Article Text

Statistics from Altmetric.com
Natalizumab is a disease-modifying therapy (DMT) used in relapsing-remitting multiple sclerosis (RRMS), licenced for use in patients with highly-active disease. It is an α4-integrin receptor antagonist that decreases activated T cell migration across the blood-brain barrier.1 Natalizumab carries a risk of progressive multifocal leucoencephalopathy (PML)—a risk that increases with duration of treatment; John Cunningham Virus (JCV) seropositivity and higher index values; prior use of immunosuppression.1 Patients may choose to withdraw from natalizumab to mitigate PML risk, or less commonly when natalizumab fails to control disease activity, or is poorly tolerated. Fingolimod has been commonly used as an option in those making the switch from natalizumab, but is associated with high rates of breakthrough clinical and/or radiological disease activity, although the risks may be lower with shorter washout periods.2 Rituximab has been suggested as an alternative to fingolimod in patients discontinuing natalizumab due to high PML risk, however, rituximab is not licenced for the treatment of RRMS and is not available in some countries for this indication.3
Alemtuzumab is a monoclonal antibody that binds to the CD52 surface protein on T and B lymphocytes, resulting in their depletion with subsequent repopulation, with comparable efficacy to natalizumab.1 Switching to alemtuzumab might be an alternative to fingolimod in patients stopping natalizumab but there is a paucity of clinical and safety data to guide this transition. Here, we present a single-centre experience in switching from natalizumab to alemtuzumab in RRMS.
Methods
We retrospectively identified patients from the National Hospital for Neurology and Neurosurgery who switched from natalizumab to alemtuzumab from May 2015 to February 2018. We extracted data from the medical records: demographic characteristics, duration of natalizumab use, drug washout period, cerebrospinal fluid (CSF) examination results, JCV serology, clinical disease activity (relapses) before and after commencing alemtuzumab, Expanded Disability Status Scale (EDSS) scores, MRI measures of disease activity (number of new T2 and gadolinium enhancing lesions) pre-alemtuzumab and post-alemtuzumab and adverse events. All data are presented as mean (SD) unless otherwise stated.
Results
19 patients (mean age 38 (11) years, 10 (53%) female) were identified who switched from natalizumab to alemtuzumab. Mean disease duration from onset at the time of receiving alemtuzumab was 10 (7) years and the median number of natalizumab infusions prior to switching was 41 (range 8–95). Natalizumab was the first DMT taken in 5 (26%) patients. The annualised relapse rate (ARR) in the 12 months prior to commencing alemtuzumab was 0.74 and median EDSS was 6.5 (1.5–8.0).
The reasons for changing treatment were: PML risk (n=11), lack of efficacy (n=6), tolerability (n=1) and family planning (n=1). Fifteen (79%) patients were JCV-positive; all JCV-positive patients had an MRI brain and 12/15 (80%) had CSF to check JCV-PCR before starting alemtuzumab. The mean washout period in the entire cohort was 128 days (median 120; range 28–307). The washout period was ≥12 weeks in 17 (89%) patients.
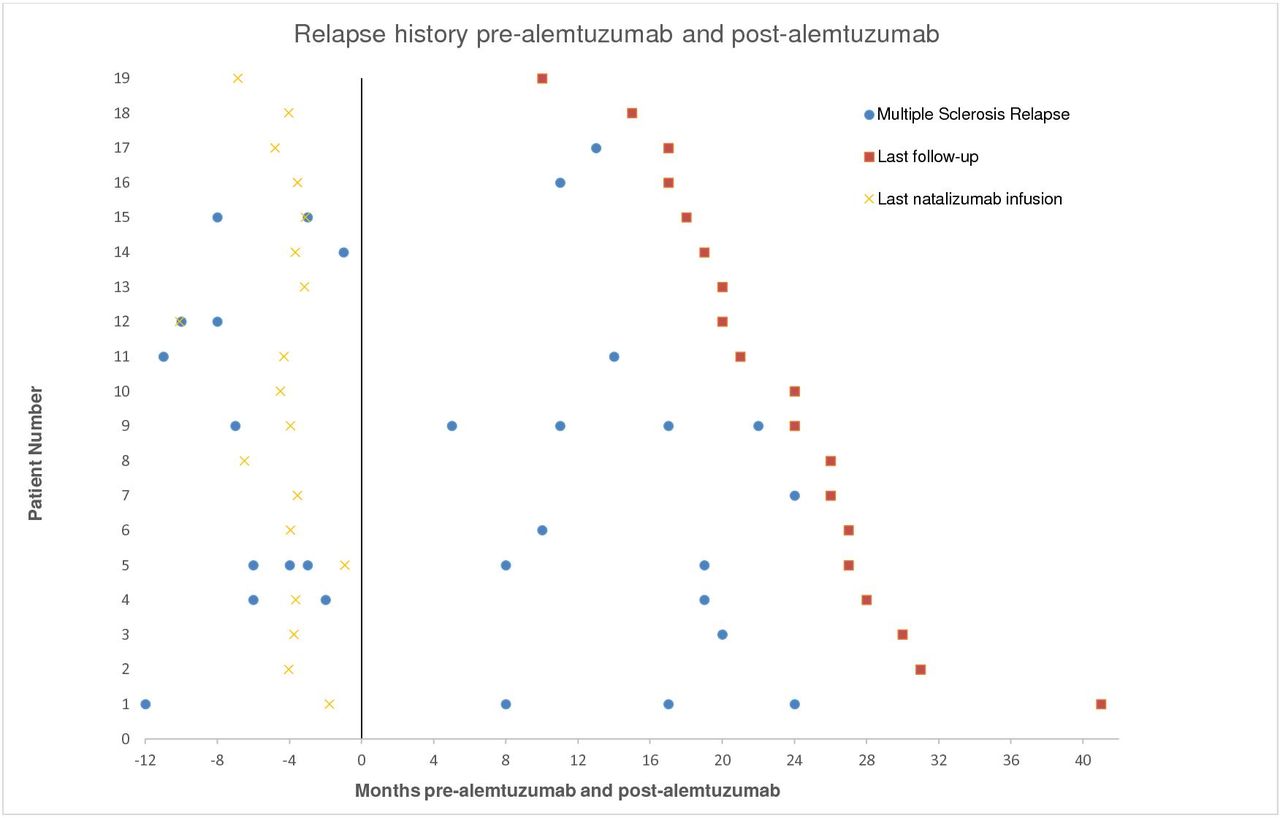
18/19 patients had at least 12 months clinical follow-up after starting alemtuzumab (median 22; (range 8–39)). Sixteen relapses occurred in 10/19 (53%) (figure 1), including 5/6 (83%) who switched from natalizumab to alemtuzumab because of ongoing disease activity. There was no significant difference in the ARR in the 12 months pre-alemtuzumab and post-alemtuzumab in those switching due to lack of efficacy (1.83 vs 0.67, p=0.07) or in those switching with inactive disease (0.23 vs 0.15, p=0.72). EDSS scores remained stable in 12 patients, improved in three patients and worsened in three patients; follow-up EDSS score was not available for one patient. Of the 17 patients who have had follow-up MRI, 5/17 (29%) demonstrated new MRI activity: three patients had new T2 lesions at the 12-month follow-up MRI (after starting alemtuzumab) and two patients developed a single gadolinium enhancing lesion seen 6 months post second cycle of alemtuzumab.

{kind=link}
Relapse history in relation to alemtuzumab commencement and last natalizumab infusion.
The mean lymphocyte counts 1 month after the first and second cycle of alemtuzumab was 0.39 (0.34) and 0.37 (0.20), respectively. In patients who experienced a relapse post alemtuzumab versus those who had stable disease, there was no difference in the mean lymphocyte count 1 month after the first (0.39 vs 0.40, p=0.60) or second cycles (0.44 vs 0.23, p=0.06).
Adverse events were in keeping with the known side effect profile of alemtuzumab. 17/19 (89%) had infusion reactions during at least one of the alemtuzumab cycles and two patients had urticaria and erythema multiforme, respectively. 10/19 (53%) developed an infection during the post-alemtuzumab follow-up period with the most common being urinary tract infections (14 infections) and upper respiratory tract infections (five infections). There was one case of herpes zoster opthalmicus. There were no cases of secondary autoimmunity to date, and no PML.
Discussion
Our series of consecutive patients suggests that alemtuzumab may be a reasonable option in patients stopping natalizumab, especially in patients with stable disease who are changing their therapy because of PML risk. In such patients, the goal is to minimise the risk of carry-over PML while maintaining control of disease activity. Giovannoni and colleagues provide an approach to managing the switch from natalizumab to alemtuzumab by using an initial MRI and CSF JCV DNA-PCR to exclude subclinical PML (small risk of false negative results) followed by a direct switch, 3–6 months washout before commencing alemtuzumab or starting an oral bridging agent within 2–4 weeks and using this for 6–12 months before starting alemtuzumab.4 Using MRI and CSF JCV-PCR to exclude subclinical PML prior to switching, and a median washout period of 120 days, there have been no cases of PML in our cohort. Our experience is similar to Malucchi and colleagues, who reported on 16 patients with stable RRMS, switching to alemtuzumab due to PML risk after a median washout period of 70 days (41–99). At 12 months follow-up, there were no cases of PML or breakthrough disease activity.5
Our results suggest that alemtuzumab may not prevent breakthrough disease activity in patients who discontinued natalizumab because of lack of efficacy. While there is a paucity of published data examining cohorts switching solely due to lack of efficacy, Pfeuffer and colleagues in a retrospective analysis of 143 patients who switched from natalizumab to either fingolimod or alemtuzumab, suggest that patients switching to alemtuzumab had lower rates of disease activity compared with those switching to fingolimod.6 Previous studies examining washout periods when switching from natalizumab suggest that the risk of breakthrough disease activity increases with washout periods greater than 8–12 weeks.2 7 In our cohort, the high proportion of cases with breakthrough disease activity in those switching due to lack of efficacy is only partly explained by the duration of the washout. Recent work has also shed light on lymphocyte depletion following alemtuzumab administration, its potential link to anti-alemtuzumab antibodies and the impact this may have on breakthrough disease activity at an individual level.8 9 These factors may have played a role in the development of breakthrough disease activity in our cohort given the trend towards higher lymphocyte counts post second cycle in those who experienced a relapse post alemtuzumab. The small sample sizes made it difficult to detect differences in postalemtuzumab lymphocyte counts between these two groups. Other options such as autologous haematopoietic stem cell transplantation may need to be considered in patients who fail natalizumab because of ongoing disease activity.3 Limitations of our study include the small sample size and retrospective study design. Larger prospective studies are required to further assess the efficacy and safety of alemtuzumab in patients previously treated with natalizumab.
Footnotes
Contributors NJ and WJB planned the study. NJ and AC were involved in data acquisition. NJ completed data analysis and drafted the manuscript. WJB provided key edits to the manuscript. The final manuscript was reviewed and edited by AC, WJB and JC. The guarantor for the content of the manuscript is JC.
Competing interests WJB has received speaker honoraria for educational activities for Merck Serono, Roche and Sanofi Genzyme. JC has received support from the Efficacy and Mechanism Evaluation Programme and Health Technology Assessment Programme (NIHR); UK Multiple Sclerosis Society and National Multiple Sclerosis Society; National Institute for Health Research University College London Hospitals (NIHR-UCLH) Biomedical Research Centre (BRC) and University College London. In the last three years, he has been a local principal investigator for trials in multiple sclerosis funded by: Receptos, Novartis and Biogen Idec, and has received an investigator grant from Novartis outside this work. He has taken part in Advisory Boards/consultancy for Apitope, Roche, Merck, MedDay, Biogen and Celgene.
Patient consent for publication Not required.
Ethics approval The study was approved by the Queen Square Quality and Safety Committee, National Hospital for Neurology and Neurosurgery.
Provenance and peer review Not commissioned; externally peer reviewed.