Article Text

Statistics from Altmetric.com
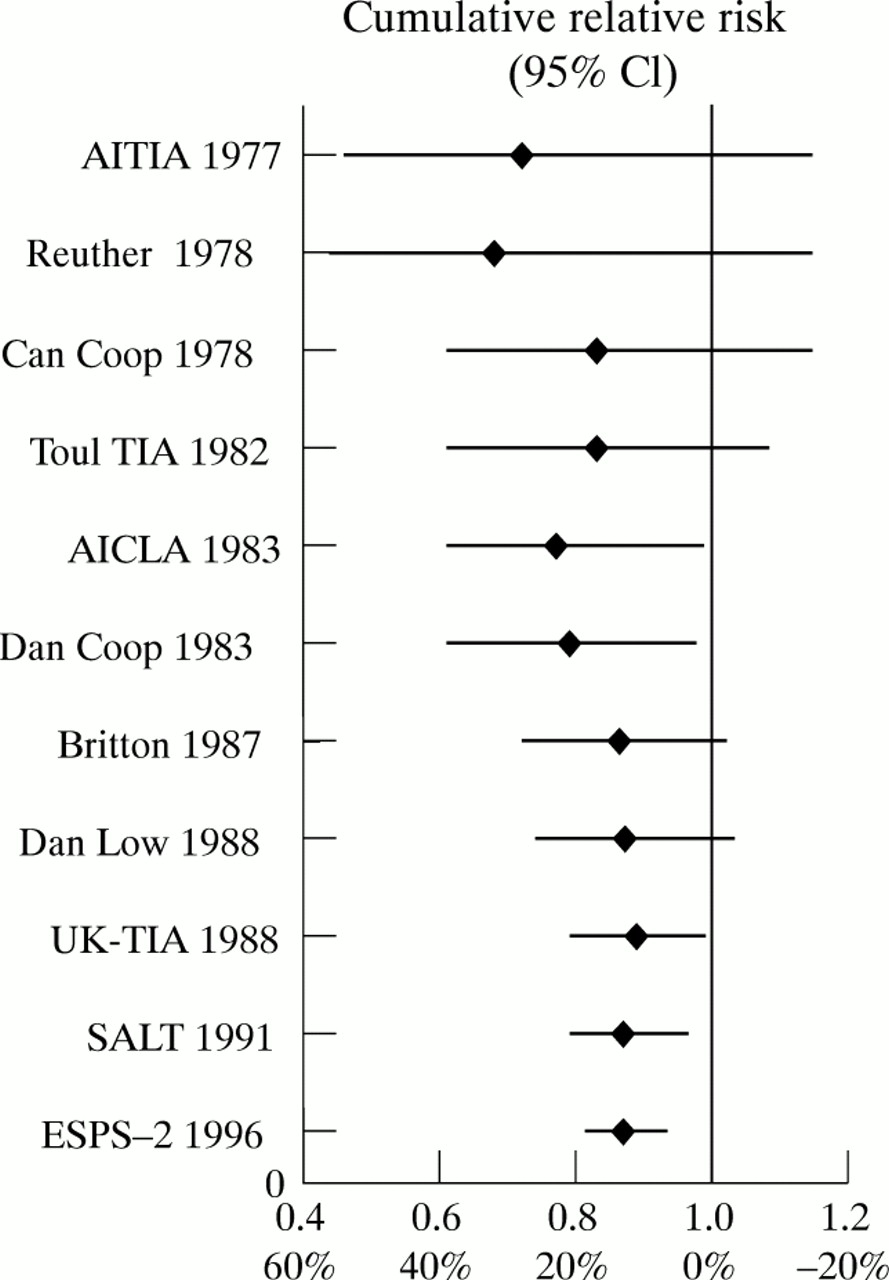
In 1996 we reported in this Journalthat there was virtually no difference in relative risk reduction for low (<100 mg/day), medium (300 to 325 mg/day), and high (>900 mg/day) doses of aspirin in the prevention of vascular events in patients with cerebral ischaemia of arterial origin.1 A meta-analysis of the cumulative data showed a modest 13% (95% confidence interval (95% CI) 4% to 21%) relative risk reduction. Recently the final data of the second European Stroke Prevention Study (ESPS-2) were reported.2 One of its comparisons was between 50 mg aspirin daily and placebo in patients after cerebral ischaemia; the relative risk reduction of 13% (95% CI 0% to 24%) was exactly the same as that resulting from our previous meta-analysis. This similarity allows the calculation of an update of the meta-analysis. The overall relative risk reduction of course remains 13%, but the 95% CI has narrowed to 6% to 19%. The figure shows the results of the updated cumulative meta-analysis, in chronological order. These data once more underscore the need for more efficacious treatment strategies. For this reason we started the European and Australian Stroke Prevention in Reversible Ischaemia Trial (ESPRIT).3

{kind=link}
Cumulative meta-analysis in chronological order (1977 to 1996) with relative risks and corresponding relative risk reductions with 95% CIs. Each line represents the relative risk and 95% CI of that study combined with all previous studies.