Article Text

Abstract
Objective Myasthenia gravis (MG) is the most common autoimmune disorder affecting the neuromuscular junction. However, evidence shaping treatment decisions, particularly for treatment-refractory cases, is sparse. Both rituximab and eculizumab may be considered as therapeutic options for refractory MG after insufficient symptom control by standard immunosuppressive therapies.
Methods In this retrospective observational study, we included 57 rituximab-treated and 20 eculizumab-treated patients with MG to compare the efficacy of treatment agents in generalised, therapy-refractory anti-acetylcholine receptor antibody (anti-AChR-ab)-mediated MG with an observation period of 24 months. Change in the quantitative myasthenia gravis (QMG) score was defined as the primary outcome parameter. Differences between groups were determined in an optimal full propensity score matching model.
Results Both groups were comparable in terms of clinical and demographic characteristics. Eculizumab was associated with a better outcome compared with rituximab, as measured by the change of the QMG score at 12 and 24 months of treatment. Minimal manifestation of disease was more frequently achieved in eculizumab-treated patients than rituximab-treated patients at 12 and 24 months after baseline. However, the risk of myasthenic crisis (MC) was not ameliorated in either group.
Interpretation This retrospective, observational study provides the first real-world evidence supporting the use of eculizumab for the treatment of refractory, anti-AChR-ab positive MG. Nonetheless, the risk of MC remained high and prompts the need for intensified monitoring and further research effort aimed at this vulnerable patient cohort.
- myasthenia
- neuromuscular
- neuroimmunology
Data availability statement
Data are available upon reasonable request. All data relevant to the study are included in the article or uploaded as supplementary information. All analysed data are presented in the manuscript and available upon reasonable request from qualified investigators.
This is an open access article distributed in accordance with the Creative Commons Attribution 4.0 Unported (CC BY 4.0) license, which permits others to copy, redistribute, remix, transform and build upon this work for any purpose, provided the original work is properly cited, a link to the licence is given, and indication of whether changes were made. See: https://creativecommons.org/licenses/by/4.0/.
Statistics from Altmetric.com
Introduction
Myasthenia gravis (MG) is the most common autoimmune disorder affecting the neuromuscular junction, characterised by antibody (ab)-mediated dysfunction of the postsynaptic membrane.1 The hallmark of MG is fluctuating weakness of ocular, bulbar, limb and respiratory muscles, with corresponding morbidity and mortality.2
In the majority of patients with MG, disease is sufficiently controlled by immunosuppressive treatment, while a clinically distinct subgroup of patients, often referred to as refractory, continues to experience severe disease despite therapy.2 3 Nonetheless, a consensus for the definition of refractory MG is currently lacking, with various studies employing heterogeneous definitions.3 Treatment strategies are evolving with novel biological agents complementing existing standards of therapy. Rituximab, a B cell-depleting monoclonal antibody (ab), has been discussed as potential therapy for patients with MG whose disease is refractory to standardised immunotherapies.4 This viewpoint is supported by findings from a meta-analysis of smaller case series as well as observational studies investigating rituximab for new-onset MG in patients who are anti-acetylcholine receptor (AChR)-ab positive5 and for anti-muscle-specific tyrosine kinase (MuSK)-ab positive.6 Concurrently, identification of complement as major driver of disease activity in anti-AChR-ab MG7 led to the development of complement-targeted therapies. As such, eculizumab is a humanised, monoclonal ab that specifically recognises and inhibits cleavage of complement C5.8 Ablation of terminal complement activation by eculizumab has proven efficacious for treating patients with anti-AChR-ab positive treatment-refractory (TR) MG in the phase 3, randomised, placebo-controlled REGAIN trial.9
Both biologicals, that is, rituximab and eculizumab, may be considered as treatment options for refractory MG after failure of immunosuppressive standard therapies (ISTs).5 9 10 However, evidence guiding treatment strategies is sparse. Thus, we compared rituximab and eculizumab for the treatment of generalised, therapy-refractory anti-AChR-ab positive MG in a retrospective, observational study. The change to baseline quantitative myasthenia gravis (QMG) score was employed as the primary outcome parameter with a follow-up period of 24 months. Study outcomes were specified prior to data analysis.
Material and methods
Study cohort
Our cohort is a retrospective, observational multicentric analysis of patients from six university hospitals (University Medicine Charité Berlin, University Hospital Cologne, University Hospital Duesseldorf, University Hospital Freiburg, University Hospital Magdeburg and University Hospital Regensburg). A total of 815 patients with MG were recruited with a focus on TR cases. Diagnosis of MG was established by characteristic clinical presentation and supported by characteristic antibody (ab) findings in accordance with national guidelines.11 Participating centres are established as the integrated Myasthenia Centre (iMC) by the German Myasthenia Gravis Society, employing standardised workflows for patient management. According to the iMC protocol, patients with a stable course were seen every 6 months and unstable patients more frequently. Data were collected according to the standards of the German Myasthenia registry and included sociodemographic data (age, sex and disease duration), ab-status (AChR, MuSK, lipoprotein-related protein 4 or seronegative), MG-specific medication (cholinesterase inhibitors, glucocorticoids and immunosuppressants), history of thymectomy, and comorbidities. The scoring of MG-specific parameters was performed by the treating neurologist. No clinical scoring was applied retrospectively.
Patient cohort and selection
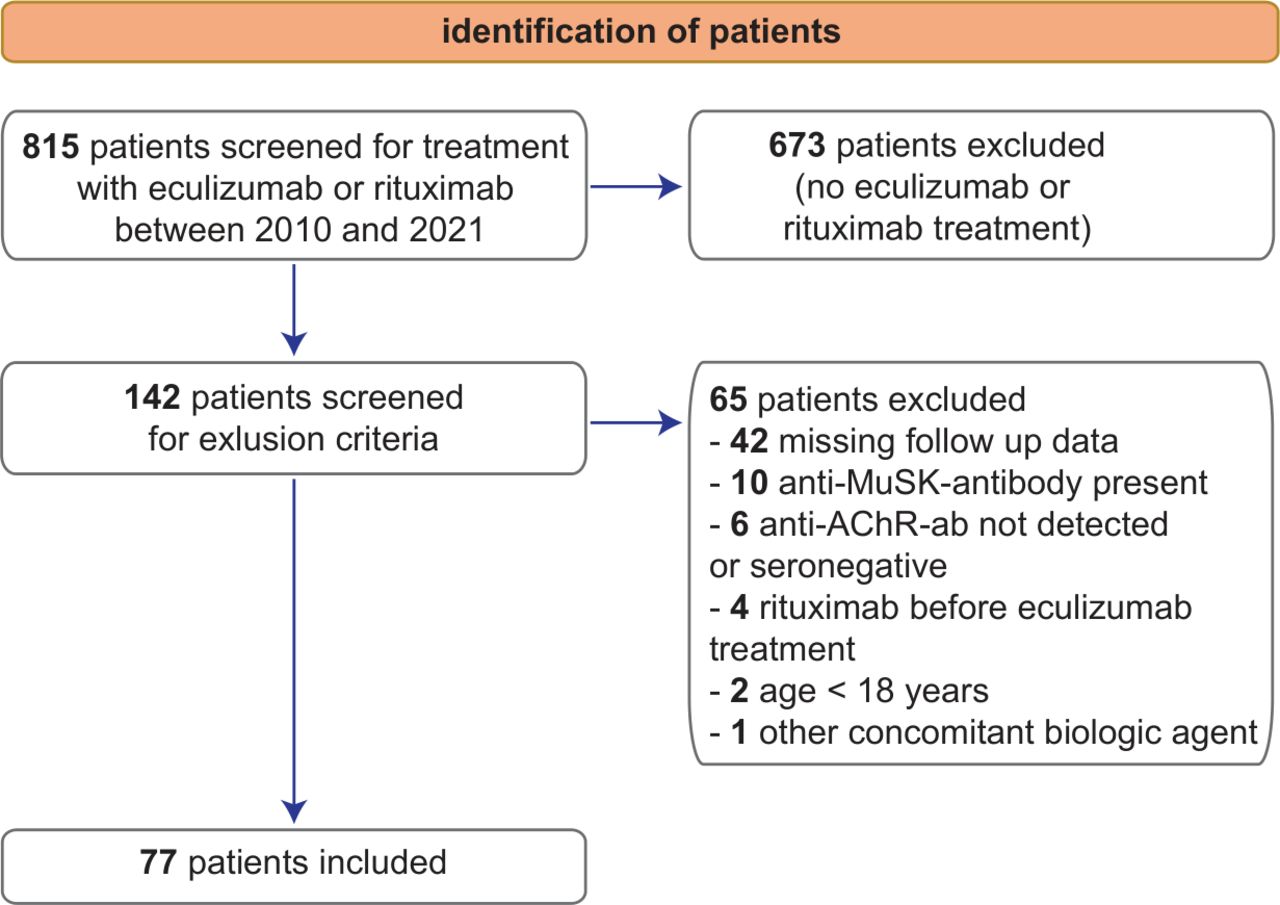
We identified 142 patients treated with rituximab or eculizumab between 2010 and 2021 (figure 1).
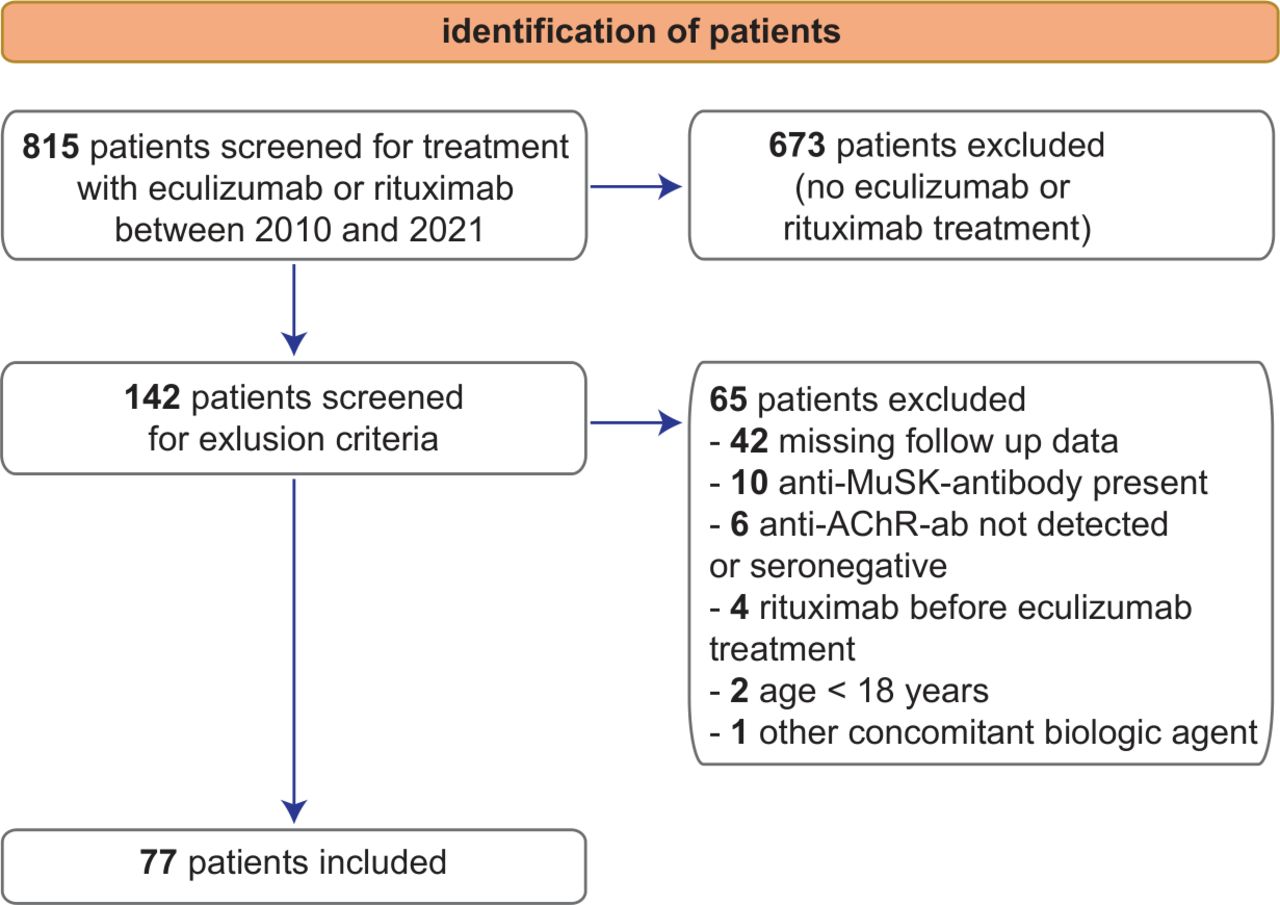
Flow chart detailing patient recruitment. Seventy-seven patients were included in the final study for rituximab (n=57) and eculizumab treatment (n=20). ab, antibody; AChR, acetylcholine receptor; MuSK, muscle-specific tyrosine kinase.
The following inclusion criteria were applied:
Confirmed diagnosis of MG in accordance with national guidelines.
Confirmed serological detection of anti-AChR-ab.
Age≥18 at start of rituximab or eculizumab treatment.
Treatment refractory MG according to the following definition3: persistent impairment due to MG despite adequate standard therapy for more than 12 months or persistent intolerable side effects. In this study, we employed generalised disease with a QMG score of ≥6 as operational definition for persistent impairment. Standard therapy was defined as having received two previous first-line ISTs or one first-line IST and prednisolone at maximum tolerable dose for a minimum treatment duration of 6 months each without achieving disease control or until treatment has to be stopped due to intolerable side effects. Standard ISTs included azathioprine, mycophenolate mofetil, methotrexate or cyclosporine. Acetylcholinesterase inhibitors were required to be at a maximum tolerable dose. Thymectomy was performed if indicated.
Sufficient clinical follow-up data with at least three out of four QMG scores assessed by a trained neurologist at baseline, that is, start of rituximab or eculizumab treatment, as well as at 6 months, 12 months and 24 months after therapy initiation.
Additionally, the following exclusion criteria was applied during patient selection:
Presence of ab other than anti-AChR-ab (anti-titin-ab were permitted as these are considered complementary markers to anti-AChR-ab).
Presence of IST or a biological agent other than rituximab or eculizumab (rescue treatments including plasmapheresis (PLEX), intravenous immunoglobulins (IVIG) and immune adsorption (IA) were permitted).
Previous treatment with rituximab for eculizumab patients or eculizumab for rituximab patients.
Pregnancy during the treatment period.
Following selection using the inclusion and exclusion criteria, 57 patients treated with rituximab and 20 patients treated with eculizumab were included in the analysis (figure 1). The first patient of this cohort was treated with rituximab in 2010. Until 2017, a total of 39 patients received rituximab. The remaining 18 rituximab-treated patients were included between 2017 and 2021. After formal approval for MG, the first patient received eculizumab in 2017. All eculizumab-treated patients were recruited between 2017 and 2021. During this period, eculizumab was preferentially offered due to its on-label status. If patients declined eculizumab, rituximab was offered instead.
Dosing regime
Rituximab and eculizumab treatment regimens were performed in accordance with local standard operating procedure. For rituximab, a dose of 1000 mg was given 14 days apart. The treatment interval for maintenance therapy with 1000 mg was 6–9 months, depending on clinical response.11 For eculizumab, treatment started with 900 mg weekly for 4 weeks followed by maintenance therapy at week 5 with 1200 mg in a biweekly application scheme.
Definitions
Myasthenic crisis (MC) was defined as a rapid clinical deterioration requiring non-invasive or invasive ventilation.12 An age of 50 years at disease onset was used as a cut-off point between early (<50 years) and late-onset (≥50 years) MG.13 IVIG, PLEX and IA were considered as rescue therapies if given for an exacerbation of MG concurrently with IST or biological agents. Recurrent IVIG infusions were defined as IST if given without other IST or biological agents. Minimal manifestation (MM) was defined based on the Myasthenia Gravis Foundation of America post-intervention status.14 For MM status, the patient was required to have no functional limitations due to MG except for minimal weakness on examination. In our study, residual weakness was required to be a QMG score of ≤3 points. For MM, symptomatic treatment with cholinesterase inhibitors was permitted. MM required that no rescue therapy was needed in the last 6 months at the time of assessment.
Standard protocol approvals, registrations and patient consents
This study was conducted in accordance with the Declaration of Helsinki. Data were anonymised and collected retrospectively according to the standards of the German Register for Myasthenia.
Study outcomes
The change from baseline QMG score after 12 months of therapy was the primary study outcome. The QMG is a 13-item scale with each item scored from 0 (no impairment) to 3 (severe impairment), for a total score ranging from 0 to 39 points.15 The change from baseline QMG score after 24 months of therapy, the time to MC and the number of patients reaching minimal manifestation at 12 and 24 months of therapy were secondary study outcomes. Patients presenting with MC that overlapped with specified time points were to be considered as missing data for the analysis of the QMG score. During this study, no overlap between MC and the specified time points of 12 and 24 months were detected. Transient worsening (that did not qualify as MC) and acute rescue therapies overlapping with the specified time points was permitted and the corresponding QMG score was recorded. Study outcomes were specified prior to data analysis.
Data availability
All analysed data are presented in the manuscript and available on reasonable request from qualified investigators.
Statistical analysis
Statistical analysis was performed using RStudio V.1.4.1103 (R-Tools Technology). Data are presented as the mean (SD) or n (%). To account for pretreatment disease severity and reduce selection bias, we employed a model of propensity score matching. The propensity scores were calculated for each patients using a logistic regression model with a priori selected covariates (sex, age at diagnosis, age at baseline, thymoma and QMG at baseline). The obtained propensity scores were subsequently entered in an Average Treatment effect on the Treated weighting model to provide a balanced sample of patients except for their respective treatment. Due to differences in sample sizes, we preferred an optimal full matching approach as to avoid a selection of patients to remain unmatched.16 As previously described,16 17 the balance between the two groups was assessed by comparing the standardised mean differences of the covariates before and after propensity score adjustment. Using a model of optimal full matching, we achieved standardised mean differences for the selected covariates below 0.1 indicating adequate balance of the two groups (online supplemental figure 1). Differences between groups were analysed using a two-tailed, unpaired T test for quantitative variables and two-tailed Fisher’s exact test for categorical variables. Group differences for time to MC were assessed through Kaplan-Meier curves and the logrank test for comparison of MC distribution. Differences were considered statistically significant with the following p values: *p<0.05, **p<0.01, ***p<0.001.
Supplemental material
Missing data
A total of three rituximab-treated (5.3%) and one eculizumab-treated (5%) patients were lost to follow-up. Clinical and demographic baseline data were indistinguishable from patients completing the full observation period (data not shown). All patients lost to follow-up were missing, that is, patients who did not complete follow-up visits and did not state a specific reason. As we detected no systematic differences between patients with missing data and those with complete data, we assumed that these data points were missing completely at random.18 Consequently, listwise deletion was applied to handle missing data points.
Results
Out of 142 patients receiving rituximab or eculizumab, we included 77 patients in the final analysis (figure 1). Distribution of baseline characteristics were comparable between the two groups (table 1). The majority of patients in both groups were women (rituximab 35 (62.5%) vs eculizumab 12 (54.6%), p=0.61), with an early onset of disease (rituximab 36 (63.1%) vs eculizumab 16 (72.7%), p=0.59). The average age at the start of rituximab and eculizumab treatment was 46.5 (SD 17.1) and 45.4 (SD 15.2) years, respectively (p=0.791). Disease severity in both groups was high with QMG scores at baseline of 10.7 (5.1) for rituximab and 13.25 (5.2) or eculizumab (p=0.056). Previous numbers of ISTs were comparable with rituximab-treated and eculizumab-treated patients receiving a median of two previous ISTs (IQR 2–3). Azathioprine was the most common previous IST in the rituximab and eculizumab group with 49 (63.4%) and 18 (90.0%) patients, respectively (p=0.126). Prednisone dose at baseline was similar, with rituximab-treated patients receiving 6.0 mg (SD 10.3) and eculizumab-treated patients 10.4 mg (SD 12.6) prednisone (p=0.121). Thymectomy was performed before baseline for all included patients. Eight rituximab-treated and four eculizumab-treated patients had a confirmed thymoma (p=0.487). No deaths or meningococcal infections were recorded during the observation period. Adverse events were in line with the known spectrum of both agents (ie, headache, nausea, diarrhoea, fever, joint pain and upper airway infections).4 19
Baseline characteristics of patients, total n=77
We compared the change to QMG baseline after 12 months of treatment with rituximab (n=56) and eculizumab (n=20) using a model of full optimal propensity score matching. After matching, the standardised mean differences of all included covariates were below 0.1 indicating adequate balance (online supplemental figure 1). Eculizumab-treated patients demonstrated a significantly greater benefit from treatment as compared with rituximab patients (QMG at 12 months for rituximab 11.2 (SD 7.3) and eculizumab 8.4 (SD 6.1); p=0.021, figure 2). In addition, we compared rituximab (n=54) and eculizumab (n=19) cohorts for changes of their QMG score to baseline at 24 months (figure 2). Here, we observed a significantly greater benefit from eculizumab treatment compared with rituximab (QMG at 24 months for rituximab 11.2 (SD 6.4) and eculizumab 9.6 (SD 8.5); p<0.001). Thymoma status did not impact the change to the QMG score at 12 or 24 months (p=0.123 and p=0.848, respectively). For two rituximab-treated and one eculizumab-treated patient, the prespecified time point of 12 months coincided with application of IVIGs. Excluding these patients from the analysis did not affect study outcomes (QMG at 12 months for rituximab 10.8 (SD 7.6) and eculizumab 8.1 (SD 6.9), p=0.038). To account for selection bias, we analysed the rituximab cohort included before 2017 (n=39) and after 2017 (n=18) (table 2). Both groups of rituximab-treated patients were similar in terms of demographic and clinical data. The change to baseline QMG at 12 months (QMG before 2017: 10.5 (SD 7.1), after 2017: 11.1 (SD 6.8), p=0.633) was comparable for both groups of rituximab-treated patients.

Changes to baseline QMG score. QMG scores were assessed at 6, 12 and 24 months. Baseline is defined as start of rituximab or eculizumab therapy. (A) Change to baseline QMG score after 12 months of treatment. (B) Change to QMG score at baseline after 24 months. Differences between groups were assessed in a model of optimal full propensity score matching. The propensity scores were calculated for each patients using a logistic regression model. Patients were matched for QMG score at baseline, sex, age at diagnosis, age at baseline and thymoma. Error bars display mean (95% CI). QMG quantitative myasthenia gravis. ***p<0.001, **p<0.01, *p<0.05, p≥0.05, not significant.
Characteristics of rituximab-treated patients before and after 2017
Next, we analysed the time to MC in both groups. During the 24-month observation period, nine patients experienced a MC in the rituximab group, while two patients deteriorated in the eculizumab group, which did not reach statistical significance (MC, n (%), rituximab 15 (15.8%) vs eculizumab 2 (10.0%), p=0.510). The time to MC did not differ between rituximab and eculizumab patients (figure 3A). For both groups, infection was the most common trigger for MC as recorded by the treating physician with 7 out of 9 MC for rituximab and 2 out of 2 MC for eculizumab. For the remaining MC, the trigger remained unknown.

{kind=link}
{kind=link}
{kind=link}
Time to myasthenic crisis after baseline. (A) Kaplan-Meier curve displaying time to myasthenic crisis after baseline. Baseline is defined as start of rituximab or eculizumab therapy. Differences between groups were assessed by logrank test. (B) Number of patients achieving minimal manifestation after 12 and 24 months of treatment according to treatment. (C) Number of rescue therapies per patient in the 24 months observation period. Differences between groups were assessed by two-sided Student’s t-test. (D) Change to cortisone dose at baseline at 12 and 24 months of treatment. Error bars display mean (95% CI). **p<0.01, *p<0.05, p≥0.05, not significant.
At 12 months, the rate of MM differed between the two groups with six patients achieving MM in the rituximab (n=56, 10.7%) and seven patients in the eculizumab treatment group (n=19, 36.8%; p=0.031, figure 3B). At 24 months, the effect persisted with seven patients reaching MM after rituximab (n=54, 12.9%) and seven patients after eculizumab treatment (n=19, 36.8%; p=0.015). One eculizumab patient and three rituximab patients were excluded from the analysis due to insufficient information regarding rescue therapies. The use of rescue therapies did not differ significantly between the rituximab and eculizumab groups as measured by the number of rescue therapies required for each patient during the 24 months observation period (number of rescue therapies per patient (SD) rituximab 2.20 (1.83), eculizumab 1.42 (1.81) p=0.073) (figure 3C). Lastly, both groups were able to reduce prednisone dose after treatment initiation (figure 3D). We detected no significant difference between the groups regarding the change to baseline prednisone dose at 12 months (prednisone dose at 12 months, mg (SD) rituximab 4.01 (4.90), eculizumab 5.30 (5.63), p=0.721) or at 24 months of treatment (prednisone dose at 24 months, mg (SD) rituximab 2.75 (3.67), eculizumab 3.17 (2.88), p=0.871).
Discussion
Clinical evidence is sparse in the therapeutic landscape of MG,20 but necessary to shape informed treatment decisions. To this end, we compared rituximab and eculizumab for treatment of refractory, generalised anti-AChR-ab positive MG. Eculizumab was more effective at ameliorating disease severity than rituximab as measured by QMG score after 12 and 24 months of treatment. Eculizumab-treated patients also achieved MM more frequently than rituximab-treated patients at 12 and at 24 months of treatment, while the risk for MC was comparable between both groups. Both groups were able to reduce average prednisone doses; however, no statistically significant difference was observed between the groups.
The role of eculizumab in the therapeutic landscape of MG is evolving as new evidence emerges. The REGAIN trial supports the use of eculizumab for refractory, anti-AChR-ab mediated MG.9 10 Despite not reaching the prespecified primary endpoint of change from baseline in the MG activities of daily living (ADL) score, post-hoc sensitivity analysis and secondary outcome measures demonstrated the efficacy of eculizumab in this patient collective.9 Analysis of the open-label extension reported that eculizumab’s effect was maintained throughout the 3 years of treatment.10 However, given its novelty and high cost, eculizumab remains reserved for cases with severe disease in current guidelines and direct comparisons to other therapies are lacking.21 Pathophysiological considerations might further strengthen the use of eculizumab as aberrant complement activation has been evidenced in humans and in animal models.22 Selective targeting of the complement cascade might therefore improve clinical outcomes while offering a beneficial profile of adverse effects.10 Consistent with this, data from our observational study underlines the efficacy of eculizumab as potential treatment option for refractory MG. It should be noted, that eculizumab is currently limited to anti-AChR-ab positive MG, which is mediated by IgG1 (and IgG3) subtype autoantibodies capable to activate the complement cascade. In contrast, MG mediated by pathogenic IgG4 subtype, for example, anti-MuSK MG, is unlikely to benefit from treatment due the lack of complement activation.23 By contrast, rituximab is efficacious in MG with anti-MuSK-ab as evidenced in a nationwide retrospective study.24 A shorter time to response might be expected for eculizumab in comparison to rituximab. Following infusion, complement is rapidly inhibited and therapeutic effects are seen as early as 3 days after treatment.25 Maximum efficacy is expected after 12 weeks of treatment as demonstrated in the REGAIN trial.26 As a general rule, rituximab effects are delayed for 6–8 weeks after infusion, and some patients require repeated cycles to achieve clinical benefits.27 28 Surprisingly, differences in treatment efficacy between the therapies persisted at 12 and 24 months after therapy initiation. Both treatment options carry a risk of severe infection, especially in combination with other immunosuppressants. Specifically, eculizumab is accompanied by an increased risk for meningococcal infections with approximately 0.1 events per 100 patient years,29 30 leading to obligatory anti-meningococcal vaccination before starting therapy.
Comparison between the two groups revealed no meaningful differences in the time to MC. With 10% and 16% of patients experiencing a MC during the 24 months observation period, the risk for MC remained high, underlining the need for intensified care and monitoring for patients with MG during a refractory course of disease.3 A potential explanation for the high rate for MC observed in both groups might be the frequency of infectious complications accounting for the majority of MC triggers. Treatment might dampen autoimmunity and improve symptoms, but not protect patients from infectious agents, resulting in disease flare-ups. However, the current sample size of eculizumab-treated patients might not be powered to detect effects on MC and prospective trials are required to better understand the long-term efficacy of eculizumab compared with established treatment strategies. In the open-label extension of the REGAIN trial, MG worsening occurred in ~13% and MC in 3% of patients in a time period of 22 months,10 indicating potential differences between study settings and real-world data. The current coronavirus disease 2019 (COVID-19) pandemic is a further factor shaping treatment decisions, as treatment agents such as rituximab increase the risk of hospitalisation due to immunosuppression.31 32 In contrast, data on the safety profile of ongoing eculizumab-treatment for COVID-19 is mostly lacking.
A limitation to this study is the retrospective, observational design, potentially introducing a selection bias for treatment decisions. In addition, limitations include data collection during routine clinical practice rather than a defined study setting. This might result in variances in data quality and quantity between patients. For example, the MG-ADL score was not routinely assessed during clinical practice and could not serve as an additional outcome parameter. Further, a conclusive definition for a treatment refractory status is currently lacking. For this study, we adapted a previously published definition of treatment refractory status as operational definition.3 However, we appreciate that the definition of treatment refractory disease at baseline, as employed for this study, is provisional until a consensus has been achieved for treatment refractoriness in the field of MG. The scope of our study is limited to the comparison of rituximab and eculizumab. Further studies investigating the efficacy of either agents against untreated patients in a real-world setting might be of scientific interest. Due to the clinical heterogeneity and rarity of the disease, MG has been historically difficult to study in the context of clinical trials.20 Thus, a strength of this study is the use of a well-defined MG cohort with high diagnostic certainty, providing novel data for treatment decisions for refractory MG. Moreover, data collection was standardised across participating centres in accordance with the German Myasthenia Gravis Register. Collectively, the results of this retrospective, observational study support the treatment of refractory, anti-AChR-ab MG with eculizumab and indicates certain advantages compared with rituximab in this subgroup. Based on our data, a randomised, prospective trial comparing rituximab and eculizumab in the setting of severe, generalised MG is required to establish the most effective treatment strategy for this disease course.
Data availability statement
Data are available upon reasonable request. All data relevant to the study are included in the article or uploaded as supplementary information. All analysed data are presented in the manuscript and available upon reasonable request from qualified investigators.
Ethics statements
Patient consent for publication
Ethics approval
The study was approved by the corresponding ethic boards (no. AZ 2020-010-f-S, no. AZ 07/2017, 19-8973-BO, AZ 21-1265, AZ 21-1331). Participants gave informed consent to participate in the study before taking part.
Acknowledgments
We thank the patients and their families for their valuable contribution and support.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
CN and CBS are joint first authors.
CN and CBS contributed equally.
Correction notice This article has been corrected since it was first published. The open access licence has been updated to CC BY.
Contributors CN, CBS and TR designed the study and methods. Formal analysis was done by CN and CBS. Clinical data were provided by CN, CBS, FS, MP, AG, HS, MS, BB, AT, TH, SS, SV, AM, HW, SGM and TR. Resources were provided by FS, AM, SGM and TR. CN and CBS wrote the original draft. FS, MP, LR-N, NM, AG, HS, MS, BB, AT, TH, SS, SV, AM, SGM and TR reviewed and edited the manuscript; Figures were created by CN and CBS. Supervision by AM, SGM and TR. Guarantor of the study is TR.
Funding PM is Einstein Junior Fellow funded by the Einstein Foundation Berlin, and is supported by grants from the Bundesministerium für Bildung und Forschung (grants no. 16GW0191 and NUM-COVID 19 – Organo-Strat 01KX2021).
Competing interests CN reports no conflicts of interest. CBS reports no conflicts of interest. FS received speaking honoraria from Biogen and Alexion. MP received speaker honoraria and travel/accommodation/meeting expenses from Novartis. LR-N reports no disclosures. NM reports no conflicts of interest. PM is on the Advisory Board of HealthNextGen and has equity interest in the company. His research is funded by the Bundesministerium für Bildung und Forschung (BMBF), the European Union, the Else Kröner-Fresenius Stiftung, the Volkswagen Stiftung and the Einstein Foundation Berlin. AG reports no conflicts of interest. HS reports no conflicts of interest. MS reports no conflicts of interest. BB received travel grants and/or training expenses from Bayer Vital GmbH, IpsenPharma GmbH, Norvartis, Biogen GmbH and Genzyme, as well as lecture fees from Ipsen Pharma GmbH, Alexion Pharma GmbH, Merck, Sanofi Genzyme and Roche. AT reports on conflicts of interest. TH received speaker honoraria and advisor honoraria from Alexion, Argenx, Biogen, Roche, Sanofi-Genzyme, Novartis and Hormosan. SS reports no conflicts of interest. SV reports no conflicts of interest. AM received speaker honoraria, consulting services and/or research support research from Alexion, argnx, GRIFOLS, Hormosan, Janssen, Octapharma, UCB and Vitaccess. He serves as chairman of the medical advisory board of the German Myasthenia Gravis Society. HW receives honoraria for acting as a member of Scientific Advisory Boards, Biogen, Evgen, Genzyme, MedDay Pharmaceuticals, Merck Serono, Novartis, Roche Pharma AG and Sanofi-Aventis as well as speaker honoraria and travel support from Alexion, Biogen, Cognomed, F. Hoffmann-La Roche, Gemeinnützige Hertie-Stiftung, Merck Serono, Novartis, Roche Pharma AG, Genzyme, TEVA and WebMD Global. HW is acting as a paid consultant for AbbVie, Actelion, Biogen, IGES, Johnson & Johnson, Novartis, Roche, Sanofi-Aventis and the Swiss Multiple Sclerosis Society. His research is funded by the German Ministry for Education and Research (BMBF), Deutsche Forschungsgemeinschaft (DFG), Else Kröner Fresenius Foundation, Fresenius Foundation, the European Union, Hertie Foundation, NRW Ministry of Education and Research, Interdisciplinary Center for Clinical Studies (IZKF) Muenster and RE Children’s Foundation, Biogen, GlaxoSmithKline GmbH, Roche Pharma AG, Sanofi-Genzyme. SGM receives honoraria for lecturing, and travel expenses for attending meetings from Almirall, Amicus Therapeutics Germany, Bayer Health Care, Biogen, Celgene, Diamed, Genzyme, MedDay Pharmaceuticals, Merck Serono, Novartis, Novo Nordisk, ONO Pharma, Roche, Sanofi-Aventis, Chugai Pharma, QuintilesIMS and Teva. His research is funded by the German Ministry for Education and Research (BMBF), Bundesinstitut für Risikobewertung (BfR), Deutsche Forschungsgemeinschaft (DFG), Deutsche Multiple Sklerose Gesellschaft (DMSG), Else Kröner Fresenius Foundation, Gemeinsamer Bundesausschuss (G-BA), German Academic Exchange Service, Hertie Foundation, Interdisciplinary Center for Clinical Studies (IZKF) Muenster, German Foundation Neurology and Alexion, Almirall, Amicus Therapeutics Germany, Biogen, Diamed, Fresenius Medical Care, Genzyme, HERZ Burgdorf, Merck Serono, Novartis, ONO Pharma, Roche and Teva. HW receives honoraria for acting as a member of Scientific Advisory Boards, Biogen, Evgen, Genzyme, MedDay Pharmaceuticals, Merck Serono, Novartis, Roche Pharma AG and Sanofi-Aventis as well as speaker honoraria and travel support from Alexion, Biogen, Cognomed, F. Hoffmann-La Roche, Gemeinnützige Hertie-Stiftung, Merck Serono, Novartis, Roche Pharma AG, Genzyme, TEVA and WebMD Global. TR reports grants from German Ministry of Education, Science, Research and Technology, grants and personal fees from Sanofi-Genzyme and Alexion; personal fees from Biogen, Roche and Teva; personal fees and non-financial support from Merck Serono, outside the submitted work.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.