Article Text

Abstract
Objectives Up to 40% of patients with idiopathic generalised epilepsy (IGE) are drug resistant and potentially could benefit from intracranial neuromodulation of the seizure circuit. We present outcomes following 2 years of thalamic-responsive neurostimulation for IGE.
Methods Four patients with pharmacoresistant epilepsy underwent RNS System implantation in the bilateral centromedian (CM) nucleus region. Electrophysiological data were extracted from the clinical patient data management system and analysed using a specialised platform (BRAINStim). Postoperative visualisation of electrode locations was performed using Lead-DBS. Seizure outcomes were reported using the Engel scale.
Results Patients experienced a 75%–99% reduction in seizure frequency with decreased seizure duration and severity (Engel class IB, IC, IIA and IIIA), as well as significant improvements in quality of life. Outcomes were durable through at least 2 years of therapy. Detection accuracy for all patients overall decreased over successive programming epochs from a mean of 96.5% to 88.3%. Most electrodes used to deliver stimulation were located in the CM (7/10) followed by the posterior dorsal ventral lateral (2/2), posterior ventral posterior lateral (3/4) and posterior ventral ventral lateral (2/3). In all patients, stimulation varied from 0.2 to 2.0 mA and amplitude only increased over successive epochs. The raw percentage of intracranial electroencephalography recordings with stimulations delivered to electrographic seizures was 24.8%, 1.2%, 7.6% and 8.8%.
Conclusion Closed-loop stimulation of the CM region may provide significant improvement in seizure control and quality of life for patients with drug-resistant IGE. Optimal detection and stimulation locations and parameters remain an active area of investigation for accelerating and fine-tuning clinical responses.
- epilepsy
- surgery
- electrical stimulation
- neurosurgery
- epilepsy
Data availability statement
Data are available on reasonable request. Deidentified data are available on reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution 4.0 Unported (CC BY 4.0) license, which permits others to copy, redistribute, remix, transform and build upon this work for any purpose, provided the original work is properly cited, a link to the licence is given, and indication of whether changes were made. See: https://creativecommons.org/licenses/by/4.0/.
Statistics from Altmetric.com
Key messages
What is already known on this topic
Responsive neurostimulation is an effective treatment for drug-resistant focal epilepsy and may be equally or more effective for drug-resistant idiopathic generalised epilepsy (IGE). The thalamus is an important node in IGE seizure networks and a potential target for responsive neurostimulation.
What this study adds
In this retrospective study of four patients with drug-resistant IGE, seizures were readily detected in the centromedian region of the thalamus and used to trigger closed-loop thalamic stimulation that dramatically reduced seizure frequency and severity.
How this study might affect research, practice or policy
A phase 3 clinical trial to study thalamic RNS for drug-resistant IGE is planned to begin enrolling in 2022.
Introduction
One-fifth of the approximately 3.4 million people living with epilepsy in the USA are diagnosed with idiopathic generalised epilepsy (IGE).1 2 Of those, about 10%–40% never achieve adequate seizure control with medication, with generalised tonic-clonic (GTC) seizures and myoclonic seizure types increasing the risk of drug resistance,3 resulting in significant detrimental impacts on quality of life and health.4–8 Unlike focal epilepsies, patients with IGE are not candidates for surgical resection and potential cure. Brain stimulation, however, is a surgical therapy that holds great promise for reducing seizure burden in patients with medically refractory IGE.
The potential for using electrical stimulation to abort seizures has been demonstrated since early intraoperative explorations by Penfield and Jasper.9 10 Likewise, the role of thalamic nuclei in generalised epilepsies has been a long-standing area of focus in both animal and human models, since the work of Hunter and Jasper, who showed that seizures could be induced by electrical stimulation of the thalamus.11 Subsequently, Monnier et al showed that medial thalamic stimulation could also desynchronise the cortical electroencephalography (EEG).12 As early as 1987, Velasco et al, motivated by the notion that cerebellar stimulation may be too diffuse to be effective, began exploring the centromedian (CM) nucleus as a target for chronic stimulation for IGE with excellent results.13–15 Subsequent feasibility studies and case series demonstrated equivocal findings, until a clinical trial by Valentin et al redemonstrated significant therapeutic benefit in patients with IGE.16 17 More broadly, the SANTE trial demonstrated the benefit of deep brain stimulation (DBS) of the anterior nucleus (ANT) for treating secondary generalisation of focal seizures.18 19
In contrast to traditional DBS, closed-loop brain stimulation uses programmable detection and stimulation to tailor therapy to a patient’s individual neurophysiology and has demonstrated reductions in frequency and severity of focal seizures that is superior to that of DBS or vagal nerve stimulation (VNS).20–23 The NeuroPace RNS System (RNS) is the only closed-loop device with Food and Drug Administration (FDA) approval for use in patients with focal epilepsy.24 25 Our previous case report of a single patient with IGE who received RNS in the CM region (CM-RNS) described significant reduction in seizure frequency and severity at 18 months.26 Here, we present 2-year outcomes for our initial series of four patients with IGE who underwent CM-RNS at a single centre.
Methods
Patient selection
Subjects had drug-resistant epilepsy, a consensus diagnosis of IGE, and had undergone thalamic RNS implantation following the recommendation of a multidisciplinary surgical epilepsy conference. Subjects were studied retrospectively via an institutional review board (IRB)-approved epilepsy surgery database for which they provided consent for inclusion. IRB review was not needed for implantation of RNS for generalised epilepsy, because the intention of off-label use was to provide the best potential treatment option for reducing seizures in these drug-resistant patients, based on the expert opinion of the multidisciplinary epilepsy team. Preoperative insurance authorisation was obtained for each surgery and no postoperative authorisation reversals occurred.
Surgical procedure
Under general anaesthesia, 4-contact depth leads with a contact length of 2.0 mm and intercontact interval of 3.5 mm (DL-330-3.5; NeuroPace, Mountain View, California, USA) were implanted using robotic stereotactic assistance (ROSA, Zimmer Biomet). The patients were positioned supine for transfrontal entry points, with head fixation using a Leksel stereotactic frame firmly attached to the robot chassis and coregistered by selecting points on a preoperative CT-based three-dimensional model of the Leksell frame.27 Indirect targeting of the CM nucleus of each hemisphere was used, with coordinates 10 mm lateral from the midline, 1 mm anterior to the posterior commissure (AC-PC), and 1 mm above the intercommissural line, consistent with previous studies.28 29
RNS system programming
Following implantation, the RNS was set to record intracranial EEG (iEEG) without stimulation in order to characterise baseline thalamic electrophysiology, prior to the initiation of stimulation.
Data analysis
Electrophysiological data were extracted from the NeuroPace Patient Data Management System using a custom-built platform (BRAINStim).30 Follow-up appointments were scheduled at approximately 3-month intervals for programming adjustments and monitoring. The percentage of seizure versus non-seizure stimulation was calculated from reviewed iEEG recordings. Cumulative stimulation, or cumulative charge duration, was calculated as charge density (µc/cm)×burst time (ms) by location.31 The average number of stimulations, long episodes (proxy for electrographic seizures) and detections (proxy for interictal activity) were calculated using daily detection counter data. Sensitivity, specificity and accuracy of detections and stimulations were calculated using reviewed iEEG recordings and extrapolated using a previously described method to adjust for temporal and selection bias.32 Piecewise linear regression of long episode counts per periods of stable detection and long episode configuration was performed to measure relatively trends in electrographic seizures. Postoperative visualisation of electrode locations was performed with Lead-DBS, using a postimplantation volumetric CT, a preimplantation volumetric MRI and the Morel atlas of the thalamus.33 34
Seizure outcomes
Clinical outcomes were derived by extended Personal Impact of Epilepsy Scale questionnaires and Engel scale. Although not developed to consider IGE cases, postoperative seizure control assessments were reported as Engel classifications,35 since a neuromodulation-specific surgical outcome scale has not yet been developed.
Results
There is no FDA-approved surgical therapy for IGE. Thus, diverging from the standard of care, which is continuation of medical management alone, was not taken lightly. In our first case described below, the patient had failed all available medical options and was offered but refused VNS, which although reported in the literature, is also off-label for IGE. In another case, the patient’s insurance would not authorise presurgical approval of VNS but did authorise RNS System therapy. The first patient was implanted in March 2018, and we reported her clinical indication and initial outcome previously.26 Her relatively rapid response, which appeared stable at 6 months postimplantation, encouraged us to implement a similar approach in three patients with subsequent IGE, all of whom have reached at least 2 years of continuous therapy. There were no surgical complications. The duration from RNS implantation to the most recent follow-up reported in this study was 24–33 months. Patient characteristics are listed in table 1, and per programming epoch detection and stimulation information is summarised in table 2.
Patient characteristics before and after RNS implantation
Detection and stimulation characteristics by programming epoch
As noted in our initial case report, the use of state-of-the-art techniques for lead localisation in a modern thalamic atlas demonstrated that use of traditional AC-PC coordinates resulted in lead implantations that are best described as being in the CM region. Electrode locations in this cohort were likewise determined to be in the CM, posterior (Po), ventral posterior medial (VPM), anterior ventral posterior lateral (VPLa), posterior ventral posterior lateral (VPLp), posterior dorsal ventral lateral (VLpd), posterior ventral ventral lateral (VLpv), intralaminar (Li), pulvinar anterior (PuA) regions of the thalamus or in white matter (WM). Given that this is the first reported case series of CM-region RNS for IGE, we describe each case separately below.
Patient 1
Patient 1 presented as a teenage girl with a history of eyelid myoclonia with absences (table 1). Seizures were incapacitating, averaging 1–4/hour (mean 60/day) and lasting 5–10 s without postictal effects. Ictal EEG was characterised by 3–5 Hz generalised spike and polyspike and wave discharges. Clobazam, ethosuximide, lamotrigine, levetiracetam, topiramate and zonisamide failed to control her seizures and/or provoked intolerable side effects. Treatment with valproate was not pursued because of the patient’s history of polycystic ovary disease and potential desire to become pregnant. Additionally, she declined the option of VNS, as she was an amateur singer who did not want to risk any potential voice side effects.
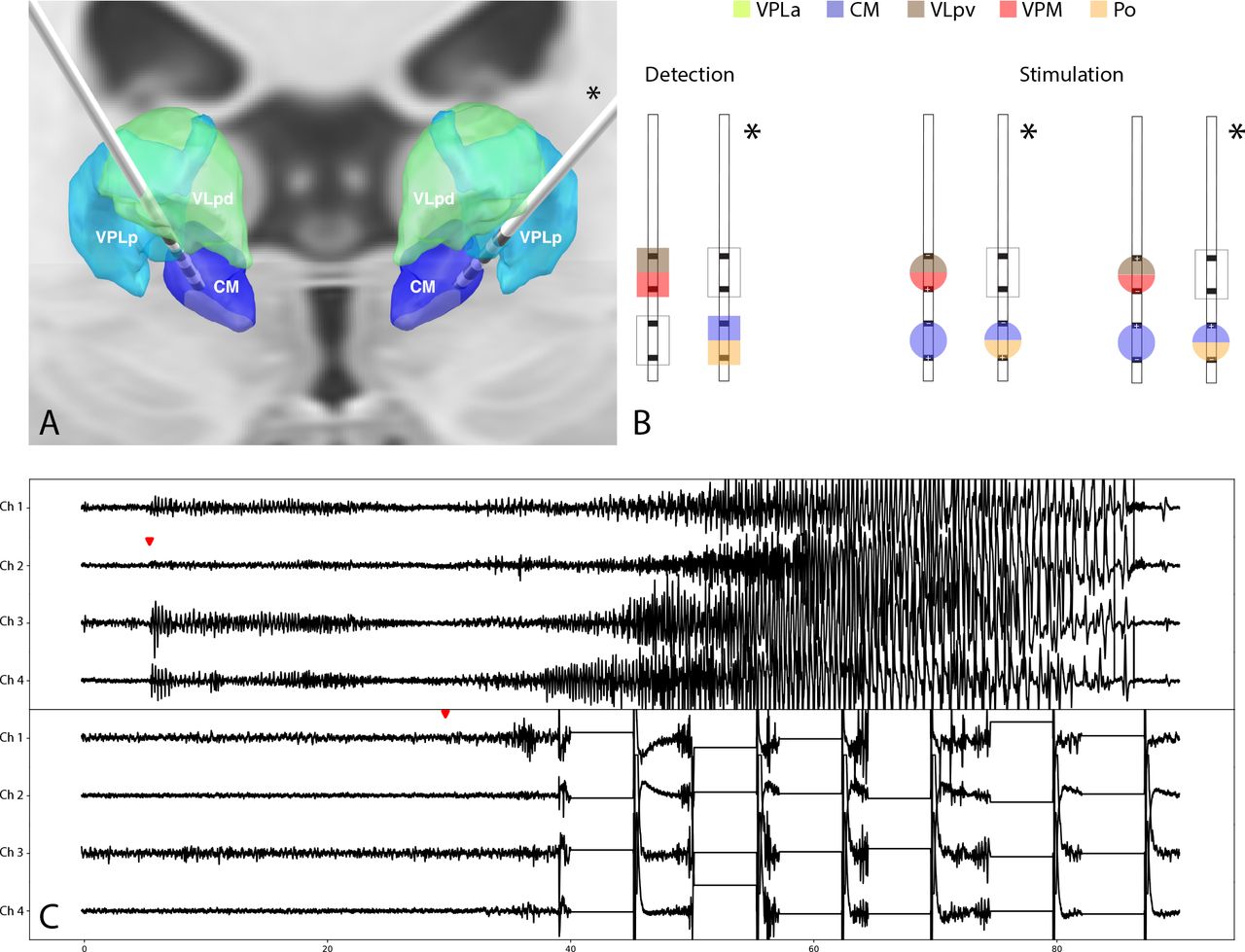
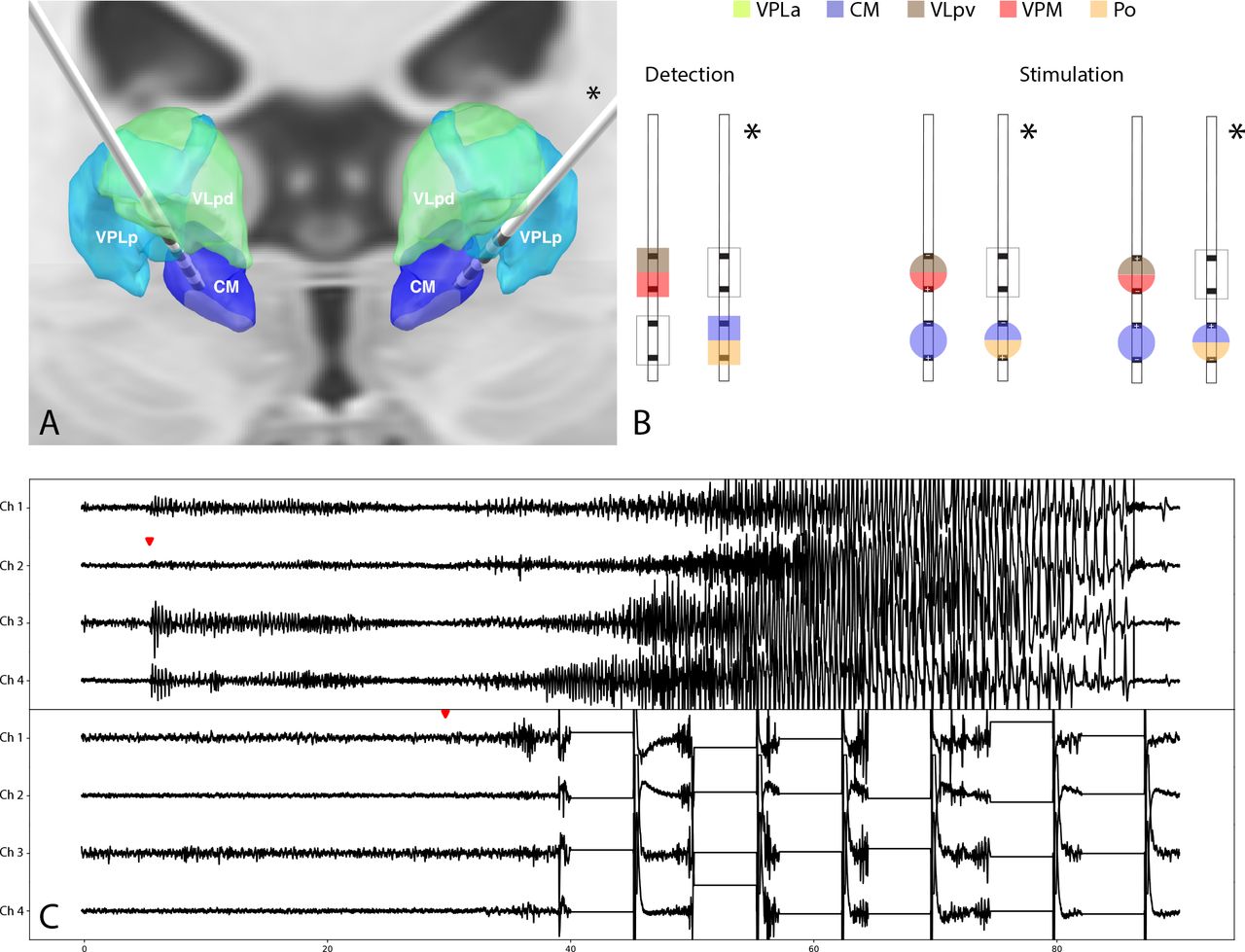
The baseline recording period (0–8 weeks) used line-length detectors on channels 1 (L-CM–L-PuA) and 3 (R-CM–R-VPLp) (online supplemental table 1). At 8 weeks, detection was modified to use bandpass filters on channels 2 (L-VPLp–L-VPLp) and 4 (R-VLpd–R-VLpd), and stimulation was enabled, also on channels 2 and 4, at 1.0 mA for up to five therapies composed of a single burst each (figure 1; online supplemental table 2). By 51 weeks, the detector was made slightly more sensitive and stimulation had been gradually increased to 2.0 mA (figure 1). Throughout the first 52 postoperative weeks, the patient reported a dramatic improvement in seizure control, in the setting of complete cessation of AEDs. Overall, the average daily number of therapies delivered was 130.2 (0–1120), with an average of 150.6 (0–2475) episodes and 4.7 (0–125) long episodes recorded (table 2).
Supplemental material

Implant localisations (A), detection and stimulation montage at most recent follow-up (B) and representative iEEG of electrographic seizure (C) baseline recording (top) and stimulated seizure (bottom) for subject 1. Asterisks (*) denotes patient’s left side. Detection and stimulation montages demonstrate the location of electrodes used for seizure detection and for delivery of stimulation. The amount of stimulation delivered (2.0 mA) is linearly scaled by circle radius for these schematic representations in figures 2–4, but is not the predicted VTA; for reference, VTA models predict approximately linear activation at 0.5–2.0 mA for axonal diameters of 3.5 μm.37 Red triangles indicate seizure onset and are placed above the channel used for detection. CM, centromedian; iEEG, intracranial electroencephalography; PuA, pulvinar anterior; VLpd, posterior dorsal ventral lateral; VPLp, posterior ventral posterior lateral; VTA, volume of tissue activated.
At her most recent visit at 144 weeks, she continues to experience stable reduction in seizure frequency and severity. Seizures now manifest as brief episodes of eyelid myoclonia without loss of consciousness, occur only a few times per week in the setting of stressful mornings, last only a couple of seconds and do not exceed 6/day (90%–99% reduction). In addition to this >90% reduction in seizure frequency, the patient also experiences periods of >48 hours without seizures. She reported a significant improvement in quality of life with improved mental concentration, which allowed her to obtain a full-time job, pursue independent living and acquire her driver’s license. She has not received any antiseizure drugs for over 1 year, following self-initiated medication cessation. Patient 1’s outcome corresponds to Engel class IB, as she no longer experiences disabling seizures.
Patient 2
Patient 2 presented as a man in his 20s with a history of absence seizure and GTC seizures. He also has a history of learning disability and migraines without aura, completed high school and was unable to drive. Phase I evaluation demonstrated bursts of generalised spike/polyspike and wave discharges with right predominance and determined that his diagnosis was IGE. Topiramate, levetiracetam, valproate, clonazepam, clobazam, zonisamide, oxcarbazepine/carbamazepine and lamotrigine failed to control his seizures and/or provoked intolerable side effects. Although he had recurrent nephrolithiasis on topiramate, he was unable to successfully taper off this medication despite repeated attempts. He had a VNS placed previously that caused him significant pain and vocal dysfunction, and it was replaced 82 weeks prior to RNS implantation. Preoperatively, seizure frequency was approximately daily (mean 3/week) on lacosamide, topiramate, clobazam and brivaracetam. These seizures would frequently cluster and he required intubation and admission to the intensive care unit five times in 6 months prior to the RNS implantation. His medications were initially continued postoperatively.
The baseline recording period (0–28 weeks) used combination of line length and bandpass detectors on channels 2 (L-VPLp–L-VLpv) and 4 (R-VPM–R-VLpv). Stimulation was enabled at 0.5 mA for up to five therapies comprising a single burst each at 28 weeks on channels 2 and 3 (R-WM–R-CM), and detection was modified to use a bandpass filter on channel 3 only. The detector was expanded to channels 2 and 3 at 37 weeks. By 118 weeks, stimulation had been gradually increased to 1.0 mA (figure 2). Overall, there was an average per day of 59.7 (0–451) therapies delivered, 320.0 (0–1007) episodes and 12.3 (0–94) long episodes.

Implant localisations (A), detection and stimulation montage at most recent follow-up (B) and representative iEEG of electrographic seizure (C) baseline recording (top) and stimulated seizure (bottom) for subject 2. The amount of stimulation delivered (1.0 mA) is linearly scaled by circle radius for these schematic representations in figures 2–4, but is not the predicted volume of tissue activated. Red triangles indicate seizure onset and are placed above the channel used for detection. Asterisks (*) denotes patient’s left side. CM, centromedian; iEEG, intracranial electroencephalography; PuA, pulvinar anterior; VLpd, posterior dorsal ventral lateral; VLpv, posterior ventral ventral lateral; VPLp, posterior ventral posterior lateral; VPM, ventral posterior medial (VPM); WM, white matter.
By 58 weeks, he had reported only one seizure and was able to wean off the brivaracetam and topiramate. At 110 weeks, he had a seizure in the setting of sleep deprivation (>4 hours/night for three nights) that required only 23-hour observation. At his most recent visit at 118 weeks, he continued to have significant reduction in seizure severity and frequency while taking only lacosamide and clobazam. He reports a significant improvement in quality of life and has been able to keep a job, maintain a romantic relationship and acquire his driver’s license. Patient 2’s outcome corresponds to Engel class IIA, as the patient has been experiencing rare seizures since surgery.
Patient 3
Patient 3 presented as a woman in her 20s with a history of juvenile myoclonic epilepsy with GTC seizures and absences. Ictal EEG was characterised by generalised, maximal right frontal, 2.5–4.5 Hz spike/polyspike-and-wave discharges. Prior to RNS implantation, she was reporting up to one convulsive seizure and few absences per week. Her seizures were poorly controlled with lamotrigine, zonisamide and levetiracetam. GTC seizures occurred 2–4 times/month while absence seizures few times per week and were severely debilitating. At the time of implantation with RNS, she was on lamotrigine.
The baseline recording period (0–8 weeks) initially used line length detectors on channels 1 (L-Po–L-CM) and 3 (R-CM–R-CM) which were subsequently switched to bandpass detectors on channels 2 (L-VPM–L-VPLa) and 4 (R-VPM–R-VLpv). Stimulation with 0.2 mA for up to five therapies comprising a single burst each was enabled on channels 2 and 4 at 8 weeks, and the detection channels were switched back to channels 1 and 3. At 60 weeks, the detector was switched to channels 1 and 4 and stimulation was reconfigured for up to five therapies comprising two bursts each with phase reversal. Stimulation was gradually increased to 0.7 and 0.8 mA and enabled on channel 3 at 100 weeks, and detector sensitivity was slightly decreased (figure 3). Overall, there was an average per day of 449.6 (0–1120) therapies delivered, 471.3 (0–1120) episodes and 15.7 (0–215) long episodes.
Implant localisations (A), detection and stimulation montage at most recent follow-up (B) and representative iEEG of electrographic seizure (C) baseline recording (top) and stimulated seizure (bottom) for subject 3. The amount of stimulation delivered (0.7 mA) is linearly scaled by circle radius for these schematic representations in figures 2–4, but is not the predicted volume of tissue activated. Red triangles indicate seizure onset and are placed above the channel used for detection. Asterisks (*) denotes patient’s left side. CM, centromedian; iEEG, intracranial electroencephalography; Po, posterior; VLpd, posterior dorsal ventral lateral; VLpv, posterior ventral ventral lateral; VPLa, anterior ventral posterior lateral; VPLp, posterior ventral posterior lateral; VPM, ventral posterior medial.
At her most recent visit at 107 weeks, she was taking only brivaracetam. Seizure frequency decreased to 1/month for the GTCs and were less severe, with a postictal recovery period of only 4–5 min. She no longer experienced absences. She reports significant reduction in seizure frequency of 75%–89%, length of individual seizures and duration of postictal state. Patient 3’s outcome corresponds to Engel class IIIA, as the patient had a worthwhile improvement in seizure control.
Patient 4
Patient 4 presented as a woman in her 30s, with a history of GTC seizures that surfaced after a motor vehicle accident. EEG studies demonstrated 3.5–4.5 Hz generalised spike/polyspike and wave complexes. The seizures acutely worsened in the months leading up to RNS implantation, with daily myoclonic seizures, and absences occurring weekly. VNS was considered but preauthorisation was denied by her insurance company. Phenytoin, valproate, topiramate, lamotrigine, levetiracetam and clonazepam failed to adequately control her seizures or provoked intolerable side effects.
The baseline recording period (0–11 weeks) used line length detectors on channels 2 (L-Po–L-CM) and 4 (R-CM–R-CM). Stimulation was enabled at 11 weeks with 0.5 mA for up to five therapies comprising a single burst each on channels 2 and 4, and detection was switched to a bandpass filter. Stimulation was gradually increased to 1.0 mA by 64 weeks, and the detectors were made slightly more sensitive at 87 weeks (figure 4). Overall, there was an average per day of 323.7 (0–1048) therapies delivered, 476.6 (0–1716) episodes and 3.3 (0–38) long episodes.

Implant localisations (A), detection and stimulation montage at most recent follow-up (B) and representative iEEG of electrographic seizure (C) baseline recording (top) and stimulated seizure (bottom) for subject 4. The amount of stimulation delivered (1.0 mA) is linearly scaled by circle radius for these schematic representations in figures 2–4, but is not the predicted volume of tissue activated. Red triangles indicate seizure onset and are placed above the channel used for detection. CM, centromedian; iEEG, intracranial electroencephalography; Po, posterior; VLpd, posterior dorsal ventral lateral; VPLp, posterior ventral posterior lateral; WM, white matter.
At her most recent visit at 104 weeks, she was taking valproate and topiramate. She continued to have myoclonic jerks with last disabling seizure at 20 weeks. She reported a significant reduction in seizure frequency of 90%–99%. Patient 4’s outcome corresponds to Engel class IC, as the patient has rare seizures since surgery.
Adjusted long episodes
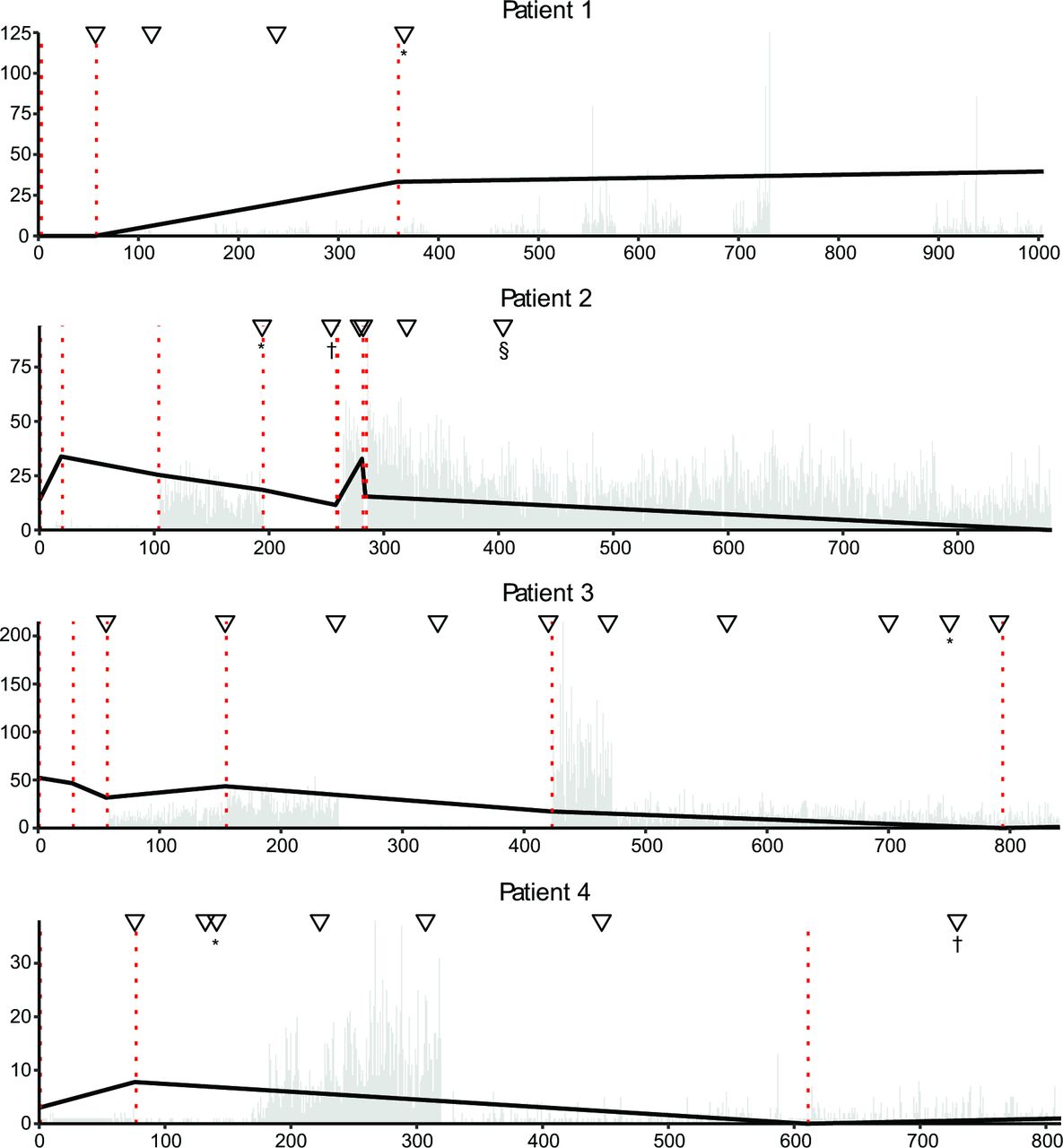
We next investigated whether patient-reported outcomes were reflected in the number of adjusted long episodes, which may be a proxy for seizure detections. Piecewise linear regression revealed a downward trend number of long episodes per day for patients 2 (−2.3×10−3/day), 3 (−5.4×10−3/day), and 4 (−9.8×10−4/day). Patient 1 had a positive trend of 9.3×10−4/day. Patient 1 was also missing data long episode counts for 42.1% (423) days as compared with minimal missing data for patients 2 (0.5%; 5), 3 (1.5%; 14) and 4 (1.8%; 16) (figure 5).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Electrographic seizure trend by detection programming epoch. Programming epochs were defined as periods of stable detectors and long episode configuration. The number of long episodes (episodes for which detection criteria were met for a preconfigured number of seconds) were used as a proxy for number of electrographic seizures. Daily total counts of long episodes were normalised for each programming epoch, and the trend was determined using linear regression. Vertical dotted lines denote a change in programming epoch. Labelled triangles mark significant events such as changes to stimulation and medications. Patient 1 events: *Off all AEDs. Patient 2 events: *Weaned brivaracetam and stimulation change; †Seizure requiring emergency department observation; §Weaned topiramate. Patient 3 events: *Only taking brivaracetam. Patient 4 events: *Last disabling seizure; †Only taking valproate and topiramate. ▽Represents changes to stimulation, unless otherwise marked. AEDs, antiepileptic Drugs.
Use of CM contacts in detection and stimulation
With regard to contact locations within the thalamus, across patients, electrodes resided in the CM (10), WM (5), VPLp (4), VPM (4), VLpv (3), Po (2), VLpd (2), PuA (1) and VPLa (1) regions. The CM was used for detection in 8/10 possible contacts located in the CM with initial programming, but only in 5/10 at most recent follow-up (table 3). The CM was used for stimulation in 5/10 possible contacts located in the CM with initial programming and in 7/10 at mostrecent follow-up.
Electrode locations for all patients by thalamic nuclei and regions
General detection and stimulation characteristics
Weighted detection accuracy varied from 0% to 100% (mean=81.1%; median=87.5). Unweighted accuracy (based only on manually reviewed recordings) differed significantly from weighted accuracy (88.4%–99.9%; mean=94.9%; median=95.5%). Detection accuracy for all patients overall decreased over successive programming epochs from a mean of 96.5% to 88.3%, with a corresponding increase in sensitivity of 28.0% to 58.8% and decrease in specificity of 99.2% to 89.0%.
Stimulation amplitude varied from 0.2 to 2.0 mA between patients and overprogramming epochs. In all patients, stimulation amplitude only increased over successive epochs. Total stimulation delivered varied between patients: 2.8×108 µc/cm/ms (patient 1), 2.1×108 µc/cm/ms (patient 2), 4.6×109 µc/cm/ms (patient 3) and 1.6×109 µc/cm/ms (patient 4). The raw percentage of iEEG recordings with stimulations delivered to electrographic seizures (true positive detections) was 24.8% (patient 1), 1.2% (patient 2), 7.6% (patient 3) and 8.8% (patient 4) (table 2). Patient 3 had 44.9% more stimulation delivered to the right versus left thalamus (3.2×106 vs 2.2×106), while the remaining patients had the same amount of stimulation delivered to both sides.
Discussion
We implanted the first cohort of patients with IGE to receive closed-loop thalamic stimulation and evaluated seizure outcomes over more than 2 years of therapy. CM-RNS produced a robust and durable therapeutic response in all patients in this cohort, by reducing both seizure frequency and severity, resulting in readily appreciable quality-of-life improvements. Two of four patients with previously intractable seizures obtained a driving license and were able to maintain full-time employment and long-term relationships. These results hold significant promise for over 2 50 000 patients with active, medically refractory IGE in the USA, who traditionally are not considered candidates for surgical therapy.
Adjusted long episodes
Piecewise linear regression revealed that long episodes, frequently assumed to approximate electrographic seizures and used to track patient response, decreased in three of four patients, consistent with their reported outcomes. We attribute the paradoxical small increase in long episodes observed in the first patient to the significant amount of missing data that resulted from her infrequent downloads. When sufficient data are present, this statistical technique to quantify patient-specific physiology may be useful in quantifying the therapeutic benefit of stimulation and detection settings, as well as changes to medications, as has been suggested for focal epilepsy.36
Stimulation location
Most electrodes used to deliver stimulation were implanted in the CM. Stimulation was enabled or disabled based on clinical efficacy and without prior knowledge of precise anatomical electrode location. This is consistent with our established rationale for CM implantation according to its established physiology.37 Given the variable response rates to stimulation of different thalamic nuclei, and their unique functional connectivity, the precise anatomic location target stimulation should be an important clinical consideration.38 However, there is no FDA-approved stereotactic targeting atlas that includes the CM nucleus, making surgical planning challenging. Note that subsequent to this cohort, we modified our CM targeting approach in line with that described by Warrant et al.39 In addition, correlation between the estimated volume of activation, outcomes and the structural and functional ‘connectome’ that is engaged by stimulation may be useful for elucidating optimal stimulation locations, an approach that has been used to evaluate targeting in DBS for obsessive compulsive disorder.40
Stimulation parameters
Patient 3 received approximately twice the amount of daily stimulation and 21 times the amount of total charge duration (µc/cm/ms) as patients 1 and 4, who achieved Engel class I outcomes. Patient 3 was also the only patient in this cohort with a second burst of stimulation programmed for every therapy, which reversed polarity. This contrast in delivery of stimulation and Engel classification may indicate that other stimulation characteristics, such as stimulation location, are more important than the quantity of stimulation delivered. The baseline values for the stimulation strategy used here, including frequency, amplitude and pulse duration, followed that of ANT-DBS.18 As such, we acknowledge that a vast parameter space remains to be explored. For example, stimulation in this cohort was uniquely delivered in bursts lasting 5 s, as compared with the 100–200 ms duration typical of neocortical or mesial temporal patients implanted with RNS. Large-scale analysis is needed to further optimise responsive thalamic-based network stimulation.
Detection location
The optimal location for the delivery of stimulation may not be the same as the optimal location for detection. Minimal mutual information, or unique features that differentiate seizure from non-seizure electrographic activity, is crucial for seizure detection. The number of non-CM detection locations that were maintained due to clinical efficacy suggests other brain regions may have more optimal characteristics for detection in some patients. In this cohort, the anatomic location and electrode combination needed to achieve the most accurate detections possible was determined empirically postimplantation. Ideally, further development of this treatment strategy would employ pre-RNS evaluation data to inform the most suitable anatomic location for electrode implantation.
Detection parameters
Overall, detectors were programmed to be less specific and more sensitive over successive epochs, resulting in an overall decrease in accuracy over time. This finding is corroborated by the decrease in percentage of true positive stimulation observed over time, as well. As a result, the amount of stimulation delivered tends to increase, while the number of events reported on the device also increases as an artefact of accuracy. This relationship is significant, given that the number of events is frequently used as a quantitative approximation of clinical response, and even small changes in detector accuracy can mislead clinicians, if not accounted for by applying the extrapolation and piecewise linear regression techniques we described.32
Limitations
This is a small case series which limits the generalisability of any findings reported. The vast parameter space of closed-loop stimulation and unique patient physiology present challenges for optimising detection and stimulation. These results, however, verify that ictal events can be detected rapidly in the thalamus of patients with IGE and suggests that CM-RNS therapy is safe, durable and quality-of-life improving.
Conclusion
Closed-loop stimulation of the CM region may provide significant improvement in seizure control and quality of life for patients with drug-resistant IGE. Optimal detection and stimulation locations and parameters remain an active area of investigation for accelerating and fine-tuning clinical response. A phase 3 clinical trial to study thalamic RNS as an adjunctive therapy for treating drug-resistant IGE in individuals ≥12 years old is planned to begin enrolling in 2022 (ClinicalTrials.gov Identifier: NCT05147571).
Data availability statement
Data are available on reasonable request. Deidentified data are available on reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
This human subjects research was classified as exempt from the Federal Policy for the Protection of Human Subjects by the Mass General Brigham IRB (Mass General Brigham Protocol No: 2020P000281), due to the minimal risk to subjects of extracting anonymised data from the clinical record. Participants gave informed consent to participate in the study before taking part.
Acknowledgments
We are grateful to these patients and their families, who entrusted our team to use our expertise to make the best possible recommendations for care.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @rmarkrichardson
Correction notice This article has been corrected since it was first published. The open access licence has been updated to CC BY.
Contributors Study conception and design: NDS, RMR; data collection: NDS, VK, AU; analysis and interpretation of results: all authors; draft manuscript preparation: NDS. All authors reviewed the results and approved the final version of the manuscript. RMR is responsible for the overall content as the guarantor.
Funding RMR reports grant support for closed-loop neuromodulation development from R01NS110424.
Competing interests RMR is a consultant for NeuroPace.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.