerves, is affected due to ON and the ventral posterior nucleus (VPN), which receives afferences from the dorsal column-medial lemniscal pathway and the spinothalamic tract, due to myelitis (figure 1). Thus, we assessed LGN and VPN volumes in NMOSD, and studied whether they are associated to clinical attacks (ON, myelitis), attack-related structural damage (in retina and spinal cord) and clinical deficits (visual and sensory dysfunction). Our secondary, exploratory objective was to investigate whether there is occult volume loss in other thalamic nuclei in NMOSD.

Lateral geniculate and ventral posterior nuclei and their afferences in the visual and sensory pathways. (A) The afferent visual pathway; note the lateral geniculate nucleus (LGN), which receives afferences from both optic nerves. We hypothesised LGN volume loss in neuromyelitis optica spectrum disorders (NMOSD), due to optic neuritis. (B) Axial T1-weighted three-dimensional magnetisation prepared rapid acquisition gradient echo (MPRAGE) image showing an actual example of LGN segmentation (red) using the Multiple Automatically Generated Templates (MAGeT) brain algorithm in a control. Note also the optic tract in yellow. (C) The thalamic ventral posterior nucleus (VPN) receives afferences from the spinothalamic pathway (in red) and dorsal column/medial lemniscal pathway (in green). We hypothesised VPN volume loss in NMOSD, due to myelitis involving these pathways. (D): Coronal T1-weighted three-dimensional MPRAGE image showing an actual example of VPN segmentation (turquoise) using the MAGeT brain algorithm in a control. The schematic figure of the afferent visual system (A) is adapted from the website of the Neurodiagnostics laboratory @ Charité – Universitätsmedizin Berlin, Germany (http://neurodial.de/2017/08/25/schematic-figure-the-afferent-visual-system-creative-commons-license).
Methods
Study participants
We screened 78 patients with NMOSD from a prospective observational cohort study at the NeuroCure Clinical Research Center at the Charité-Universitätsmedizin Berlin (recruited from May 2013 to January 2018). The inclusion criteria were: (1) age ≥18 years and (2) AQP4-IgG seropositive NMOSD, according to the 2015 International Consensus Diagnostic Criteria.1 AQP4-IgG were determined by a cell-based assay (Euroimmun, Lübeck, Germany). Patients that were AQP4-IgG seronegative (n=25), had incomplete clinical data and/or unknown AQP4-IgG-status (n=10), no MRI data (n=3) or an attack within 3 months prior to baseline (n=1) were excluded.
We included 39 AQP4-IgG seropositive NMOSD patients. Data from 37 healthy controls with age ≥18 years, without history of neurological or opthalmological diseases were also included. Healthy controls were chosen from the institute’s research database, to be as well matched as possible regarding age and sex to the patients. The characteristics of the study participants are presented in table 1.
Characteristics of the NMOSD patients and controls included in the study
This study was approved by the local ethics committee (Ethikkommission der Charité—Universitätsmedizin Berlin; EA1/131/09) and conducted in accordance with the Declaration of Helsinki in its currently applicable version. All participants gave written informed consent before inclusion in the study.
Clinical assessment
Comprehensive neurological examinations were performed by raters, under supervision of board-certified neurologists, to assess the Expanded Disability Status Scale, including the functional system scores (FSS) according to the neurostatus definitions. Attack history was also recorded, using clinical criteria.
Visual acuity was tested monocularly under photopic conditions using retro illuminated Early Treatment in Diabetes Retinopathy Study charts at a 4 m distance. The logarithm of the minimum angle of resolution (logMAR) was used as a measure of visual function. We included the visual function measurement only from patients where best correction was used (n=30).
Magnetic resonance imaging
MRI was performed for all participants at 3T (MAGNETOM Trio Siemens, Erlangen, Germany) on the same day as the clinical examination, except for two participants, where there was an interval of 1 day. Details regarding the MRI protocol and the assessment of thalamic and optic radiation (OR) lesions are given as online supplementary material.
Supplemental material
Measurement of thalamic volume and thalamic nuclei volume
The volumes of the entire thalamus and the thalamic nuclei were measured using the Multiple Automatically Generated Templates (MAGeT) brain algorithm17 on three-dimensional T1-weighted magnetisation prepared rapid acquisition gradient echo (MPRAGE) images. MAGeT uses an atlas derived from manually segmented serial histological data, including delineation of the thalamic nuclei. It first customises the atlas to a subset of participants, representative of the study population, using nonlinear registration and uses this newly segmented subset as a template library for the remaining participants. This has the advantage of correcting for the neuroanatomical variability of the study population. Details regarding the representative subset of the present study are given as online supplementary material.
The segmentation results were visually inspected by one experienced rater (LG), who was blinded to the clinical data and no subjects had to be excluded. Last, all volumes were extracted and normalised using the SIENAX V-scaling factor for head-size.18
Figure 1 and online supplementary figures 1 and 2 show examples of the LGN and VPN as segmented by MAGeT.
Mean upper cervical cord area
The mean upper cervical cord area (MUCCA) was used as a sensitive measure to assess spinal cord atrophy in patients with NMOSD.19 Methodological details are given as online supplementary material.
Optical coherence tomography
Retinal imaging was performed using a Heidelberg Engineering Spectralis spectral domain optical coherence tomography (OCT; Heidelberg Engineering, Heidelberg, Germany). We report the OCT acquisition settings, scanning protocol and details regarding excluded scans as online supplementary material.
The mean peripapillary retinal nerve fibre layer (pRNFL) thickness and the combined ganglion cell and inner plexiform layer (GCIPL) volume were used in the analysis.
Statistical analysis
Differences in age and sex-distribution between patients and controls were investigated using t-test and Fisher’s exact test, respectively.
The associations of thalamic, LGN and VPN volumes with demographic characteristics were studied in controls using linear mixed effect models (LMM), with age, sex, handedness and brain side as fixed effects. If not stated otherwise, group comparisons, as well as structural–structural and structural–functional associations of thalamic nuclei were also performed using LMM, to account for intra-subject inter-side dependencies. Age and sex were always included as fixed effects in these models. The association of LGN volume with visual function was studied in LMM with monocular logMAR as dependent variable and LGN volume sum of both hemispheres as fixed effect, since both LGN receive afferences from each eye. Relevant results were checked in additional LMM, adjusting for OR lesions and retinal damage (mean pRNFL thickness). We also performed analyses stratified for: (1) ON (for LGN), (2) myelitis (for VPN) and (3) brainstem attacks (for VPN). We report effect sizes from the LMM as marginal R2 (mR2), representing the variance explained by the fixed effects alone, and conditional R2 (cR2), representing the variance explained by both fixed and random effects.
Associations between LGN and VPN volumes with number of attacks and FSS were studied through Spearman correlation tests, due to the non-normal distribution of these variables (analysis per patient, using the volume sum of both hemispheres). Bilateral ON was counted as two episodes.
Last, we performed an exploratory analysis comparing all other thalamic nuclei between patients and controls, using LMM. This analysis was corrected for multiple comparisons using the Holm-Bonferroni method.
For all models, statistical significance was achieved at p<0.05. All statistical analysis was performed using R,20 V.3.4.3 with packages: pastecs, lme4, lmerTest, MuMIn and ggplot2.
Data availability statement
All anonymised data not published within this article can be shared on reasonable request from any qualified investigator.
Results
Demographics, clinical and imaging characteristics of the study population
Patients with NMOSD and controls showed no difference regarding mean age (p=0.447), sex (p=0.475) or handedness (p=0.494; table 1).
Twenty-five patients (64.1%) had a history of at least one ON attack (NMO-ON) and the rest never had an ON (NMO-NON). Most patients (92.3%) had at least one myelitis, while there were also five patients with a brainstem attack (table 1).
A total of 17/39 (43.6%) patients had OR lesions, typically small, with non-specific morphology (median lesion number: 0, range: 0–18). There was a single patient with a left thalamic lesion. Since the left LGN and VPN volumes of this patient were not outliers (147.7 mm3 and 612.2 mm3, respectively) we did not exclude this patient from the analysis.
Volume of the entire thalamus
In controls, thalamic volume was associated with age (B=−17.50, SE=8.45, p=0.047) and brain side, with the thalamus being larger on the right (7760.5±602.3 mm3) compared with left (7185.7±560.2 mm3; B=573.54, SE=34.26, p<0.001).
Total thalamic volume did not differ between NMOSD patients (7382.6±668.7 mm3) and controls (7473.1±646.1 mm3), when accounting for age and brain side (B=−68.49, SE=119.62, p=0.569).
Volume of the LGN
In controls, LGN volume was also associated with brain side, with the LGN being larger on the right (240.3±29.9 mm3) compared with left (156.3±20.6 mm3; B=83.42, SE=3.53, p<0.001), but not with age, sex or handedness. Mean LGN volume did not differ between NMOSD patients and controls (table 2).
Volumes of the LGN and VPN in NMOSD patients and controls
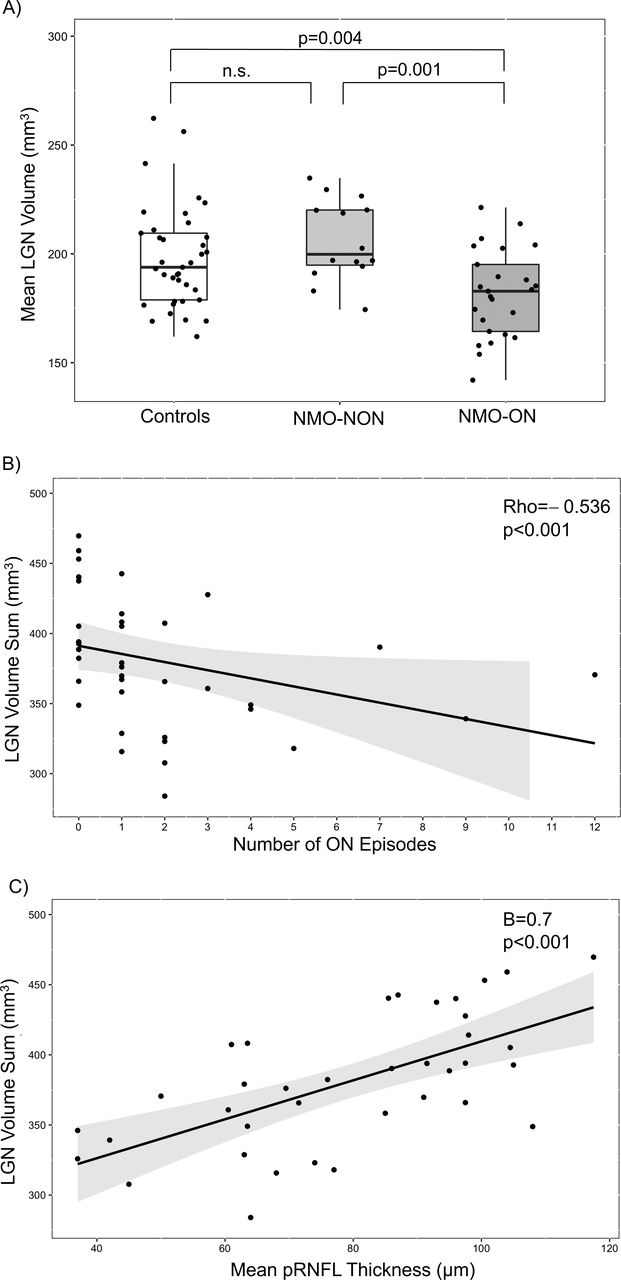
LGN volume was lower in NMO-ON patients compared with NMO-NON patients (B=−23.74, SE=6.76, p=0.001, mR2=0.05, cR2=0.94; figure 2) and in NMO-ON patients versus controls (table 2, figure 2). These results remained after exclusion of seven patients on daily prednisolone (data not shown). In contrast, there was no difference between NMO-NON patients and controls (table 2, figure 2).
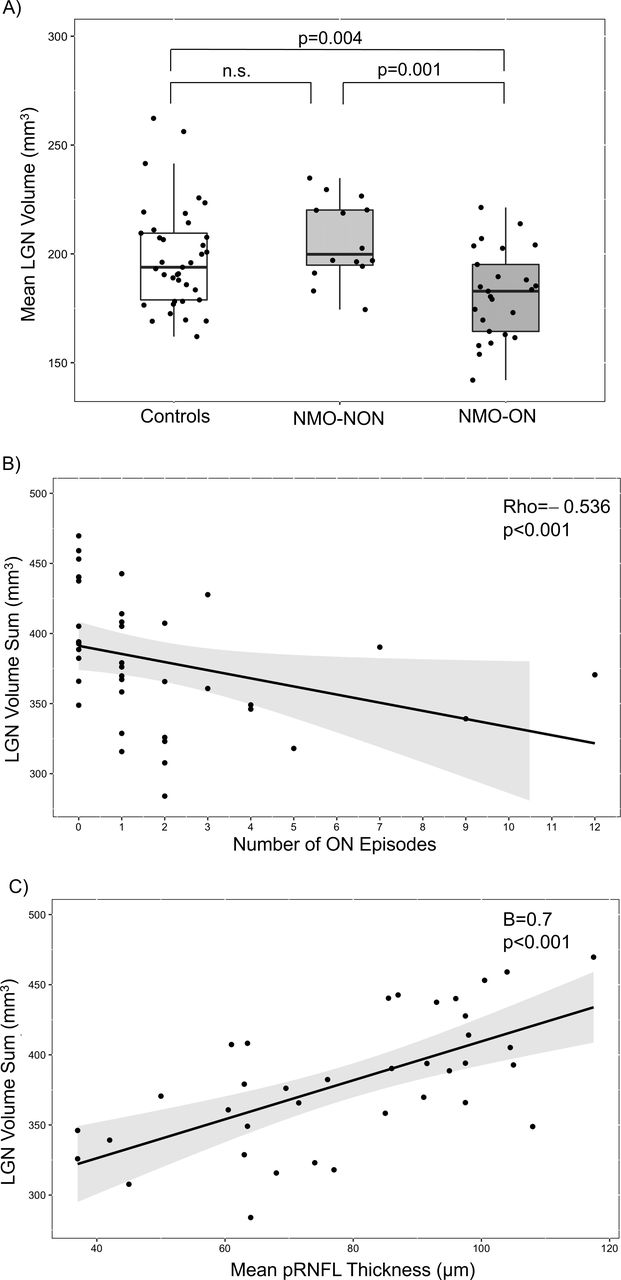
Volume of the lateral geniculate nucleus (LGN) in NMOSD and its relationship with optic neuritis (ON) and retinal axonal damage. (A) Normalised LGN volume per participant (mean of both hemispheres) in the three groups: controls, patients with NMOSD and negative ON history (NMO-NON) and patients with NMOSD and positive ON history (NMO-ON). (B–C): Relationship between normalised LGN volume in NMOSD patients (sum of both hemispheres per patient) and: (B) number of ON episodes,(C) mean peripapillary retinal nerve fibre (pRNFL) thickness of both eyes. NMOSD, neuromyelitis optica spectrum disorders.
For a separate analysis of the ipsi- and contralateral LGN volumes and their association to ON, see online supplementary material.
Volume of the LGN, ON and OCT parameters
In line with the smaller LGN found in NMO-ON, LGN volume inversely correlated with number of ON episodes in patients (Rho=−0.536, p<0.001; figure 2). When assuming a linear relationship, each ON episode led to, on average, an LGN volume loss of −3.09 mm3 (SE=1.16, p=0.012). We did not find an association between LGN volume and time since first (B=−0.16, SE=0.67, p=0.809) or last ON episode (B=1.28, SE=1.29, p=0.333).
In patients, LGN volume was associated with mean pRNFL thickness (B=0.70, SE=0.14, p<0.001, mR2=0.07, cR2=0.94) and mean GCIPL volume of both eyes (B=51.82, SE=11, p<0.001, mR2=0.06, cR2=0.94) (figure 2). The results were similar in models adjusted for OR lesions (pRNFL: B=0.71, SE=0.15, p<0.001; GCIPL: B=51.86, SE=11.10, p<0.001). In controls, there were no associations of pRNFL and GCIPL with LGN volume (data not shown).
When looking at NMO-NON and NMO-ON patients separately, the associations of LGN volume with pRNFL thickness and GCIPL volume remained only in the NMO-ON subgroup (pRNFL: B=0.64, SE=0.21, p=0.007, mR2=0.05, cR2=0.93; GCIPL: B=40.18, SE=16.18, p=0.023, mR2=0.04, cR2=0.93), but not in NMO-NON patients (pRNFL: B=0.19, SE=0.55, p=0.741; GCIPL: B=40.51, SE=39.09, p=0.322).
Volume of the LGN and lesions in the OR
Presence of OR lesions was not associated with ipsilateral LGN volume (B=−0.52, SE=6.35, p=0.935) and OR lesion number did not correlate with LGN volume (Rho=0.026, p=0.877). Moreover, LGN volume remained smaller in NMO-ON than in NMO-NON, when accounting for OR lesions (B=−23.74, SE=6.82, p=0.001, mR2=0.04, cR2=0.94).
Volume of the LGN and visual function
LGN volume (sum of both hemispheres) was associated with visual function measured as logMAR (B=−0.01, SE=0.002, p=0.002, mR2=0.22, cR2=0.27). This effect did not remain significant after inclusion of pRNFL thickness in the model (LGN: B=0.001, SE=0.002, p=0.613; pRNFL: B=−0.02, SE=0.003, p<0.001, mR2=0.52, cR2=0.52).
Volume of the VPN
In controls, VPN volume was associated with brain side, with the VPN being larger on the left (706.7±65.8 mm3) compared with right (652.8±60.4 mm3; B=−54.44, SE=6.54, p<0.001), but not with age, sex or handedness.
Mean VPN volume was not different between NMOSD patients and controls (B=−4.58, SE=13.4, p=0.730; table 2 and figure 3).
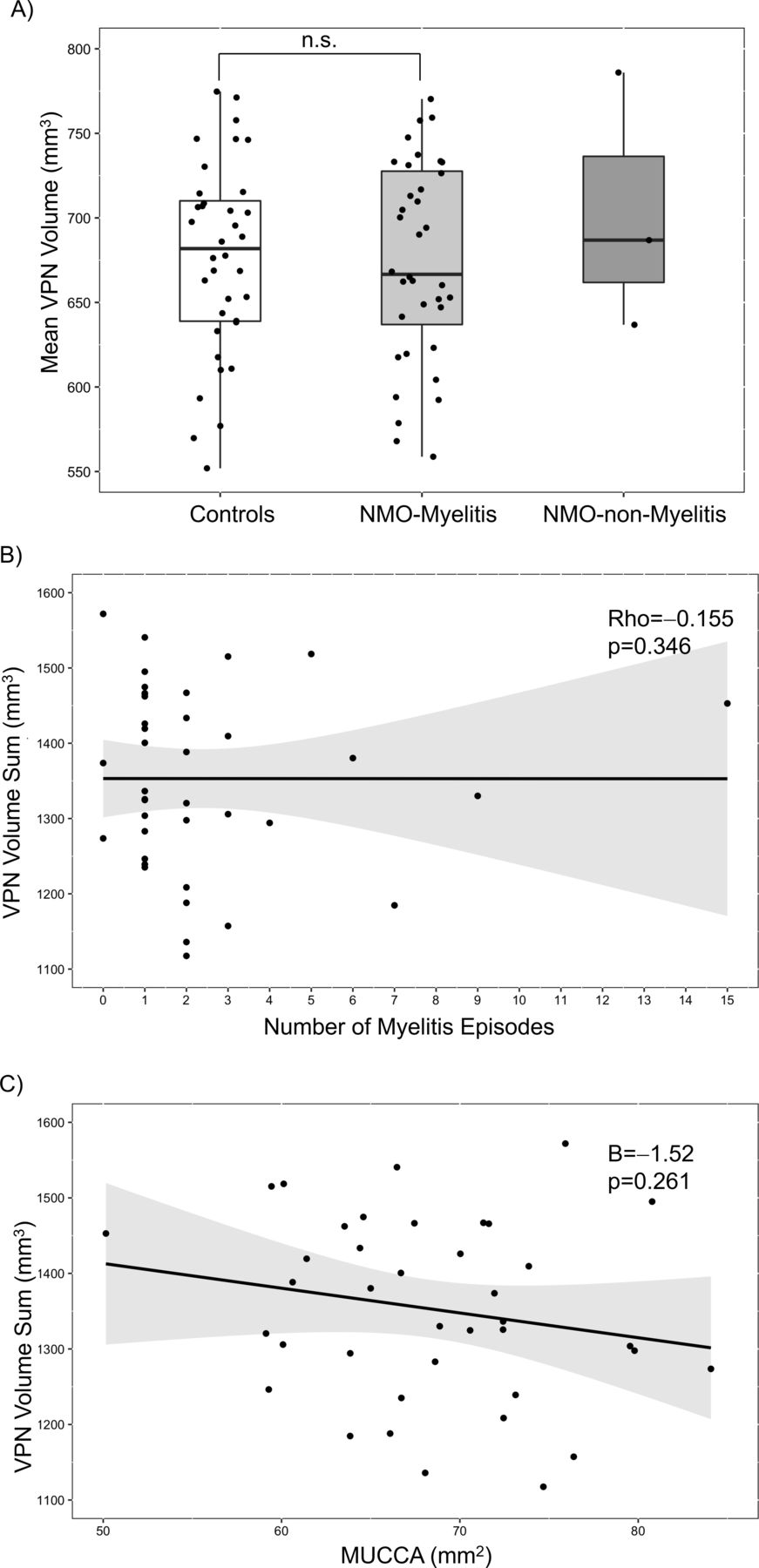
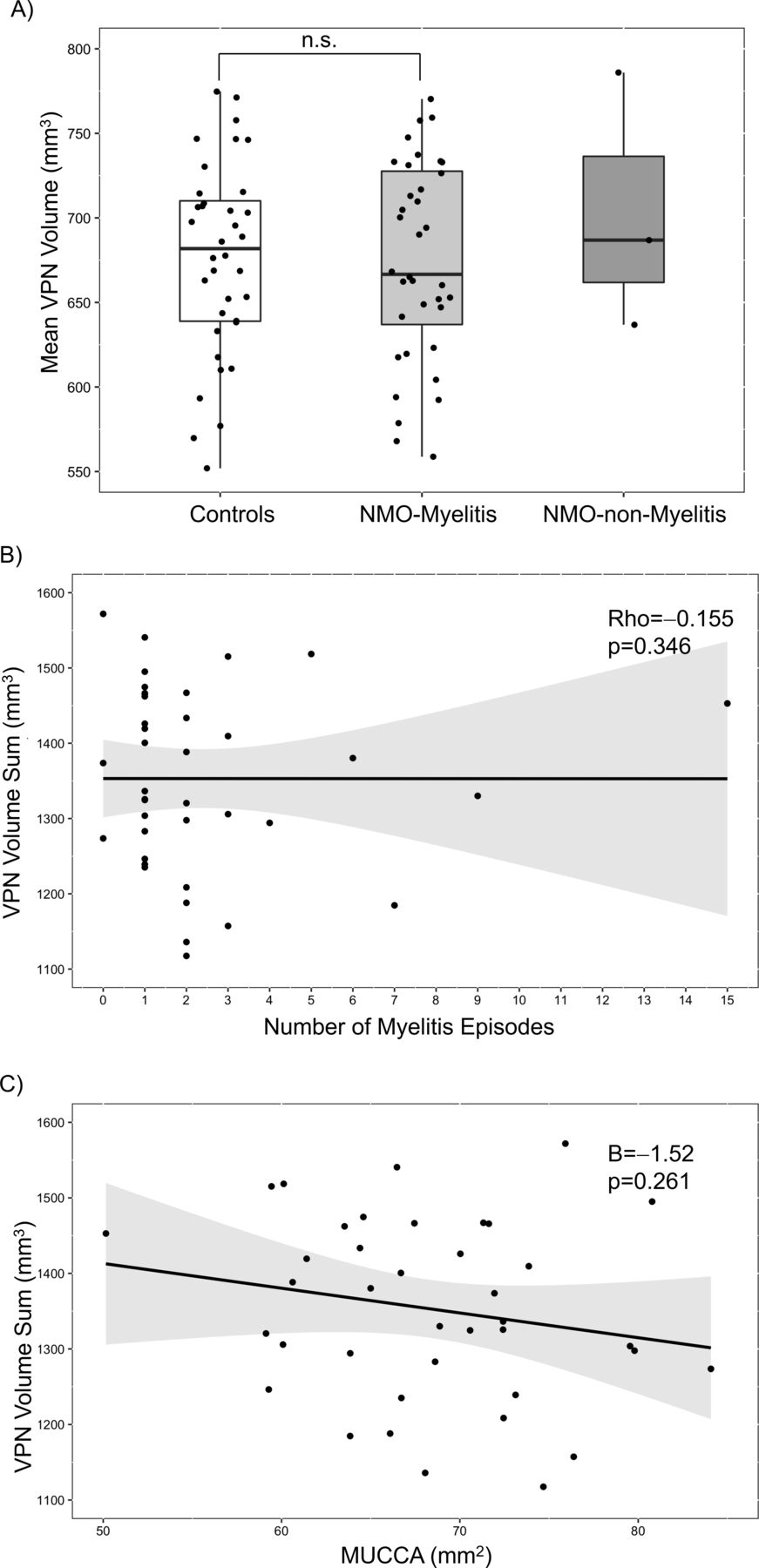
Volume of the ventral posterior nucleus (VPN) in NMOSD and its relationship with myelitis and spinal cord damage. (A) Normalised VPN volume per participant (mean of both hemispheres) in the three groups: controls, patients with NMOSD and myelitis (NMO-Myelitis) and patients with NMOSD without myelitis (NMO-non-Myelitis). No comparison was made between patients with- and without myelitis, due to the low number of the latter (n=3). (B–C): Relationship between normalised VPN volume in NMOSD patients (sum of both hemispheres per patient) and: (B) number of myelitis episodes, (C) mean upper cervical cord area (MUCCA). NMOSD, neuromyelitis optica spectrum disorders.
Volume of the VPN and myelitis
There was no difference in VPN volume between patients with myelitis and controls (table 2, figure 3). This remained after exclusion of seven patients on daily prednisolone (data not shown). Moreover, we found no association between VPN volume and number of myelitis episodes (Rho=−0.155, p=0.346; figure 3), time since first- (B=−1.09, SE=1.48, p=0.466), or last myelitis (B=−4.32, SE=2.78, p=0.131).
To study associations between VPN and myelitis-related spinal cord damage, we used the MUCCA (mean in patients: 68.3±7.0 mm2 vs 74.8±6.4 mm2 in controls). MUCCA was neither associated with VPN volume in NMOSD patients (B=−1.52, SE=1.33, p=0.261; figure 3) nor in the subgroup of patients with myelitis (B=−2.45, SE=1.37, p=0.084). Similar results were seen in controls (data not shown).
Moreover, there was no correlation between VPN volume and sensory FSS (Rho=−0.282, p=0.091).
Volume of the VPN and brainstem attacks
Due to the unexpected lack of association between VPN and myelitis, and since the VPN segmented in the present study included the ventral posterolateral nucleus, which receives afferences from the brainstem (trigeminothalamic tract), we performed a subgroup analysis in patients that had both myelitis and brainstem attacks (n=5; see table 3).
Patients with myelitis and brainstem attacks
Indeed, we found lower VPN volumes in these patients (613.6±71.8 mm3) versus controls (679.7±68.33; B=−76.18, SE=30.52, p=0.017, mR2=0.12, cR2=0.85; figure 4). Since two of these patients were on daily prednisolone, we also performed this analysis including prednisolone treatment as random effect and the result remained (B=−70.84, SE=31.83, p=0.048). There was also a correlation between VPN volume and number of brainstem attacks (Rho=−0.378, p=0.018), but no significant correlation with brainstem FSS (Rho=−0.314, p=0.058).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Volume of the ventral posterior nucleus (VPN) in patients with myelitis and brainstem involvement. Normalised volume of the VPN per participant (mean of both hemispheres) in the groups: controls and patients with neuromyelitis optica spectrum disorders, myelitis and brainstem relapses (‘NMO-Brainstem’).
Volumes of the other thalamic nuclei
In an exploratory analysis, we investigated whether other thalamic nuclei were different in NMOSD patients versus controls. Among nine nuclei, we found only the lateral posterior nucleus to be smaller in patients (table 4). When corrected for multiple comparisons, this effect became non-significant (corrected p=0.180).
Volumes of the remaining thalamic nuclei in NMOSD patients and controls
Discussion
In this study that assessed all thalamic nuclei in patients with NMOSD, we hypothesised that attack-related damage would be measurable as volume loss only in specific nuclei (LGN due to ON and VPN due to myelitis).
Indeed, LGN volume was reduced in NMOSD patients with ON history compared with controls, and also compared with patients without prior ON. Moreover, LGN volume was associated with number of ON episodes, retinal damage and visual function. These results strongly suggest anterograde degeneration in the afferent visual pathway of NMO-ON patients. Moreover, they support the use of LGN volume as an imaging marker of attack-related brain structural damage in NMOSD, with also functional relevance.
Anterograde degeneration in the visual pathway is well established in multiple sclerosis (MS),21 22 while even in radiologically isolated syndrome there seems to be an association between retinal and thalamic volume loss.23 In NMOSD, previous studies investigated transsynaptic degeneration in the visual pathway by analysing changes in the OR.15 24–27 Several studies using diffusion tensor imaging15 24 26–28 reported decreased OR fractional anisotropy, indicating microstructural OR-changes in NMO-ON patients versus controls. A further study25 showed reduced myelin water fraction, suggesting reduced myelin density, in the OR of NMOSD patients (80% with prior ON) compared with controls. The interpretation of these findings was, that axonal loss in the optic nerve(s) after ON can cause OR changes, by a propagation of damage through the LGN-synapses (anterograde transsynaptic degeneration).
However, reported microstructural damage in the OR of NMOSD patients without prior ON26 27 suggests that white matter in this region might also be prone to direct changes due to NMOSD-related astrocytopathy. Thus, the specific assessment of the LGN, the grey matter structure where the actual synapses occur, is crucial to confirm transsynaptic degeneration and measure attack-related structural damage in the visual pathway in NMOSD. Moreover, LGN volume as assessed in our study has the advantage of using a broadly available MRI sequence (three-dimensional T1-weighted). This is important, since standardised diffusion tensor imaging for the OR-assessment is often hampered in clinical routine.
The lack of data on LGN volume in NMOSD is probably due to the small LGN size, which makes its measurement technically challenging.22 A single previous study27 reported, in line with our results, reduced LGN volume in NMOSD patients with ON compared with controls and to patients without ON. In this previous study however, LGN volume was measured manually, which is prone to bias, especially for such a small structure.29 In the present study, we used a multi-atlas-based tool of automated segmentation, the MAGeT Brain algorithm.17 This algorithm is based on histological data, was validated against manual segmentations30 31 and intraoperative recordings31 and was previously used to investigate deep grey matter volume in patients with MS.29
Next to this methodological strength, the present study included a—given the rarity of NMOSD in Europe32—relatively large (n=39) number of AQP4-IgG seropositive NMOSD patients, compared with the heterogeneous population of Tian et al,27 who analysed AQP4-IgG seropositive and seronegative patients together, and to the smaller sampler sizes of previous studies investigating the visual pathway of AQP4-IgG seropositive NMOSD.15 24–26
Although previous work showed GCIPL volume reduction6 and microstructural OR changes26 in AQP4-IgG seropositive NMO-NON patients, our current results do not support a subclinical LGN volume loss in the absence of ON, since NMO-NON patients had normal LGN volumes. The reasons for this are not clear. It could be that neurodegenerative processes are different in the retina than the brain and in the white- than the grey matter in NMOSD. However, it cannot be ruled out that in this cross-sectional study we had insufficient power to detect subtle subclinical volume loss at the LGN level.
The LGN volume was not associated with OR lesions in our study. This is in contrast to what was shown in MS,33 where findings suggest retrograde degeneration from OR lesions towards the retina.34 The reason for this could be, that the typically small, non-specific lesions observed in the OR of NMOSD patients are less destructive than demyelinating OR lesions in MS. This would be in line with the non-specific morphology and asymptomatic nature of most white matter brain lesions in NMOSD.35–37
In contrast to the LGN findings, VPN volume was not smaller in NMOSD patients with myelitis versus controls and did not correlate with number of myelitis episodes. One possible explanation for these negative findings is, that compared with the small LGN, which receives afferences almost exclusively from the retina/optic nerve, the VPN is a larger nuclear complex receiving afferences from several regions.38 Moreover, the VPN as segmented in the present study included not only the ventral posterolateral subnucleus (receiving afferences from the spinal cord), but also the ventral intermediate nucleus and the ventral posteromedial subnucleus. The latter receives afferences from the trigeminothalamic tract in the brainstem.39 Accordingly, we found reduced VPN volumes in five patients who suffered brainstem relapses. Four of these patients had attacks with brainstem or area postrema syndromes and cervical myelitis, with MRI lesions extending from the brainstem into the cervical spinal cord. We speculate that a lesion located in the most cranial part of the spinal cord (ie, at a shorter distance from the VPN) and the brainstem (ie, close to the spinal tract of the trigeminal nerve and/or the trigeminothalamic tract) might be associated with the VPN volume loss seen in these patients.
Another possible explanation for the lack of association between VPN and myelitis is the heterogeneous population of patients, with different degrees of sensory involvement, as well as spinal cord lesions with different lengths and locations. Last, it should be emphasised that lack of volume loss in the VPN does not necessarily mean lack of damage. Microstructural changes that do not necessarily result in a volume reduction or functional, adaptive changes could be present in the grey matter, despite ‘normal’ volume.
The volume of the entire thalamus was not reduced in our NMOSD patients compared with controls, which is in line with three previous European studies13–15 with AQP4-IgG seropositive patients. However, three other Asian studies11 12 16 reported reduced thalamic volumes compared with controls. In one of these studies,12 seven thalamic subregions (not corresponding to specific subnuclei) were also examined separately and almost all showed reduced volumes in NMOSD. These overall conflicting findings may be due to the genetically different NMOSD populations in Europe and Asia40 and due to variability in antibody-status of the patients, with the Asian studies including also 10%–30% AQP4-IgG seronegative patients.11 12 16
A limitation of our study is the use of volume changes as the only measure of thalamic damage. Quantitative imaging methods, such as diffusion tensor imaging of thalamic nuclei, or even functional MRI might contribute to our understanding of microstructural and functional changes in NMOSD that do not necessarily result in volume loss, although their application in such small structures as the thalamic nuclei would be technically challenging. Moreover, the cross-sectional nature of the present study is a drawback. Longitudinal studies following changes in thalamic nuclei in patients with NMOSD after an acute (ideally the first) attack would be warranted in the future.
To conclude, we found structural damage of the LGN due to ON in AQP-IgG seropositive NMOSD patients. Our results support the role of this thalamic nucleus as an imaging marker of attack-related neurodegenerative damage in the brain of these patients, also with functional relevance (association with visual function). Similar results were not observed for VPN and myelitis, although we saw an association with brainstem attacks, which needs confirmation in larger studies. Our findings suggest selective, attack-related rather than diffuse damage to thalamic nuclei in NMOSD.
Supplemental material
Supplemental material
Acknowledgments
We thank all patients and controls that participated in this study, Charlotte Bereuter for performing the visual assessment and optical coherence tomography, as well as Susan Pikol and Cynthia Kraut for performing the magnetic resonance imaging.
References
Footnotes
Contributors Conception and design of the study: AP and AB. Acquisition, analysis and interpretation of data: AP, FCO, LG, JK, HZ, CC, NS, SA, JB-S, KR, MC, MS, SM, JW, FP and AB. Drafting the manuscript or figures: AP, FCO, JK, HZ, CC, NS, MC, SM, JW, FP and AB.
Funding This study was supported by the ‘Deutsche Forschungsgemeinschaft’ (grant DFG Exc. 257) and the German Federal Ministry for Education and Research (BMBF; grant N2-ADVISIMS: 16GW0079) to FP and AB and by the Swiss National Science Foundation (project number P300PB_174480) to AP.
Competing interests AP has received speaker-fee from Sanofi-Genzyme and travel support from Bayer AG, Teva and F. Hoffmann-La Roche. Her research was supported by the University of Basel, the Swiss Multiple Sclerosis Society and the ‘Stiftung zur Förderung der gastroenterologischen und allgemeinen klinischen Forschung sowie der medizinischen Bildauswertung’. The current research work was supported by the Swiss National Science Foundation (Project number: P300PB_174480). FCO was employee of Nocturne UG, not in context of this work. LG was a temporary employee of Novartis AG and is currently an employee of F. Hoffmann-La Roche; her contribution to this work was prior to her employment in F. Hoffmann-La Roche. JK received conference registration fees from Biogen and financial research support from Krankheitsbezogenes Kompetenznetzwerk Multiple Sklerose (KKNMS). HZ received research grants from Novartis and speaker fees from Teva. CC has nothing to disclose. NS has nothing to disclose. SA reports travel grants from Celgene, unrelated to this project. JB-S has received travel grants and speaking fees from Bayer Healthcare, Biogen Idec, Merck Serono, Sanofi-Aventis/Genzyme, Teva Pharmaceuticals, and Novartis. KR served on the scientific advisory board for Sanofi-Aventis/Genzyme, Novartis, and Roche; received travel funding and/or speaker honoraria from Bayer Healthcare, Biogen Idec, Merck Serono, Sanofi-Aventis/Genzyme, Teva Pharmaceuticals, Novartis, and Guthy Jackson Charitable Foundation; is an academic editor for PLoS ONE; receives publishing royalties from Elsevier; and received research support from Novartis and German Ministry of Education and Research. MC has nothing to disclose. MS has nothing to disclose. SM has received research support from Swiss MS Society, Swiss National Science Foundation, University of Basel and Stiftung zur Förderung der gastroenterologischen und allgemeinen klinischen Forschung sowie der medizinischen Bildauswertung. He also received travel support from Biogen and Genzyme. JW is CEO of MIAC AG Basel, Switzerland. He served on scientific advisory boards of Actelion, Biogen, Genzyme-Sanofi, Novartis, and Roche. He is or was supported by grants of the EU (Horizon2020), German Federal Ministeries of Education and Research (BMBF) and of Economic Affairs and Energy (BMWI). FP serves on the scientific advisory board for Novartis; received speaker honoraria and travel funding from Bayer, Novartis, Biogen Idec, Teva, Sanofi-Aventis/Genzyme, Merck Serono, Alexion, Chugai, MedImmune, and Shire; is an academic editor for PLoS ONE; is an associate editor for Neurology® Neuroimmunology and Neuroinflammation; consulted for SanofiGenzyme, Biogen Idec, MedImmune, Shire, and Alexion; and received research support from Bayer, Novartis, Biogen Idec, Teva, Sanofi-Aventis/Genzyme, Alexion, Merck Serono, German Research Council, Werth Stiftung of the City of Cologne, German Ministry of Education and Research, Arthur Arnstein Stiftung Berlin, EU FP7 Framework Program, Arthur Arnstein Founda-tion Berlin, Guthy Jackson Charitable Foundation, and National Multiple Sclerosis of the USA. AUB is cofounder and shareholder of technology startups Motognosis and Nocturne UG. He is named as inventor on several patent applications describing MS serum biomarkers, perceptive visual computing and retinal image analysis.
Patient consent for publication All participants gave written informed consent before inclusion in the study.
Ethics approval Ethikkommission der Charité—Universitätsmedizin Berlin (EA1/131/09).
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Data are available upon reasonable request.