Single photon emission computed tomography in the identification of new variant Creutzfeldt-Jakob disease: case reports
BMJ 1998; 316 doi: https://doi.org/10.1136/bmj.316.7131.593 (Published 14 February 1998) Cite this as: BMJ 1998;316:593
- Rajith de Silva, medical physicist,
- James Patterson, medical physicista,
- Donald Hadley, consultanta,
- Aline Russell, senior registrarb,
- Martin Turner, consultantc,
- Martin Zeidler, research fellowd
- a Department of Neuroradiology, Southern General Hospital
- b Department of Electrophysiology, Southern General Hospital
- c Woodilee Psychiatric Hospital, Lenzie G66 3UG
- d National CJD Surveillance Unit, Western General Hospital, Edinburgh EH4 2XU
- Correspondence to: Dr de Silva
- Accepted 21 July 1997
See editorial by Pocchiari and p 577
New variant Creutzfeldt-Jakob disease may be associated with exposure to the causative agent of bovine spongiform encephalopathy.1 Currently, a reliable diagnosis is possible only after neuropathological examination of the brain, which is risky for patients and diagnosticians.2 The sensitivity and specificity of recently developed techniques are not known for new variant Creutzfeldt-Jakob disease, and they are available only in highly specialised centres. 3 4
Single photon emission computed tomography is a readily available neuroimaging technique that uses intravenously administered radioactive ligands to map different aspects of brain function.
We report the findings on this technique using the cerebral perfusion tracer hexamethylpropyleneamineoxime (HMPAO) in two patients with neuropathologically confirmed new variant Creutzfeldt-Jakob disease.
Patients, methods, and results
Case 1 —A 28 year old woman developed paraesthesia of her right arm, then right leg, and later both left arm and leg. Six months later she complained of weight loss and fatigue, and had mild ataxia. After 1 year, speech, memory, and behavioural abnormalities were identified, her ataxia had worsened, and choreiform movements were noted. Six months later she developed myoclonus, primitive responses, pyramidal signs, and severe limb and truncal ataxia. Finally, she became rigid and mute; she died 23 months after the onset of her symptoms. An electroencephalogram taken 11 months after initial presentation showed no abnormalities. A repeat tracing 3 months later showed no abnormalities either, and at that time, results from magnetic resonance imaging of the brain were reported as normal apart from showing mild atrophy. Simultaneous single photon emission computed tomography showed hypoperfusion, most marked in the left temporoparietal region. The diagnosis of new variant Creutzfeldt-Jakob disease was established histopathologically.
Case 2 —A woman aged 34 was admitted to a psychiatric unit with a 9 month history of presumed agitated depression. Neurological examination gave normal results, and antidepressant treatment was started. Over the next 2 months she developed delusional thoughts and became unsteady. An electroencephalogram showed diffuse slowing, and magnetic resonance imaging of the brain was reported to be normal. She continued to deteriorate with worsening psychiatric symptoms, progressive ataxia, bulbar palsy, and incontinence. Single photon emission computed tomography (two weeks after the magnetic resonance study) showed widespread reduction in cortical perfusion (figure). Over the ensuing months she became more withdrawn, ataxic, and rigid. Finally, she had rest and stimulus sensitive myoclonus, and was mute. She died 14 months after the onset of her illness. The histopathological findings were characteristic of new variant Creutzfeldt-Jakob disease. Serial electroencephalographic recordings (the last was performed 10 days before her death) showed progressive slowing of background rhythms but no typical periodic complexes.
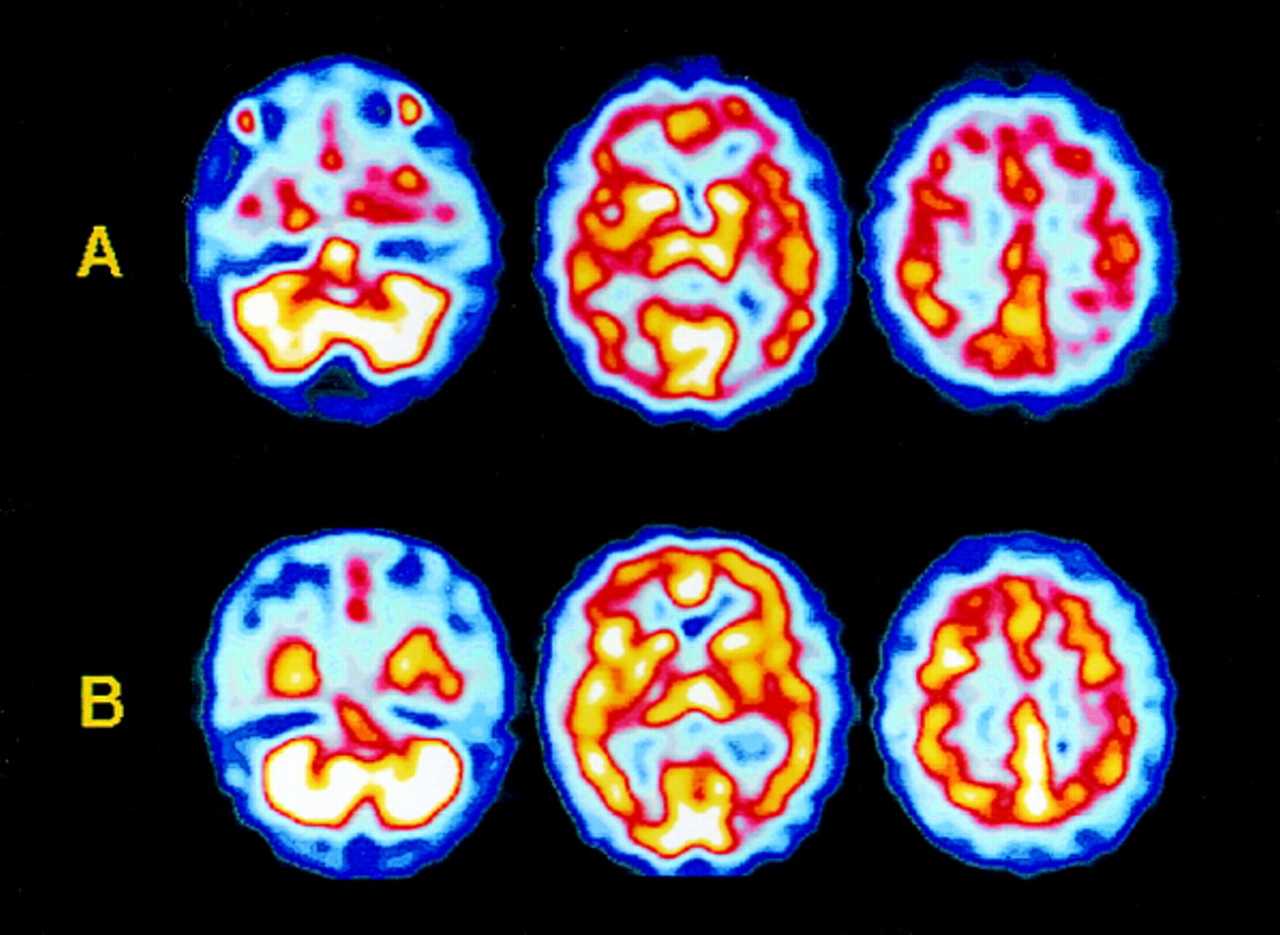
Axial sections on single photon emission computed tomography through cerebellum, basal ganglia, and parietal region in case 2 (A) showing widespread reduction in cortical perfusion, and in age matched, healthy subject (B) for comparison
{kind=link}
Comment
The two patients presented consecutively at this institute, and necropsy confirmed that they had died of new variant Creutzfeldt-Jakob disease. As with other cases of the disease identified to date, early diagnosis was hampered by the absence or subtlety of neurological features, and by comparatively normal results in investigations. The clinically important abnormalities of cerebral perfusion on single photon emission computed tomography, when findings on electroencephalography or cerebral magnetic resonance imaging were normal, raised or supported the diagnosis of an organic encephalopathy in both cases. Similar abnormalities shown in single photon emission computed tomography have been reported in sporadic Creutzfeldt-Jakob disease, and a patient who died 7 weeks after onset had a unilateral perfusion deficit corresponding to the clinical, electroencephalographic, and pathological abnormality.5 Although the perfusion abnormalities seen here are non-specific and cannot be claimed to be diagnostic of new variant Creutzfeldt-Jakob disease, they are more marked and widespread than those associated with depression. Consequently, the technique may prove useful in raising the possibility of the disease in young patients presenting with unusual psychiatric or neurological syndromes, with normal or unhelpful results in routine investigations.
Acknowledgments
We thank Professor Ian Bone and Dr William Durward for giving their permission to publish these cases. The histopathological examinations were performed at the National CJD Surveillance Unit by Dr James Ironside.
Contributors: RdeS, JP, and DH raised the possibility of using single photon emission computed tomography as a diagnostic “pointer” in new variant Creutzfeldt-Jakob disease, and RdeS wrote the paper. AR, MT, and MZ discussed the core concept and suggested amendments to the early drafts. JP and DH reviewed the final manuscript. MT contributed psychiatric data in case 2, and AR interpreted the electrophysiological data. JP and DH interpreted the single photon emission computed tomograms. DH interpreted the other radiological studies and collated these with the single photon emission computed tomography scans. MZ was involved in establishing the final diagnoses.
Funding: None.
Conflicts of interest: None.